











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkDear Editor,
Last year, a research group from South Korea used the National Health and Nutrition Examination Survey to study the relation between depressive illness and access to dental services. They found that people with depression are more likely to experience access problems rather than their counterparts, which leads -among other factors- to poorer oral health1. This finding was possible through Real-World Data (RWD) whose sources have been defined as the blocks that compose the Real-World Evidence (RWE) building. RWE is defined as “the clinical evidence regarding the usage and potential benefits or risks of a medical product derived from the analysis of RWD2.
To generate RWE, the available sources of RWD, such as Electronic Health Records (EHR), insurance bills, official registries of diseases, population surveys, among others, must go through three steps: obtainment, administration and depuration, and application. The latter include studies with different purposes (descriptive or analytic), approaches as observational and experimental, and designs as longitudinal cohort studies and clinical trials3 (Figure 1).
Advantages of RWE include the relatively large amount and scope of information, and its low costs which is appealing to researchers and stakeholders. However, some limitations are: technical (e.g. quality of information, interoperability of electronic sources), operational (e.g. lack of protocols to design and conduct studies), and cultural (e.g. trust among patients, institutions and stakeholders)3. In addition, there are ethical considerations entailing the use of personal data without explicit consent. In Latin America, other limitations for RWE are the low budgets of clinical and academic institutions, social inequity, and deficiencies in research skills of the professionals4.
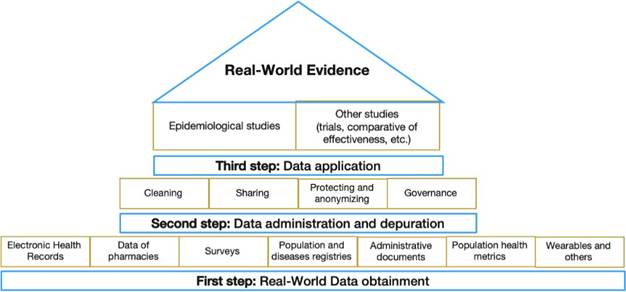
Source: by the authors
Figure 1 Real-world data and processes related with Real-world evidence construction
To describe the production of RWE in Latin America, we performed a search in PubMed and Scielo databases (August 2021). Due to the fact that there is not a MeSH term established, we used Real-world evidence OR Real-world data in the title. We retrieved 1,808 articles in PubMed, 37 from Latin America, and one in dentistry5. In Scielo, filtering by title for RWD only -because 1 article was retrieved if applying the filter for both RWE and RWD-, we retrieved 20 papers, 14 from Latin America and one in dentistry6.
Searching for RWD/RWE and dentistry (Query: ((Real-world data[Title/Abstract] OR (Real- world evidence[Title/Abstract]) AND (((Dentistry[Title/Abstract]) OR (Oral Medicine[Title/ Abstract])) OR (Oral Health[Title/Abstract]))) we retrieved two papers1,6, one of them discussed the relation between depressive illness and access to dental care, as mentioned above, and the other one was about the Practice Based Research (PBR) in dentistry. This latter concept is close but not an equivalent to RWE generation process.
To increase RWE in dentistry academic and clinical institutions, there is a need to be aware of RWE and facilitate training activities. There are current training and developing opportunities in the field as The Standardized In-Line Clinical Case Series methodology, which has been implemented in 14 countries and constitutes a “step forward for RWE in dental surgery”7.

