











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Based on treating principles, drug is referred to chemical substance which is employed to prevent or diagnose various diseases and disorders of body organs.1 Nowadays, considering the advancements obtained in various scientific fields, people are increasingly gaining access to various drugs. However, this facile access is turning into a detrimental social phenomenon, i.e. indiscriminate and inappropriate drug consumption. Indiscriminate drug consumption and totally self-medication are among the biggest social, health, and economical problems of different societies including Iran. According to the surveys, the drug prescription level does not match epidemiologic status of diseases in our country which can be caused by self-treating or self-medication in the society.2 Paulo and Zenini3) has defined self-medication as using a synthesized substance to treat or prevent a disease or to improve health without the prescription of and medical expert. Self-medication is not only prevalent in our country but also in other countries, leading to numerous side effects. Culture and people’s conception of drug is one the most important causes of self-medication. In other words, people like to have the doctor prescribe a great deal of drugs for them. On the other hand, people have their own reasons including having paid for the visit and transportation, having wasted time, and having left or interrupted their jobs. Hence, if the doctor does not prescribe any drugs for them, they will visit another doctor or try to consume drugs on their own, paving the path for the spread of self-medication in the country.4
Earlier research has showed that 83.3% of Iranians are used to self-medication.5 Common drugs in self-medication include antibiotics, pain killers, and injective vitamins. Inappropriate and arbitrary taking of antibiotics will contribute to the spread of bacterial resistance. Resistance to antibiotics would allow the infections that were thought to be treatable 15 years ago to emerge as main threats to public health again.6 An important factor in self-medication, which has been widely emphasized in different studies, is selling drugs without the doctor’s prescription.7 This will result in the factors including increased drug consumption per capita, resistance to drugs, lack of optimum treatment, poisoning, unexpected consequences, etc.8 Various studies have shown that women are particularly interested in self-medication, being unaware of its consequences.9 Hence, it can be concluded that even the pregnancy event in women can easily increase the consumption of drugs and chemical substances, while self-medication is responsible for more than 3% of congenital abnormalities. Especially, when the pregnancy is unintended and the mother is not aware of it, she will most likely keep on self-medicating.10 According to the results of some studies, self-medication during pregnancy can lead to uterine contraction.
The Strandberg’s survey revealed that this can increase the chance of premature pregnancy by 2-3 times and cause abortion or fetal abnormality.11 Also, taking some drugs during breastfeeding period can cause problems for the baby so that even arbitrary drug taking can cause problems such as fatigue and general weakness, sleepiness, the baby’s breathing difficulties, etc.2 Various studies have shown that self-medication among women is frequently aimed at treating problems such as dysmenorrhea (painful periods), eliminating menopausal symptoms, period disorders, osteoporosis prevention, and pregnancy and breastfeeding problems. For example, more than 70% of women are infected by vaginal fungal infection and 40%-5% of these infections will tend to reoccur in throughout their future life. All these factors would lay the groundwork for women’s tendency towards self-medication.12 According to the statistics, 30% of liver and kidney diseases are caused by taking drugs.7 Considering the increasing access to various drugs and the direct role of the individual in choosing and taking the drugs, people will need to obtain the required knowledge for changing behavior if they wish to a longer, healthier, and more active life.13 In line with achieving this goal, the studies indicate that identifying factors affecting behavior will facilitate changing the behavior. For this purpose, researchers have employed models to identify the factors affecting behavior.14) The models aim at contributing to the identification of the factors affecting the behavior and determining the way these factors function. These models also provide us with suggestions on how to affect these elements in various conditions. The Health Belief Model is an essential and exact pattern that is used to determine the relationship between health beliefs and behavior, and is also the most important model that is used in the development and design of prevention programs. According to this model, a person's decision and motivation to cultivate a particular behavior included items such as, Person's perception of being at risk (perceived susceptibility) and its seriousness (perceived severity), belief in the perceived action of usefulness to reduce the risk of illness, and understanding of the health benefits (perceived benefits) due to obstacles and moderating factors such as demographic and psychosocial variables (awareness). Cues to action also facilitate healthy behaviors.15 This model generally focuses on changing one's convictions and believes that changes in behavior can lead to changes in beliefs.16 Based on this model, people have to believe that they are prone to being hit by a phenomenon such as self-treating (understood sensitivity). Subsequently, they are expected to understand a benefit in terms of their behavioral change (not to self-medicate) and be able to overcome inhibitive factors including cost (perceived barriers). Considering the fact that self-medication is common among women and most of health centers do not offer enough education in this field or just rely on traditional education methods, being evidenced by an increase in self-medication per capita among women even during pregnancy, the present study has been carried out based on determining the effect of health belief model on the self-medication status of women in Fasa city.
