











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkMental health disorders are growing at an alarming rate. According to the World Health Organization (WHO), 450 million people suffer from mental illnesses being the leading cause of disability worldwide 1. Also, beyond the negative impact on jobs, relationships, and families of those affected, studies have shown that mental diseases can decrease a person's life expectancy by 10 to 20 years.
Today, mental illnesses affect one in five young adults, where 50% are ill at the age of 14 and 75% by the age of 24 2. Mental diseases are a far-reaching health problem that can worsen since about 40% of the world population is less than 25 years, and it is estimated that this populace will peak in 20 years 3 (Figure 1).

Figure 1 shows that most people worldwide and Peruvians are in the age range with a high risk of suffering mental illnesses. As the natality rate falls, the current young adults will comprise the last mass population wave, becoming the majority in the future. Therefore, an accurate understanding of mental illnesses in young adults can help develop national educational policies or specialized training to eliminate (or at least mitigate) the proliferation of stress, anxiety, and depression (SAD) in the last worldwide working-age population.
Depression, an extreme form of recurrent melancholy and lack of vitality and concentration 4, affects more than 300 million people worldwide, and it is considered the leading cause of disability for individuals between 15 to 45 years old 5. Anxiety is related to chronic states of worry, fear, and guilt. It affects the person's capacity to make logical and moral decisions 4 and affects 264 million people worldwide 6. Likewise, stress is a response to pressure or noxious or aversive stimulus 7.
Early young adults are vulnerable to SAD due to puberty hormonal changes and their transition into adulthood (e. g., more responsibilities, exposure to new life events). Also, traumatic experiences such as losing a loved one or a parent's divorce can severely affect youngers' mental balance leading to SAD symptoms.
In low and middle-income countries, SAD cases are spreading fast, but data about demographics are unknown 8. In Peru, a middle-income country in South America, young people between 15 to 29 years are 28% of its total population 9. Nevertheless, few studies about SAD in younger university students are found; for instance, the INSM 10 reported mental illnesses in Peruvians from Lima but without specifying in what proportion SAD affects the life and well-being of younger adults and what are the stressors causing these mental diseases.
Most importantly, there is a strong link between mental diseases and suicide, which is the worst consequence of untreated SAD. Today, suicide is the second leading cause of death in people between 15 to 19 years old 11. Also, 15% of those that suffer from depression commit suicide 4.
In younger people in universities, a study from South Africa revealed that 24% of students had some form of suicidal idealization, and its predictors were post-traumatic stress and anxiety 12. Globally, several studies 13-20 have been done on SAD in university students (Table 1).
Table 1 SAD related studies (n=7)
| Studies | Country | Population | n | Stress (%) | Anxiety | Depression | Reported Stressors |
|---|---|---|---|---|---|---|---|
| Sarkar 14)1 | India | Medical students | 3882 | 39,2 | 34,5 | 51,3 | - |
| Singh 15)2 | Pakistan | College students | 400 | 52,7 | 86,5 | 59,2 | academic performance, parent love deprivation, family income, and course workload. |
| Aboalshamat 16)3 | Saudi Arabia | Medical students | 645 | 64 | 79,7 | 67,4 | Being a foreign, marital status, and clinical vs. interns. |
| Zou 17)4 | China | Male senior college students | 582 | 6,7 | 12,7 | 6,7 | an adverse interpersonal relationship, course workload, sudden life changes. |
| Cheung 18)5 | Hong Kong | Nursing and Mental Health students | 661 | 20 | 39,9 | 24,3 | income, exercise, entertainment, sleep quality, quiet time, family crisis, and diet. |
| Beiter 19)6 | USA | Undergraduate | 374 | 11 | 15 | 11 | Academic performance, success pressure, financial concerns, sleep quality, friends and family relationships, and others. |
| Kulsoom20)7 | South Arabia | Medical students | 431 | 41 | 63 | 43 | course workload and hectic schedule. |
Highlights: Study (1): Reported higher SAD in women. (2): A prevalence of anxiety in all students; co-morbidity of 39.5%; higher SAD in 17 to 19-year-old students; severe or extremely severe depression in 36.95% of male students. (3): Reported low self-esteem in 23.4%; and a negative relationship between self-esteem and SAD. (4): Reported 6.7% of adverse life events, and it was positively related to SAD. (5) Reported no significant relationship between gender and SAD and a negative relationship between age and anxiety. (6): Reported that students living off-campus had higher depression and anxiety as well as transfer students that also were significantly more anxious than non-transfer students. (7) Reported that students living with their parents and 4-year students reported the highest SAD; also, Saudi students and regular smokers reported high SAD.
