











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Syncope is a common clinical entity, accounting for almost 3% of emergency room admissions and 6% of hospitalizations 1. The incidence rate is 6.2 cases/1,000 persons/year; however, the incidence increases with age, especially in the elderly 2. Thus, in those over the age of 80, the incidence rises to 19.5 cases/1,000 persons/year 3. No epidemiological data on this topic are available in our setting. The prognosis of syncope varies and depends mainly on the underlying medical condition. The one-year mortality rate for vasovagal syncope is 0%, but in cardiogenic syncope, mortality may reach up to 30% 4.
Almost 40% of patients who are seen in the emergency room for syncope are hospitalized, and the average length of hospital stay is 5.5 days 5. This, together with the lack of a specific diagnostic test, leads to the indiscriminate use of diagnostic tests, increasing care costs which, according to the Medicare database in North America amount to US$5,400 per hospitalized patient. In addition, when liberal management strategies are compared to a standardized management strategy, the latter shows a 29% reduction in the average cost per syncope diagnosis 6.
The Short-Term Prognosis of Syncope (STePS) study determined short-term (10-day) prognostic factors which include: an abnormal electrocardiogram, concomitant trauma, the absence of prodromal autonomic symptoms and male sex 7. The objective of the study was to evaluate the performance of this rule in a population of patients presenting to the emergency room with syncope.
Materials and methods
This was a prospective, observational study performed at the Hospital Universitario Clínica San Rafael in Bogotá, Colombia. The inclusion criteria were: patients over the age of 18 who were admitted to the emergency room with a diagnosis of syncope, defined as loss of postural tone with a transient (no greater than five minutes) loss of consciousness followed by spontaneous total recovery, without neurological sequelae (except amnesia of the event). The exclusion criteria were: head trauma prior to the loss of consciousness (LOC), non-spontaneous recovery of consciousness, similar non-syncopal syndromes (dizziness, vertigo, collapse, seizures), alcohol or drug abuse, and refusing to consent to participate in the study.
The same 10-day serious outcomes from the original study were evaluated: death, patient readmission for the same or similar symptoms within the first 10 days after the initial syncopal event, and need for major therapeutic procedures due to the syncope (cardiopulmonary-cerebral resuscitation, admission to intensive care, cardioverter-defibrillator or pacemaker implantation, and starting acute antiarrhythmic treatment).
Syncope prodrome symptoms were defined as the presence of autonomic symptoms immediately prior to syncope, such as feeling hot, weakness, blurred vision, nausea, diaphoresis, piloerection or abdominal discomfort. An abnormal electrocardiogram was defined as any of the following: atrial fibrillation, supraventricular tachycardia, sinus pauses for > 2 seconds, sinus bradycardia (fewer than 50 beats per minute), conduction disorders (right bundle branch block, left bundle branch block, left anterior-superior or posterior-inferior fascicular hemiblock of the bundle of His, second degree Mobitz I atrioventricular block or greater), signs of left or right ventricular hypertrophy, signs of previous myocardial infarction or multiple ventricular extrasystoles.
Patient follow-up was conducted on day 10 to record outcomes, using a directed interview or chart review for patients who were still hospitalized, or a telephone call to patients discharged during the first 10 days.
A descriptive analysis of the demographic and clinical variables of the study population was performed, as well as a comparative analysis according to admission/non-admission to the intensive care unit (ICU). A Chi-square test was used for qualitative variables, and Student's t-test for quantitative variables. The behavior of the STePS prediction rule was differentiated according to the prevalence of one of its four criteria, or their sum, with a bar graph of percentage values. Variables which represented risk factors associated with serious 10-day outcomes were selected for inclusion in a logistic regression model. Statistically significant association was defined as a p < 0.05. An outcome consisting of serious events at 10 days was established and analyzed with regard to the presence of any of the criteria evaluated by the STePS prediction rule. Finally, the performance characteristics of the STePS prediction rule were determined according to each of the criteria it evaluates, and the operative characteristics for each criterion and for the rule in general were graphed, with an area under the curve greater than 0.8 considered acceptable and an area under the curve greater than 0.9 considered optimal.
The analysis was performed on SPSS V.18. This protocol adhered to the international norms of the Treaty of Helsinki. The data collection process conformed to the established scientific principles, with patient safety as the priority.
Results
A total of 98 patients were included; the average age of the population was 63±21 years, and 60.2% (n=59) were women. The demographic, clinical and laboratory characteristics are found in Table 1. Altogether, 36.7% (n=36) of the population had a history of syncope. For 31.3%, syncope had occurred within the six months prior to admission. Twelve patients had had more than one syncopal episode in the six months prior.

The most commonly used medications were angioten-sin-converting enzyme (ACE) inhibitors, or angiotensin II receptor blockers (ARBs) (38.8%), with losartan being the most frequently prescribed drug (21.4%). Second were beta blockers (29.6%), with metoprolol being the most frequently prescribed (15.3%). In addition, some patients were on calcium channel blockers (10%) or antiarrhythmics (6%).