Methods
The present study is a quasi-experimental study carried out among the women visiting health centers in the city of Fasa, Fars province, South of Iran. Among the six health centers in Fasa, two centers were randomly selected (one as the experimental group and the other as the control group). The sampling method in each health center was also random and performed based on the number of the household with health files in a center. In fact, they were gathered on a certain day in the health center and asked for their informed consent to participate in the survey. In the present study, the studied population includes all women without special who visited the health centers specified for sampling in the city of Fasa. The inclusion criteria included the women visiting the specified health centers for sampling in the city of Fasa who were not infected by any special diseases, while the exclusion criteria consisted of the unwillingness of women to keep on participating at the survey, absence for more than 1 to 3 sessions, and the incidence of special diseases for the sample during the survey. In this study, self-medication consists of arbitrary taking of any types of drugs (including herbal or chemical) without the doctor’s prescription and diagnosis. Figure 1 presents the study flow diagram.

The data collection instruments consist of questionnaires including six parts. Part 1 includes 9 demographic questions. Part 2 consists of knowledge questions including 10 4-choice questions (a correct answer in the knowledge section is scored 1, while the incorrect answer is scored zero). Part 3 includes 20 questions about sensitivity, severity, and the perceived benefits and barriers in terms of self-medication which have been designed as the 5-choice Likert scale. Part 4 evaluates different types of internal and external practice cues to action for self-medication by asking 2 questions. Part 5 is a checklist assessing the person’s performance in terms of self-medication during the past 3 months. And Part 6 investigates the causes of self-medication in people. At the end, each person’s score is calculated out of 100 through dividing the number of correct answers by the total number of all questions (10 questions) and multiplying the result by 100. In the section of sensitivity, severity, benefits, and the perceived barriers, the sensitivity amplitude of each question varies between 0 and 4 where the “I completely disagree” answer is scored zero, “I disagree = 1”, “I have no comments = 2, I agree = 3, and “I completely agree = 4. In general, the total score of each of these parts (sensitivity, severity, benefits, and perceived barriers) varies between 0 and 20. The obtained score of each one divided by 20 and multiplied by 100 will give the final score. In the performance checklist part, depending on the diseases for which the individual has self-treated, the participants score will be calculated out of 100. For this purpose, the number of diseases for which the individual has self-treated is divided by the total number of the mentioned diseases and the result is multiplied by 100 to give her score in the performance part. If she has self-treated in diseases other than those listed in the questionnaire, this part has been assessed through an open question (mention other necessary items).
The questions of internal and external practice guides as well as different types of self-medication have been calculated as self-medication. Questionnaire was designed by following preceding study.17) The reliability of the mentioned questionnaire was evaluated by the Cronbach's alpha method on 25 women who are demographically similar to the studied population, being obtained to be over 0.81 for knowledge, sensitivity, intensity, benefits, and practice. This value was calculated to be 0.84, 0.88, and 0.81 for sensitivity, intensity, and perceived benefits and obstacles. In the present study, the case and control groups will be selected to compare the effect of education using the health belief model (the experimental group) with traditional education methods in other centers (control).
Before the performance of educational intervention in both experimental and control groups, data was collected using the mentioned questionnaire then educational intervention for the experimental group was performed for 3 months. The experimental group was trained for four sessions in this 3-month period and each session lasted 60 minutes. The methods employed for education include giving speeches and holding group discussions. Educational matters and contents were prepared based on educational goals, the necessary must-learns about self-medication, and considering the needs assessment carried out ahead of the intervention and regarding the valid books and educational leaflets of the health ministry and Razi pharmaceutical journal as well as by consulting pharmacists.
The first session included getting familiar with the history of self-treating and increasing people’s knowledge in terms of self-medication. The second, third, and fourth sessions were also based on the health belief model including training for enhancing sensitivity, severity, and perceived benefits and barriers as well as the internal and external practice guide in terms of self-medication. It is worth to note that at the end of each session the pamphlet of the presented subjects are given to the participants Also, the subjects of the last sessions are briefly reviewed before the start of each session. 2 perusing sessions have been held for 1 to 2 months after intervention in order to review the presented participants and people received a short message about the consequences of self-medication how to preventing it. Finally, the data were collected from both experimental and control groups. Before starting the survey, the informed consent of participating in the study based on the resolutions of the ethics committee of the research council of the medical science University of Fasa was taken from the samples. In the present study, in addition to employing the chi-square tests to compare the mean score of knowledge, sensitivity, severity, and the perceived benefits and barriers before and after invention, the T-pair test was performed in each group, while the T-test was carried out between groups.
