











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Violence is an important public health problem and one of the main causes of death worldwide. Each year, 1.7 million people lose their lives to violence and a considerable proportion suffer non-fatal injuries as a result of either self-inflicted, collective or interpersonal violence. Included in the latter is intimate partner violence (IPV), which is carried out by a member of a current or previous intimate relationship.1 According to the World Health Organisation (WHO), 1 in every 3 women world-wide has experienced physical or sexual violence, which was predominantly conducted by their partner.2 Out of the 50 000 registered cases of IPV in Colombia in 2018, 86% were against women (43 000 cases), with a rate of 204/100 000 women. Cali, with 2100 cases, was the city with the second highest number of cases in Colombia.3
While the prevalence of IPV varies greatly between countries due to contextual factors, measuring IPV and comparing data across countries is also a challenge. Some of the differences in prevalence and the level of severity of IPV reported by women in different countries may be partly explained by the definitions of IPV used, the instruments used to measure it and the methodological designs of each study. For example, studies from around the world quote different prevalences of IPV: the United States of America, 64%;4 Egypt, North Africa, 29%5, and Ghana, West Africa, 50%.6
IPV is a complex event that can vary depending on personal factors, such as age and character and on con-textual factors which include situational and sociocultural factors.7 Contextual factors include family dynamics and eco-nomic dependence. Survivors of IPV also experience ill-health effects at an individual level and their functioning in society is impaired. Previous studies from different contexts have reported that IPV is associated with an increased risk of depressive symptoms, depression, PTSD and anxiety.8)-(12
IPV is a systematic behaviour that can be explained by the theory the cycle of abuse of IPV that consists of three interdependent phases: tension building, episode of aggression and the honeymoon. This violence has consequences on the survivors coping mechanisms associated with self-care, work, interpersonal relationships, and other areas.13
Mental health consequences of experiencing IPV can lead to deliberate self-harm and suicide.14)-(16 Unhealthy habits have also been observed such as alcohol abuse, smoking, the transmission of sexually transmitted diseases17 and physical injuries. A meta-analysis identified that the prevalence of depression in female survivors of IPV was approximately 48% and PTSD was between 24% and 84%.18
The 2015 Colombian National Survey of Mental Health reported that 9% of the 3463 women interviewed, aged 18 to 44 years old, had a traumatic experience due to domes-tic violence. Of these women, 57% stated the nature of it was psychological violence, 71% physical violence and 27% sexual violence. In women above 45 years old, 7% of3023 subjects had a traumatic experience due to domestic violence and the figures were similar in relation to psychological (72%), physical (77%), and sexual violence (32%).19
IPV affects a women's quality of life as it is associated with different levels of disability; a concept defined by the WHO in its publication: The International Classification of Functioning, Disability and Health (ICF). They define disability as "an umbrella term for impairments, activity limitations and participation restrictions" and explain how "disability and functioning are viewed as outcomes of interactions between health conditions (diseases, disorders and injuries) and contextual factors". Contextual factors are divided into environmental (social attitudes, legal and social structures and climate, etc.) and personal (age, sex or ethnicity, etc.), which affect how disability is experienced.20
Previous studies have identified that there is a relationship between depression and level of disability in female survivors of IPV.21)-(23 In such cases, the disability is manifested at both societal and individual levels, taking into account the sever-ity of violence. At the societal level it is associated which role loss and restrictions in participation, causing social isolation. At the individual level, it can be associated with experiencing limitations in conducting every day activities and both functional and physical impairments.24),(25 While some studies have identified the close relationship between depression, IPV and disability, the mediating role of depression on the latter two is not clear.21),(22 A mediating variable is one that transmits its effect on the relationship of an independent variable on a dependent variable.26
Estimating the direct, indirect or total effect of an exposure on an outcome allows the identification of mediating effects between a group of variables.26 Detecting mediation effects is useful to identify casual pathways that generate a final outcome, in this case, disability. Targeted interventions can that be created to target the mediator, which in turn positively affects the outcome. The objective of the present study is to identify the mediating effect of depressive symptoms on the relationship between the severity of IPV experienced and the level of disability experienced in female survivors of IPV.