As Table 1 shows, all studies used the DASS-21 to measure SAD symptoms in college students. Never-theless, they differ in some population characteristics, such as academic field and country of origin. Most studies are done with medical college students considering medicine as a stressful career 13 while neglecting other fields, such as Social Work.
The Social Work professional is usually the first line of defense in the industry and government agencies against most forms of social attrition. These overwhelming responsibilities plus the daily educational and social routines can lead to SAD, similarly to SWS in universities facing several responsibilities at the same time. Studies reported moderate stress in SWS 21 and depressive symptoms 22, but they did not use the DASS-21 to assess SAD.
Therefore, understating what sociodemographic and college stressors are related to SAD symptoms in SWS in Peru is of vital importance.
In this context, the contributions of this study are: (a) data about stress, anxiety, and depression in SWS; (b) three models of association of sociodemographic and college stressors with each SAD illness, (C) validation of the DASS-21 Spanish version and optimizations for Spanish students, and (d) the report of the Peruvian SWS profile.
METHODOLOGY
Participants and instrument
Our sample is composed of 152 SWS from the Universidad Nacional del Altiplano in Puno, Peru. We used a self-administered, pre-tested, online, anonymous questionnaire and a paper-print version of the questionnaire. For the paper-print version, we allowed 15 minutes to explain the purpose of the study and reiterate the anonymity of the answers. On average, the students used 34 minutes to fulfill the questionnaire. In total, 204 questionnaires were received, but 52 were excluded for being incomplete or non-legible.
The questionnaire had two parts. The first measured SAD symptoms using the DASS-21 scale, a 21 questions tool that asks students about their previous seven-day experiences. Each question used a scale ranging from 0 to 4; for example: (0) represents:
"Did not apply to me at all - never," and four (4) represents: "Applies to me a lot, or most of the time - almost always."
The DASS-21 is a reliable and well-known psycho-logical instrument that measures SAD symptoms in different populations, including young adults in universities. It has the same efficiency and provides similar results to the DASS-42 (its complete version) but using fewer questions 23.
We used the DASS-21 Spanish version from the study of Daza 24. The pre-test required modification from the original DASS-21, mainly to change the phrase "Me aplicó" to "Me afecto"; thus, the original "0 = No me aplicó, changed to 0 = No me afectó" and so for all cases. This change was made to adapt to the Peruvian Spanish.
The second part of the survey collected SWS socio-demographic data and the perceptions on university stressors such as academic semester and workout frequency (Table 2). We developed the questionnaire, carried out the pre-test stages, data collection, and data analysis from August 2018 to February 2019.