Results
The age average of the experimental and control groups were 42.16±2.81 (M±SD) and 40.86±3.16 years, respectively. In both groups, most women were married and employed. In this study, 75.55% and 71.11% of women were under the coverage of the health insurance system. Also, most women had high school level education and no meaningful difference was observed between the groups in terms of these variables (Table 1).
Table 1 Relative frequency distribution of the studied people in terms of marital status, occupation, education, and the health service coverage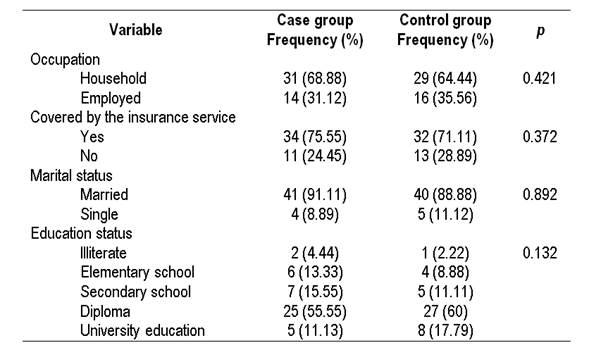
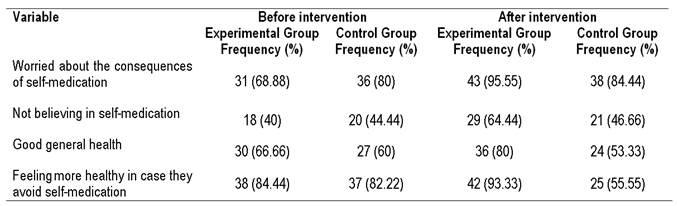
The score average of knowledge, perceived sensitivity, perceived severity, perceived benefits, perceived barriers, and perceived practice in self-medication in the both experimental and control group has been demonstrated in Table 2. The findings revealed that there is no noticeable difference between the groups before intervention in terms of the mentioned variables (p=0.461, p=0.135, p=0.235, p=0.215, p=0.411, and p=0.512), however, a meaningful difference (p=0.001) was observed between the two groups in all variables after educational intervention. Moreover, the results indicate that there is a meaningful difference between the score average of variables in the case group before and after educational intervention (p=0.001), while no meaningful difference was observed in the control group before and after intervention. All components of the health belief model were in relationship with women’s practice in terms of self-medication so that a reverse relationship was detected between the perceived sensitivity and practice (p=0.002 r=-0.47), the perceived severity and practice (p=0.003, r=-0.52), and between the perceived benefits and practice (p=0.022, r=-0.63) in terms of self-medicating. On the other hand, a direct and meaningful relationship was found between the perceived barriers about appropriate drug taking and self-medication (p=0.001, r=+0.84). The most perceived barrier in terms of appropriate drug taking among women includes their inadequate knowledge of proper drug taking. Also, the relative frequency distribution of the internal and external practice guides in both case and control group before and after educational intervention is presented by Tables and Table 4. No meaningful difference was observed between the two groups in terms of internal and external guides before the educational intervention, whereas a meaningful difference was found between the two groups in all internal and external practice guides 3 months after educational intervention (p=0.001).
Table 2 A comparison between the average knowledge scores, sensitivity, severity, perceived benefits and barriers, and practice in terms of self-medication before and 3 months after educational intervention between the experimental and control groups

Table 3 The frequency distribution of the internal practice guide in terms of self-medication upon the views of the studied population before and 3 months after educational intervention in the experimental and control groups

Discussion
Self-medication is one of the health problems requiring theory-based studies. The present study is aimed at determining the effect of educational intervention based on the health belief model on improving the actions preventing self-medication among 90 women visiting health centers in Fasa. In this study, the samples had achieved less than half of knowledge score before intervention. This level of knowledge can be attributed to notification by radio, television, newspaper, magazines, and books. Shamsi et al.17) carried out educational intervention between the two groups and found that there was a meaningful difference between all mentioned variables. The study also indicated a decrease in the mothers’ negative practice. These findings can effectively indicate the effect of educational intervention according to the health belief model as well as employing the advancing method of observational film viewing and offering free medical services on enhancing knowledge, perceptions, and the actions preventing self-medication.