Methods
This was a cross-sectional study performed at the baseline of a randomised control trial "Evaluation of a cognitive-behavioural intervention for victims of domestic violence in Cali and Tuluá, Colombia", registered in ClinicalTrials.gov NCT03333798. This study recruited female adults (above 18 years old) during the period from November 14th 2017 to September 27th 2019. They were survivors of IPV performed by men who were identified by two public hospitals in the South West of Colombia. Women were excluded if they had severe pathologies or symptoms of mental illness, thyroid disease or if they had received pharmacological treatment for their mental health illnesses for less than 6 months.
Instruments
The level of severity of IPV in women was measured using the Severity of Violence Against Women Scale (SVAWS), that measured the violence they had experienced by their male partner within the last 12 months. The instrument uses 3 sub-scales: threats of violence (19 questions), physical violence (20 questions) and sexual violence (4 questions). SVAWS has shown a high reliability (Cronbach alpha, 0.89-0.96),27 and it has been validated and applied previously in Colombia.28 The questionnaire has the following responses to questions on the frequency of exposure to different violent behaviours: Never: 0 points; once: 1 point; sometimes: 2 points, and many times: 3 points. The total number of points give an overall score for each item on the SVAWS scale. There are total of43 items with total possible scores ranging between 0 and 129.28
For the analysis of the severity of violence, the scores of the three types of violence were combined and the answer to each item score was weighted, as previously done by Valdez-Santiago et al.,29 where higher scores indicated higher severities of violence. Weighted scores ranged between 0 to 7, depending on the relative severity of the type of violence examined by each item. With this method, the total weighted score ranged from zero to 387 points, where a higher score indicated a higher severity of violence. Due to the wide range of values in the SVAWS weighted scale, their value was divided by 10 for the statistical analysis in the Structural Equation Model (SEM) described later.
The presence of depressive symptoms was evaluated using the instrument Hopkins Symptom Checklist (HSCL-25), which is a self-reporting scale, originally designed by Parloff et al.30, later reduced to 25 questions.31),(32 The HSCL-25 instrument has previously been validated and used in Colombia with a reported a=.88.33 The HSCL-25 instrument asks about the frequency of depressive symptoms in the last four weeks and has the following responses: never: 1 point; once: 2 points; sometimes: 3 points, and many times: 4 points. The score of the scale is calculated by taking the average score of all of the items and therefore has a range between 1 to 4 points, with 4 being the maximum score for depressive symptoms. Due to the narrow range of scores on this scale, the scores were multiplied by 10 for the analysis in the SEM. To measure the levels of disability in the study participants, the 12 item version of the Questionnaire for the Evaluation of Disability by the WHO (WHODAS 2.0) was used. This questionnaire enables an objective assessment of disability to be conducted that incorporates 6 life domains. These domains have been grouped into factors that limit activity and restrict participation and include: cognition, mobility, self-care, relationships, daily activities and participation.34 In Colombia, the WHODAS 2.0 questionnaire has been applied in diverse populations,35)-(40 including survivors of IPV.41 This is a generic disability tool with response options relating to whether difficulty is experienced and if so, how much: no, zero points; mild, 1 point; moderate, 2 points; severe, 3 points, and extreme, 4 points. This questionnaire was validated in its original version and showed a temporal stability with a intraclass correlation coefficient of .69-.89 at the item level and .98 for the total score.42),(43 The WHODAS 2.0 questionnaire scores are calculated through a complex method that establishes a scale from 0 (nil disability) to 100 points (complete disability).44
Data collection
The study instruments were administered in face-to-face interviews conducted by 6 female health professionals: 4 psychologists, 1 registered nurse and 1 general physician who had all been trained in their use.
Statistical analysis
Bivariate analyses of the sociodemographic characteristics and depressive symptoms and disability levels respectively were performed using the Mann-Whitney U and Kruskal-Wallis tests. A path analysis using the SEM was used to evaluate the mediating role of depressive symptoms on the severity of violence and level of disability. Four observed exogenous variables were used in the model which had obtained P< .20 in the bivariate analysis: age, current relationship status (in a relationship/single), schooling (low: has not finished secondary school education, and high: has attained secondary school education or more) and preceding impairments (self-reported). Impairments are defined as "problems in body function or structure such as a significant deviation or loss".45 The following endogenous variables were used in the model: severity of IPV and level of depressive symptoms (intermediate endogenous variables) and the level of disability (the main endogenous variable). The direct effect of severity of violence on disability was analysed as well as the indirect and mediating effect of depressive symptoms and the total effect of each explanatory variable.46
The method of maximum likelihood was used for the estimation of the SEM, including missing values. The 0 coefficients of the SEM are presented in a unstandardized form to aid their interpretation (Table 2 and figure 1). The comparative fit index (CFI) >.95, the Tucker-Lewis Index (TLI) >.95, and the root mean square error (RMSE) < .05 were used to establish the model adjustment.46),(47 All the analyses were performed in Stata® 14.2.
