











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkThere is few epidemiological data on cutaneous melanoma (CM) in Latin America. 1,2 In Colombia, some studies have revealed a relative increase in its incidence in last years. 3-6 Although existing reports of melanoma characteristics show acral pattern as predominant, there is few information from private institutions regarding the characteristics of the population and the phototype. A better understanding of the disease could be achieved with additional studies and could promote early identification and diagnosis, besides relevant campaigns for the general population and the healthcare network.
The objective of this study is to describe the clinical, histopathological and treatment characteristics of melanoma in a private institution of reference for skin cancer, and to identify differences regarding sex and age.
MATERIALS AND METHODS
This is a retrospective study that includes 415 patients diagnosed with CM treated at a private institution of reference for skin cancer in Bogotá, Colombia (Dr. Alvaro Acosta de Hart IPS SAS), between January 1999 and May 2014. Clinical, histopathological and treatment data were collected from medical records in a proper database. In order to evaluate different variables, melanoma was staged in accordance with the guidelines of the American Joint Committee on Cancer (AJCC) 2009.
Clinical data (age, sex, phototype based on Fitzpatrick scale I-VI, lesion site, growth pattern, stage, number of nevus, atypical nevus), histopathological data (Breslow index, Clark level, ulceration, mitotic index, regression) and treatment data were assessed.
Regarding the statistical analysis, quantitative variables are described as mean ± standard deviation (SD) and qualitative data as numbers and percentages. In addition, patients were divided into two groups considering sex and age (≥65 and <65 years of age), and compared using the Chi-squared test, Fisher's exact test and ANNOVA test, as appropriate. A p-value of <0.05 was considered statistically significant. Data analysis was performed using the statistical program, Statistical Package for the Social Sciences (SPSS) version 21.
The study was approved by the Research Ethics Committee of the Faculty of Medicine of the Universidad Nacional de Colombia.
RESULTS
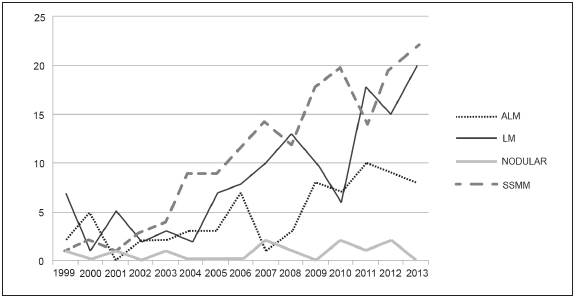
A total of 415 patients -244 (58.8%) women and 171 (41.2%) men- were included in the study, with a mean age of 56.1±16.2 SD (range 14-96) at the moment of diagnosis. A detailed description of the study population is reported in Table 1. The distribution of cases according to histological type per year of diagnosis is showed in Figure 1.
Table 1 Characteristics of cutaneous melanoma according to sex and diagnosed in a private institution of Bogotá, Colombia 1999- 2014

Mv: missing values. WLE: wide local excision. SMMS: Slow Mohs micrografic surgery; t: Data expressed as mean and standard deviation; μ: According to AJCC 2009; 1: Fisher's exact test.
Regarding the localization of disease, most melanomas were found in the head (n=165, 39.8%) and lower limbs (n=114, 27.5%). According to sex, a statistical significance was found (p<0.001) when comparing melanoma characteristics: melanomas located on the head were more frequent in men (n=83, 50.3%), but they were mainly found in the lower limbs in women (n=89, 36.8%).
Concerning growth pattern, superficial spreading malignant melanoma (SSMM) was found in 175 cases (42.7%), lentigo maligna (LM) in 138 cases (33.7%), acral lentiginous melanoma (ALM) in 75 cases (18.3%), and nodular melanoma (NM) in 12 cases (2.9%). Histological characteristics were assessed using Breslow thickness (the histology reports were done by a pathologist expert in skin cancer). A value less than or equal to 1 mm was observed in 310 patients (79.3%). A high number of cases presented with Clark I (n=196, 50.93%) and II (n=95, 24.7%). When comparing the growth pattern, LM was the most frequent among in situ MM (49.2%), while SSMM had the higher proportion of invasive MM (58.2%; p<0.001).
The distribution of melanoma cases related to phototype showed a predominance of type II (33.6%) and III (36%). In accordance with growth pattern, a higher frequency of I-II skin types was observed for SSMM (61.2%) and phototype Ill for LM (64.4%). The distribution of ALM by phototype showed that 33% of cases were type III, 28% were type II and 22% were type iv. Additionally, the absence of phototype VI was observed in this sample.
With respect to the treatment used, most cm were suitable for wide local excision (n=165, 78.9% in women; n=119, 79.9% in men) and an important percentage of cases were treated with slow Mohs micrographic surgery (SMMS), mainly LM and some ALM (n=40, 19.1% in women; n=28, 18.8% in men). Very few cases received treatment with radiotherapy, chemotherapy, interferon alpha or topical treatments. Atypical nevi were more frequent in men with melanoma than in women (n=22, 47.8% vs. n=14, 22.2% respectively, p=0.005).
When analyzing the characteristics of melanomas in relation to age (Table 2), a predominance of LM was observed among senior patients (>65 years) and a SSMM pattern among patients aged ≥65 years (p<0.001). In addition, a large number of melanomas located on the head were found in patients older than 65 years (p<0.001) and ulceration was mostly detected among these patients (p=0.046).
Table 2 Distribution of melanoma cases by age in relation to growth pattern, lesion site, Clark level and ulceration

MV: missing values. 1Fisher's exact test
An in situ vs. invasive melanoma analysis (Table 3) revealed significant predominance of SSMM and of photo types I and II in invasive melanomas (p<0.001), in contrast to LM and phototypes III, IV and V, as well as in situ melanomas (p=0.016). Furthermore, a high proportion of ulceration, mitosis, regression and advanced stages (III and IV) were observed in invasive melanomas (p<0.001).