Table 2 Sociodemographic student's data (n=152)
| Frequency | % | ||
|---|---|---|---|
| Age | Between 16 to 25 | 138 | 90,8 |
| Between 26 to 44 | 14 | 9,2 | |
| Gender | Female | 137 | 90,1 |
| Male | 15 | 9,9 | |
| Academic semester | 1st and 2nd semesters | 9 | 6 |
| 3rd and 4th, semesters | 35 | 23 | |
| 5th and 6th semesters | 23 | 15,1 | |
| 7th and 8th semesters | 37 | 24,3 | |
| 9th and 10th semesters | 42 | 27,6 | |
| Grad school or certification | 6 | 4 | |
| Live with | Live alone | 50 | 32,9 |
| Live with partner | 10 | 6,6 | |
| Live with parents or relatives | 92 | 60,5 | |
| Workout | I do not do exercises; I am always busy | 79 | 52 |
| I exercise from 1 to 3 times a week | 42 | 27,6 | |
| I exercise inter-day | 28 | 18,4 | |
| I exercise every day | 3 | 2 | |
| Smoke consumption | No, I do not smoke | 140 | 92,1 |
| Yes, I smoke occasionally | 12 | 7,9 | |
| Alcohol consumption | No, I do not drink | 105 | 69,1 |
| Yes, I drink occasionally | 47 | 30,9 | |
| Final tests | It is easy | 32 | 21,1 |
| It is not easy, and it is stressful | 120 | 78,9 | |
| Homework | It is easy | 66 | 43,4 |
| It is not easy, and it isstressful | 86 | 56,6 | |
| Presentations | It is easy | 76 | 50 |
| It is not easy, and it is stressful | 76 | 50 | |
| Resolve doubts with professors | It is easy | 68 | 44,7 |
| It is not easy, and it is stressful | 84 | 55,3 | |
| Attendance | It is easy | 125 | 82,2 |
| It is not easy, and it is stressful | 27 | 17,8 | |
| Social Media | I do not use any social media | 1 | 0,7 |
| I rarely check my social media | 36 | 23,7 | |
| I frequently check my social media | 91 | 59,8 | |
| I am always checking my social media | 24 | 15,8 |
In the sequence, we performed the factor analysis technique over the 21 indicators of the DASS-21. We confirmed that stress, anxiety, and depression are three independent factors, and each of them is correlated to seven specific indicators each (Table 3).
Table 3 SAD factors and their correlated indicators
| Extraction | Component | DASS-21 indicators | |
|---|---|---|---|
| S-1 | 0,4 | 0,6 | I found it hard to wind down |
| S-6 | 0,4 | 0,6 | I tended to over-react to situations |
| S-8 | 0,5 | 0,7 | I felt that I was using a lot of nervous energy |
| S-11 | 0,5 | 0,7 | I found myself getting agitated |
| S-12 | 0,6 | 0,8 | I found it difficult to relax I was intolerant of anything that |
| S-14 | 0,6 | 0,7 | kept me from getting on with what I was doing |
| S-18 | 0,5 | 0,7 | I felt that I was rather touchy |
| A-2 | 0,4 | 0,6 | I was aware of the dryness of my mouth |
| A-4 | 0,4 | 0,7 | I experienced breathing difficulty |
| A-7 | 0,6 | 0,8 | I experienced trembling (e.g., in the hands) |
| A-9 | 0,6 | 0,7 | I was worried about situations in which I might panic and make a fool of myself |
| A-15 | 0,6 | 0,8 | I felt I was close to panic |
| A-19 | 0,6 | 0,8 | I was aware of the action of my heart in the absence of physical exertion |
| A-20 | 0,5 | 0,7 | I felt scared with19 out any good reason |
| D-3 | 0,4 | 0,6 | I could not seem to experience any positive feeling at all |
| D-5 | 0,3 | 0,5 | I found it difficult to work up the initiative to do things |
| D-10 | 0,7 | 0,8 | I felt that I had nothing to look forward to |
| D-13 | 0,6 | 0,8 | I felt downhearted and blue |
| D-16 | 0,4 | 0,6 | I was unable to become enthusiastic about anything |
| D-17 | 0,7 | 0,8 | I felt I was not worth much as a person |
| D-21 | 0,7 | 0,8 | I felt that life was meaningless |
We used the Kaiser-Meyer-Olkin (KMO) test to measure the sampling adequacy and Bartlett's Test of Sphericity to measure the homogeneity of each SAD factor. Also, we calculated the Extraction Sums of Squared loading with an orthogonal rotation varimax technique to detect the total variance accounted for each SAD factor. Finally, we plotted graphs for each SAD factor.
We converted all sociodemographic categories into dichotomous values. Next, we used multiple regression to analyse the relationships between sociodemographic and college stressors over stress, anxiety, and depression, respectively. We calculated the R-square (R2) to support the relationships proposed in each of the three models. To support the significance of each model, we perform the ANOVA and the t-student tests. Finally, we accepted a (p<0,01) as statistically significant of the relationships proposed to stress and depression and a (p<0,05) to anxiety.