Results
Table 1 shows the sociodemographic characteristics of the study population. The median age was 35 (interquartile range, 26-43) years old, 41 women (44%) were married and 45 (48%) were in a relationship; 54 women (48%) had completed secondary education or had reached a technical or university level, and 57 (61%) were employed (Table 1).
Table 1 Sociodemographic characteristics of the study population.
| Age | |
| Mean ± SD | 36 ± 11 |
| Median(ICR) | 35(26-43) |
| 18-35 | 48(52) |
| >35-66 | 45(48) |
| Marital status | |
| Single | 41(44) |
| Married | 10(11) |
| Separated | 20(21) |
| Cohabiting with partner | 23(24) |
| Current relationship status | |
| In a relationship | 45(48) |
| Single | 49(52) |
| Education attainment | |
| Low: nil schooling, primary school Complete or incomplete, secondary School incomplete | 40(43) |
| High: secondary complete, techical certificate, university | 54(57) |
| Employmentstatus | |
| Unemployed | 37(39) |
| Employed | 57(61) |
the root mean square error (RMSE) < .05 were used to establish the model adjustment.46,47 All the analyses were performed in Stata® 14.2.
The median violence weighted score reported by the participants was 104 (43-175) points, which was 27% of the highest obtainable score in the weighted SVWAS scale (points range, 0-387). The median depressive symptoms score was 2.8 (2-3) points, that corresponded to 60% of the highest obtainable score in the HSCL-25 instrument (points range, 1-4).
The median disability score of the participants was 28 (1944), which can be interpreted as the percentage of disability experienced by responders to the WHODAS 2.0. questionnaire. There were no statistically significant differences between the median disabilities in each of the sociodemographic variables (P >.05). The median disability score for women aged 35 to 66 years old was 33 (19-48) in comparison with women aged 18 to 35, who had a median score of 27 (18-36). In both cases these medians correspond to a moderate disability (25 to 49 points).
Figure 1 and Table 2 show the non-standardized coefficients of the causal pathways between severity of IPV, level of depressive symptoms and levels of disability. The SEM shows a good fit for the data according to the indicators (x2, P = .95; CFI = 1.00; TLI = 1.23; RMSE<0.01).
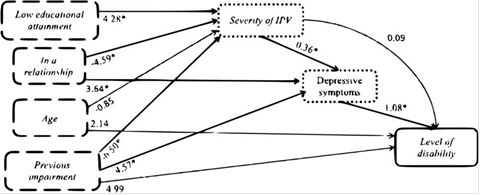
Figure 1 Casual path model and non-standardized coefficients. Boxes with dashed border contain the exogenous variables. Boxes with dotted border contain the intermediate endogenous variables, and the box with the continuous line contains the main endogenous variable. Significant coefficients at P< .05.
Figure 1 shows that low educational attainment was associated with an increase in the level of IPV experienced (0=4.28; P = .01) as a direct effect. In contrast, having a partner and a previous self-reported impairment were associated with experiencing lower levels of IPV (0=-4.59; P = .005 and 0=-6.50; P = .005 respectively). In relation to depressive symptoms, they were found to be higher in women with a current partner (0=3.64; P = .003) and with a self-reported previous impairment (0=4.57; P = .008). All these results were statistically significant.
Table 2 Direct effects, indirect effects and total effects on the relationships between severity of IPV, depressive symptoms and levels of disability.