DISCUSSION
Although data on the incidence and prevalence in developed countries are well known, there is few data in Colombia. A local report described an average incidence of 3.5/100 000 per year in men and 2.9/100 000 in women, with higher incidence and mortality rates among senior adults, particularly men. 7 Similarly, this study shows an increase of CM cases (Figure 1), probably caused not only by the global rise of this diagnosis, but to higher consultation by patients in the institution over time. Additionally, a higher preponderance of melanoma cases was found in men (58.8%).
Regarding growth pattern, an increased frequency of SSMM (42.7%) was observed in this study. Nevertheless, previous reports in Bogotá-Colombia, coming from a public institution, proved that ALM has the highest frequency with 43.7% 3, which is similar to results in Asian countries, Afro-descendants and Hispanic us populations. 8,9 This difference has been noted in some Latin American countries such as Brazil, which tend to disagree on predominant cm subtype, its incidence and mortality in the region regarding the data collected, possibly due to presence of miscegenation and high immigration rates. 1,10 As Colombia is considered a pluriethnic and multicultural state 11, the observed results could be explained by the fact that the sample is mostly composed of fair phototypes (86.4%; I - III Fitzpatrick phototype), which resemble more closely Caucasian populations in whom the SSMM pattern is predominant 12.
To our knowledge, this is the first study detailing phototypes for Colombian patients with a CM diagnose. Although it was not possible to obtain phototypes for the total study population, it is considered that the recorded data correspond to a representative sample that allows obtaining an indicator of distribution of skin types treated at the institution.
Interestingly, in this series, a great proportion of phototypes II and III correlates with ALM (61%). Although, this subtype of CM has been reported to be more frequent in dark phototypes 8, as detailed above, an important number of patients with fair skin phototypes was observed. Thereby, assessing other risk factors, for example being Hispanic as an independent factor to develop ALM, is desirable.
The literature has widely reported that location on lower limbs is more common in women 12, which correlates with the results obtained in this study, as 36.8% of melanomas were observed on lower limbs, followed by the head (33.9%). Nonetheless, a greater proportion of cm located on the head was found with 50.3% in men, as opposed to previous data which have reported a higher frequency of cm on the trunk 13. An association between older age and the development of lm on the head has been previously shown 14, which is confirmed by this study, presenting a statistical significance for a higher number of patients with cm on the head in patients over 65 years of age.
Regarding stage, a higher frequency for early stages and thin cm was found (47.2% for stage 0 and 37.4% for stage I; 49.4% in situ CM and 29.9% Breslow ≤1mm). In contrast, advanced stages have been observed in studies made by public institutions in Bogotá, with predominance of stage III and cm with Breslow >1mm (66.3%)3. Those disparities are probably caused by cases that are referred from tertiary care hospitals and different population environments. Other studies have established the variance between populations in private and public institutions 15; the latter may treat populations with a lower socioeconomic and educational level, whose access to health care is more limited, which could explain a higher Breslow and stage, and therefore their worst prognosis 16.
Differences between private vs. public healthcare have been observed also in the Chilean population in terms of ethnic, genetic and cultural conditions 15. The population that uses private clinics and has higher incomes is made up of about 20% of Amerindians and mainly Caucasian, while the population that uses public health care systems has a low socioeconomic stratum and is composed of 40% Amerindians and a darker phototype. This may suggest that ALM and a darker phototype is more frequent in patients using public health services, while SSMM and a fair phototype are more frequent in private practice.
In relation to atypical nevus, a statistical significance for a higher frequency in men compared with women was found in this work. The presence of atypical nevi and a higher number of common acquired nevus (30 or more) are associated with an increased risk of melanoma, as previously reported 17.
The analysis made by age at diagnosis showed a statistical significance for CM in >65 years of age with higher proportion of LM, located in the head, ulcerated and thick tumors. These findings resemble other previous French studies that found melanomas in people older than 60 years and were characterized by more frequent head and neck locations, a later stage at diagnosis, as well as a higher proportion of ulcerated, thick tumors and higher Breslow thickness 18. Analyses ≥40 or <40 years of age (data not reported in this work) have not found significant differences in frequencies by sex despite an increase of incidence in women younger than 40 years, which is probably related to a change in sun exposure habits and the increased use of tanning beds in this group 19.
A limitation of this retrospective study was that sample analyzed comes from a single private institution for skin cancer, with incomplete information in its clinical records, which did not allow evaluating some aspects of the population. Thus, data may not extrapolate to the entire population of the country. However, this study has the longest period of data collected and can be used to develop others studies in order to identify risk factors for melanoma development in Colombia.
In conclusion, this study reveals a divergence in frequency of a CM subtype in Bogotá, Colombia, and differences, in terms of age and sex, that may be related to demographic, ethnic and socioeconomic factors. In this study, CM cases were more common in men, with a mean age of 56 at diagnosis and high proportion of the SSMM subtype, as showed in reports of Caucasian populations. Regarding sex and location, it was more common on the head in men and on the limbs in women, with a predominance of fair phototypes.
The difference in CM presentation between public and private institutions raises the need to conduct further studies to understand better how socioeconomic and biological characteristics affect melanoma morbidity and mortality rates, which could improve early diagnosis and treatment, as well as the efforts of Public Health policies 