A meaningful difference has been observed between the performance of the experimental and control groups in many of the other studies carried out based on the health belief model including: The survey of Shojaeizadeh et al.18) on cervical cancer, the study carried out by Wen et al. (19+) in terms of the effect of education according to the health belief model on bed rest for patients with deep venous thrombosis in China. The meaningful increase in the mean score of benefits, perceived barriers, self-efficacy and performance in the test group after intervention in terms of osteoporosis has been reported by Huang et al.20 for Taiwanese women. According to M. Zaki et al.21) study, most women had a positive attitude toward medications in general but they believed pregnant women should be more cautious regarding drug-use during pregnancy. The meaningful difference between the average knowledge scores of the case and control groups can be attributed to presenting training courses on avoiding self-medication which have remarkably enhanced the case group’s knowledge (35 scores) about the appropriate way of drug taking. The findings of this study revealed that the mean score of the women’s perceived sensitivity before educational intervention in both experimental and control groups was in the same moderate conditions, being in accordance with other study.17) As reported by Sereshti et al.,22) 91% of the studied units had a positive attitude towards herbal drugs. In the latter study, the existence of a meaningful difference after educational intervention between the experimental and control groups can be a good evidence of the effect of educational intervention on increasing the perceived sensitivity in the case group. After educational intervention, most women of the case group believed that they may be subjected to self-medication. This result is in accordance with the application of the health belief model and the perceived sensitivity for self-medication in Male High School Students.23
In terms of the perceived severity, both groups were in mediocre level of educational intervention. However, increase of the perceived severity mean score in the case group after educational intervention indicates the existence of a meaningful difference in the perceived severity between the experimental and control groups. In the present study, using the images of those who had been affected by self-medication consequences to demonstrate the seriousness of these consequences and to draw the samples’ attention to loss of health, the occurrence of other diseases, and high treatment costs are significant factors which increase the level of perceived severity of the samples. In terms of the benefits of lack of self-treatment, the findings of the present study showed that the perception status of people about the appropriate benefits of taking the drugs in both case and control groups before educational intervention is a bit higher than the average level. This value was remarkably increased after educational intervention in the case group (29 scores), the increase being 15 times greater in the experimental group than the control group. It seems as if the people’s attention to the fact that appropriate taking of drugs would mitigate the consequences and facilitate the improvement process can be effective in increasing the level of the perceived benefits. In the present study, the existence of a meaningful difference in the perceived barriers between the two groups after educational intervention is ascribed to the effect of educational intervention on eliminating the perceived barriers in terms of appropriate drug taking in the case group. In this study, most of the barriers perceived by women for proper drug consumption includes their inadequate knowledge of the appropriate way of taking drugs and the soundness of taking drugs, especially the herbal drugs. Karimy et al.24 have also suggested that the most important barrier against the proper way of drug taking is lack of time to see a doctor. In the present study and in terms of self-medication practice, both groups were above the average level before the educational intervention, while 31% of Tabriz citizens.25 In the present study, the mean score of performance in the experimental group meaningfully decreased after the educational intervention which can be attributed to the positive role of education based on the health belief model being in accordance with the Shamsi result.17 In the present study, the presence of an internal cues to action to encourage the individuals to proper use of drugs and also to enhance the participation of family members as the most important external guide in decreasing self-treatment is of great importance. In the study carried out by Neafsey et al.26) that about half of the participants (46%) achieved their information about drugs from the doctors and 41% form reading the label. Also, a limited portion of people (4%) used TV and 3% obtained their required information about the proper use of drugs from journals and friends.
Conclusion
The present study reveals that the educational planning should be focused on making women aware against perceived sensitivity and barriers. In this case, doctors, women, the health personnel, and media the most important information sources for women. Self-reporting of the behavior and performing the study by interview collection method is recommended in this study. Also, the lack of facilities and teaching aids as well as obtaining cooperation for performing the study were among the difficulties of the job. Finally, the study revealed that training through the health belief pattern plays an effective role in enhancing the sensitivity, severity, barriers, benefits, and self-efficacy of the studied women, causing them to take measures to prevent self-medication. Planning promotional interventions based on the health belief model along with the application of the media in order to promote actions preventing self-medication in women is recommended.