| Parameters | Coefficient 0 | 95%CI | P |
|---|---|---|---|
| Direct effects | |||
| Violence severity a | |||
| Ageb | -0.85 | -2.33 to 0.63 | .26 |
| In a relationship (yes/no) | -4.59 | -7.84 to -1.35 | <.01 |
| Low educational attainment (yes/no) | 4.28 | 0.87 to 7.69 | .01 |
| Previous impairment (yes/no) | -6.50 | -11.09 to -1.92 | < .01 |
| Depressive symptoms c | |||
| Violence severitya | 0.36 | 0.22 to 0.50 | < .01 |
| In a relationship (yes/no) | 3.64 | 1.25 to 6.03 | < .01 |
| Previous impairment (yes/no) | 4.57 | 1.16 to 7.98 | < .01 |
| Level of disability | |||
| Violence severitya | 0.09 | -0.28 to 0.46 | .63 |
| Depressive symptomsc | 1.08 | 0.40 to 1.04 | < .01 |
| Ageb | 2.14 | -0.39 to 4.69 | .98 |
| Previous impairment (yes/no) | 4.99 | 1.75 to 11.97 | .24 |
| Indirect effects | |||
| Depressive symptoms c | |||
| Age b | -0.30 | -0.86 to 0.24 | .27 |
| In a relationship (yes/no) | -1.57 | -1.20 to 0.37 | .01 |
| Low educational attainment (yes/no) | 1.56 | 0.26 to 4.42 | .02 |
| Previous impairment (yes/no) | -2.37 | -4.28 to -0.45 | .15 |
| Level of disability | |||
| Violence severitya | 0.39 | 0.24 to 0.55 | < .01 |
| Ageb | -0.41 | -1.20 to 0.37 | .20 |
| In a relationship (yes/no) | 1.72 | -2.02 to 0.46 | .36 |
| Low educational attainment (yes/no) | 2.09 | -0.21 to 4.41 | .07 |
| Previous impairment (yes/no) | 1.80 | -3.37 to 6.98 | .49 |
| Total effects | |||
| Violence severity a | |||
| Age b | -0.84 | -2.33 to 0.63 | .26 |
| In a relationship (yes/no) | -4.59 | -7.84 to -1.35 | < .01 |
| Low educational attainment (yes/no) | 4.28 | 0.87 to 7.69 | .01 |
| Previous impairment (yes/no) | -6.50 | -11.09 to -1.92 | < .01 |
| Depressive symptoms c | |||
| Violence severitya | 0.36 | 0.22 to 0.50 | < .01 |
| Ageb | -0.46 | -1.29 to 0.36 | .27 |
| In a relationship (yes/no) | 2.95 | -0.93 to 0.83 | .13 |
| Low educational attainment (yes/no) | 1.56 | 0.17 to 2.94 | .02 |
| Previous impairment (yes/no) | 2.20 | -1.50 to 5.91 | .24 |
| Level of disability | |||
| Violence severitya | 0.48 | 0.08 to 0.89 | .01 |
| Depressive symptomsc | 1.08 | 0.60 to 1.57 | < .01 |
| Ageb | 1.73 | -0.91 to 4.38 | .19 |
| In a relationship (yes/no) | 1.72 | -2.02 to 5.46 | .36 |
| Low educational attainment (yes/no) | 2.09 | -0.21 to 4.42 | .07 |
| Previous impairment (yes/no) | 6.80 | -1.50 to 5.91 | .14 |
| 95%CI: 95% confidence interval. a IPV severity divided by 10. b Age divided by 10. | c Depression scale multiplied by 10. |
The results show that a mediating role exists between IPV severity and level of disability. The direct effect of IPV severity on level of disability was not statistically significant (0=0.09; P = .63), however, the indirect effect of IPV severity on dis-ability mediated by depressive symptoms was (0=0.39; P< .01). The total effect of IPV severity on the level of disability was even greater (0=0.48; P = .01). Additionally, the direct effect of depressive symptoms on the level of disability was also statistically significant (0=1.08; P< .01).
With respect to the remaining total effects, depressive symptoms were positively affected by IPV severity (0=0.36; P< .01) and low educational attainment (0=1.56; P = .02). Finally, low educational attainment was marginally positively associated with level of disability (0=2.09; P = .07).
Discussion
The objective of this study was to determine the mediating role of depressive symptoms on the relationship between the severity of IPV experienced and the level of disability in female survivors of IPV in Cali and Tuluá, Colombia.
The median weighted-score of IPV experienced by women in this study was 104 (42.5-175) points, which was 27% of the highest obtainable score of the weighted SVAWS scale. This median was similar to that reported by a previous study in Cali, where they found a mean violence of 41 ± 29 points in adult female survivors of IPV attending community centers. This mean value corresponded to 30% of the maximum score in the version of the SVAWS scale used (maximum, 138 points).28) However, this study used the SVAWS instrument without considering weighted-scores for each of the items used in their research. This was advisable according to the method pro-posed by Valdez et al.,29 which takes into account the severity of different expressions of violence.