RESULTS
Sociodemographic data
Of the 152 Peruvian SWS, 137 are female and 15 males. Also, 91% of all are between 16 to 25 years old. Moreover, 61% of them live with their parents or relatives. Also, 51,9% of SWS are in the 7th, 8th, 9th, or 10th academic semesters. Notably, 52% of SWS stated they are always busy, so they do not practice any physical activity. Besides, 99% of them are a participant of at least one social media platform. In this sample, 92% of SWS do not smoke, and 69% do not consume alcohol (Table 2).
We also found that 79% of all SWS consider final tests as a stressful academic requirement. Also, 55% of all stated that talking with their professors about academic doubts is challenging. Moreover, 50% of the SWS stated that performing classroom presentations is a stressful activity. Also, 57% of all consider doing homework as a taxing duty, and 82% said that attending college is not difficult.
The factorial analysis over the DASS-21 shows the association of stress, anxiety, and depression with seven specific indicators each and their respective weights (Table 3).
In Table 3, the column extraction shows the results of the commonality test, and the column component shows the weights of each indicator associated with each SAD factor. This study is the first to show sociodemographic and college stressors in SWS from Peru; then, we consider Ringle's 25 criteria about maintaining indicators with 0,7 or higher weight and those with a lower weight to preserve the model's reliability.
We also perform the KMO and Bartlett's tests to validate the usefulness of the factor analysis over each SAD factor (Table 4).
Table 4 SAD factor analysis outcomes
| Stress | Anxiety | Depression | |
|---|---|---|---|
| Kaiser-Meyer-Olkin Test (KMO) | 0,8 | 0,9 | 0,8 |
| Bartlett's Test of Sphericity | 0,0 | 0,0 | 0,0 |
| Total variance Explained (% of variance) | 49,8 | 52,4 | 53,7 |
The outcomes of the KMO test for each SAD factor support that our sampling is satisfactory and adequate for factor analysis 26. Bartlett's test results (Sig=0) support a strong correlation between seven specific DASS-21 indicators with each SAD factor. Moreover, the Extraction Sums of Squared Loadings found in this sample support a variation of 50% for stress, 52% for anxiety, and 54% for depression.
The outcome of the multiple regression in the model of stress shows that it is statistically significant (p.<0,001). The R2=0,16 means that the independent variables age, academic semester, grad school or certification, and class-room presentations explain 16% of stress variation but with different magnitudes.
The most significant and positive predictor of stress was the 6th and 5th academic semesters (t=3,31, p=0,001). It followed by the 4th and 3th semesters (t=3,15, p=0,002); 10th and 9th semesters (t=2,83, p=0,005); 8th and 7th semesters (t=2,76, p=0.007); grad school or certification (t=1,84, p=0,068); and classroom presentations (t=1,84, p=0,067). The only negative predictor was age (t=-2,95, p=0,004) (Figure 2).


The outcomes of the multiple regression also support that the anxiety model is statistically significant (p<0,005). The R2=0,14 reveals that the variables age, final tests; academic semester; grad school or certification; and classroom presentations explain 14% of anxiety variation.
In the anxiety model, age was the most significant and negative predictor (t=-2,72, p=0,007). It was followed by the positive predictor classroom presentations (t=2,23, p=0,027); 6th and 5th academic semesters (t=2,03, p=0,044); 4th and 3er semesters (t=1,96, p=0,053); final tests (t=1,77, p=.0,78); 8th and 7th semesters (t=1,68, p=0,094); 10th and 9th semesters (t=1,44, p=0,151), and grad school or certification (t=1,70, p=0,092) (Figure 3).
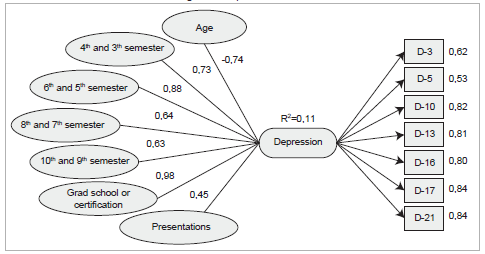
The depression model also was found statistically significant (p<0,005). The coefficient R2 shows that the variation in depression could be explained in 11,3% by the variables age, academic semester, grad school or certification, and classroom presentations.