The documented prevalence of depression among women who have experienced IPV varies, for example it has been reported as being 47% in North-American women18 and up to 75% in women in China.48 The median score for the number of depressive symptoms in the HSCL-25 instrument reported by women in this study was 2.8 (2.4-3.4)) out of a possible maximum of 4. The cut off point for positive cases of depression (1.75 points) was met or passed by an alarming 98% of women in Cali and 89% in Tuluá.
This study found that the direct effect of severity of IPV on the level of disability was not significant (0=0.09; P = .63). However, it did find a statistically significant indirect affect and therefore mediating role of depressive symptoms on the relationship between the severity of IPV and the level of disability (0=0.39; P<.01).
In view of these findings, this study suggests that after a woman is exposed to IPV, the presence of depressive symptoms is one of the main casual pathways associated with disability. In spite of the scarce amount of evidence that supports this type of analysis, there have been many reports of associations between the 3 different variables in this study. For instance, Bogantes-Rojas,25 in their analysis on the cycle of abuse of domestic violence, describe depression and the presence of a physical or mental disability as direct consequences of IPV.
Both pre-existing physical and mental health illnesses, and those directly associated with IPV cause varying levels of dis-ability. This study measured the level of disability using the WHODAS 2.0 questionnaire that evaluates disability taking a biopsychosocial approach with an emphasis on limitations on activity and restrictions on participation.44 In the United States, a study investigated the impact of IPV on different aspects of "functioning", and found that nearly 45% of women with depressive symptoms had difficulties in their ability to work, attend school activities and participate in activities of daily living. They also reported difficulties in establishing effective social interactions in everyday environments and in finding social support.23
This data implies that depressive symptoms generate restrictions on the social participation of female survivors of IPV who are already facing difficult situations such as social isolation and role loss.23),(49 There are scarce studies from Colombia that evaluate the relationship between IPV, depressive symptoms and disability. Furthermore, theoretical models studying the relationships between health conditions and their context are not widely available.
This study found that depressive symptoms significantly, directly affected the level of disability, and mediated the effect of IPV severity on functional impairment levels. Similar results were found in a longitudinal path analysis among women exposed to previous mass conflict traumas in post-conflict Timor-Leste, where both disability and IPV were associated with depressive symptoms. Authors have previously planted ideas that depression is related to one's self-perception of their physical and mental health and subjective experience of living with disability. This assumption substantiates the importance of performing multivariate analyses that contain the personal and contextual factors (variables) in survivors of IPV unpredictive models of disability.50
Some findings in this current study were contradictory to those found in previous literature. Firstly, women in this study with an existing impairment were found to have experienced less severe levels of IPV. However, other studies have found that health conditions leading to disabilities increased the probability of having experienced physical, psychological and sexual IPV. This is thought to be due to these women being more vulnerable due to their condition and being economically dependent on their dominant partner.51
This study also found that women in this study who had a current partner had experienced lower levels of violence. As participants were asked about their experiences of violence within the last 12 months only, it may have not detected women who had experienced IPV by the irex-partners. A study from Mexico by Zaldivar-Cerón et al.52 found that separating from the aggressor does not imply an end to IPV by that same partner. On the contrary, it can lead to violent behavior due to the threat that the perpetrator may lose control and power over their target. This behavior can be explained by the cycle of abuse, where the honeymoon phase is not reached.
The sample size of this study is an important limitation that made it impossible to identify possible associations between exposures that were not considered in the SEM, for example alcohol and illicit drug abuse by the woman or her intimate partner. Given the complex phenomena of depression, IPV and disability, they have multiple explanatory variables. These are pertinent in understanding the pathways leading to them. Despite this limitation, the SEM was able to identify associations at the individual level, such as a previous impairment and education level as endogenous variables.
According to the authors' knowledge, the SEM analysis used in this study has proved to be innovative in Colombia where it has not previously been used in the context of depression, disability and IPV. Additionally, the SEM analysis enabled a simultaneous model to be run that included the study of relationships between multiple independent and dependent variables that are pertinent for the explanation of the complex phenomena of depression, IPV and disability.47),(53
Conclusions
The SEM showed that depressive symptoms have a mediating role on the relationship between the severity of exposure to IPV and the level of disability in women from 2 cities in the South West of Colombia. Alarmingly high levels of depression were found in this study which were also associated with experiencing IPV. Depression was also associated with having a self-reported impairment.
Education was an important additional factor found to be linked with both IPV and depression, which suggests that improved access to education is important in tackling these and ultimately disability.
Overall, these results indicate that attention to the amelioration of depressive symptoms are an essential step to improve the functionality of female survivors of IPV in middle income countries