In this model, the most significant and positive predictor was classroom presentations (t=2,82, p=0,006). It was followed by 6th and 5th academic semesters (t=2,29, p=0,023); 4th and 3er semesters (t=2,01, p=0,046); 8th and 7tthsemesters (t=1,78, p=0,077); 9th and 10th semesters (t=1,76, p=0,080); and graduate school or certification (t=1,69, p=0,093). The only negative predictor in the model was age (t=-2,23, p=0,027) (Figure 4).
DISCUSSION
This study evidence the profile of SWS from Peru, which is composed mostly of female students. Most are between 16 to 25 years old. More than 50% of all students are in their fourth or fifth year of study. Besides, more than 60% of SWS live with their parents or relatives, and 52% do not exercise. Also, 92% of SWS do not smoke, 69% do not consume alcohol, and 99% of them are active users of at least one social media.
In this study, we confirm that SAD is impairing the mental health and well-being of SWS from Peru. It was found that 48% of SWS are suffering from at least one SAD mental disease, while an extremely high 79% of them report moderate to severe rates of SAD. The study's results contribute to international studies that, similarly to this study, found high SAD symptoms in university students from different academic majors and different countries 14-20.
The study's result confirms that some academic stressors are common between fields and can accelerate SAD symptoms in young university students. Past SAD studies found that these mental illnesses affect more women than men students 13. Our study also supports these findings since we evidenced that female SWS in Peru suffers from moderate to severe SAD. This result calls for more studies testing new college stressors related to SAD. Also, this data can help university authorities to develop academic policies to prevent or mitigate SAD.
In this study, stress symptoms were associated with the academic semester. SWS in the third year reported more stress than those students writing their thesis in the final year. Also, older-aged SWS were less affected by stress than their younger peers. We recommend new studies that explore the curriculum of SWS from Peru to understand better the academic requirements for third-year students and how to mitigate sources of stress in this academic year.
The study also shows that symptoms of anxiety are negatively related to student's age. Thus, older-aged SWS tackle better feelings of anxiety than their younger peers. Also, anxiety increased when SWS are required to perform classroom presentations. Similarly, symptoms of depression were associated with classroom presentations. Also, higher depression was found in the third year, and older-aged SWS were less affected by depressive symptoms than their younger peers.
In the study, the academic stressor classroom presentation was associated with stress, anxiety, and depression. Thus, we recommend the Social Work School authorities assess the viability of an introductory seminar for students to learn techniques to perform public presentations. We hypothesized that a significant exposure of students to presentation techniques since the beginning of their journey in the university could decrease SAD symptoms. However, further research is needed to validate this assumption.
The evidence suggests that some academic stressors increment SAD symptoms in SWS (see results section). Some studies suggest 27,28 that stress in moderate levels and specific scenarios (e.g., presentations) can also play a positive role in students' learning process and character formation. Nevertheless, identifying when and what are the primary causes of stress in SWS could help professors devise plans to mitigate its adverse effects on students' mental health and academic performance.
In this study, we did not find a significant statistical relationship between the academic stressors living situation, workout, smoke consumption, alcohol consumption, use of social media, resolve academic doubts with professors, and attendance with any SAD illness.
We validated the DASS-21 Spanish version, using factorial analysis and displaying the correlated indicators and weight for each SAD factor. The analyses revealed a potential weakness in the DASS-21 questionnaire (see methodology section). Future studies using factorial analysis over the DASS-21 in different languages and new samples of SWS from different countries are needed to validate these findings and guide future DASS-21 improvements.
Finally, it is also important to mention that undergrad students from Peru do not have major or minor once they graduated, which is different from countries like the United States. The field is chosen apriori, and they must complete a fixed number of courses in an academic period of five years. The SWS in this sample spans only for those that aimed to become Social Workers and differs from studies such as Wahler 29, in which it was not possible to specify if the students were aiming only for a minor in Social Work.
Limitations
First, the study has an intentional sample and partially portrays the reality of this population. Thus, the paper's conclusions cannot be directly generalized and are specific to this sample. Second, there is a lack of validation with precedent studies about SAD in SWS using the DASS-21. Lastly, since the data was collected with self-reports through an online questionnaire, we cannot assert any information about the student's context and how it could have affected their answers *