The electrocardiogram showed that 82.7% (n=81) of the patients had one or more disorders. The most frequent were bradycardia (22.4%), left ventricular hypertrophy (20.4%) and nonspecific T wave or ST segment abnormalities (28.6%).
With regard to the characteristics of the syncopal event, 52% had a prodrome (n=51), the most frequent being diaphoresis (33%) and blurred vision (28.6%), while palpitations were only present in 15.3% of cases (n=15). Syncope with exertion presented in 6.1% of the patients (n=6), 9% (n=9) had supine syncope, and 10 patients (10.2%) presented syncope in hot and poorly ventilated spaces. Concomitant dyspnea and chest pain presented in 33 and 34 patients (33.7 and 34.7%), respectively.
The incidence of the general outcomes 10 days after the event is described in Table 2. Transfer to the ICU, arrythmias and acute myocardial infarction were the most frequent (28.6, 17.3 and 14.3%, respectively).
Table 2 Outcomes at 10-day follow up
| 10-day Outcomes | n (%) |
|---|---|
| Death | - |
| Acute myocardial infarction | 14 (14.3) |
| Arrhythmias | 17 (17.3) |
| Ventricular fibrillation | - |
| Ventricular tachycardia | 3 (3.1) |
| Sinus pause | 2 (2.0) |
| Pulmonary embolism | 1 (1.0) |
| Cerebrovascular accident | 1 (1.0) |
| Intracranial hemorrhage | 1 (1.0) |
| Major hemorrhage | 4 (4.1) |
| Blood product transfusion | 3 (5.0) |
| Hospital readmission | - |
| Sepsis | 1 (1.0) |
| Cardiopulmonary resuscitation | 1 (1.0) |
| Percutaneous coronary intervention | 9 (9.2) |
| Pacemaker implantation | 9 (9.2) |
| ICD placement | 3 (3.1) |
| Abdominal aortic aneurysm surgery | 1 (1.0) |
| Myocardial revascularization | 2 (2.0) |
| Vasopressor initiation | 8 (8.2) |
| Use of antiarrhythmics | 9 (9.2) |
| ICU admission | 28 (28.6) |
| ICD: Implantable cardioverter defibrillator, ICU: Intensive Care Unit. | |
A comparative analysis was made according to the criterion of admission or non-admission to the ICU at 10 days. A statistically significant difference was found between these two groups with regard to the following variables: age >65 years (75 vs. 50%, p=0.02), history of heart failure (35.7 vs. 17.1%, p=0.047), chronic kidney disease (32.1 vs. 7.1%, p=0.002) and heart disease (50 vs. 24.3%, p=0.01), with these being more prevalent in the population admitted to the ICU. There were no differences with regard to the rest of the age ranges, sex, history of peripheral artery disease, cerebrovascular accident (CVA), arrhythmias, prior syncope, and need for pacemaker or ICD.
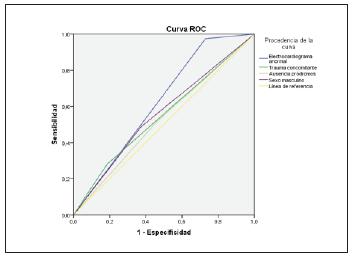
The criteria assessed by the STePS prediction rule behaved as follows: electrocardiogram abnormalities were the most frequent criterion (82.7%), followed by lack of prodrome (48%), male sex (41.8%) and the presence of associated trauma (22.4%), in order of frequency.
The distribution of serious events at 10 days according to the STePS prediction rule is shown in Table 3. The most frequent serious event was ICU admission (28%, n=28).
Table 3 Prevalence of serious events at 10-day follow up according to STePS.
| Outcomes (n, %) | 10 days |
|---|---|
| Death | - |
| Readmission | - |
| CPR | 1 (1.0) |
| ICU admission | 28 (28.6) |
| ICD | 3 (3.1) |
| Pacemaker implantation | 9 (9.2) |
| Use of antiarrhythmics | 9 (9.2) |
| CPR: Cardiopulmonary resuscitation ICU: Intensive care unit, ICD: implantable cardioverter-defibrillator. | |
Variables with a statistical significance less than or equal to 0.05 in a search for association were selected as risk factors associated with these serious 10-day outcomes to be included in a logistic regression model. The logistic regression model showed that an abnormal electrocardiogram (OR 13.98, 95% CI 1.29-151.9) and concomitant trauma (OR 5.22, 95% CI 1.20-22.67) were statistically significant in the prediction of adverse events. The rest of the factors, such as age over 65 years (OR: 2.20; CI: 0.72-6.7), male sex (OR: 1.2; CI 0.39-3.69), the presence of heart failure (OR: 1.92; CI: 0.45-8.16), peripheral artery disease (OR: 2.17; CI: 0.27-17.34), chronic kidney disease (OR: 2.46; CI: 0.41-14.7), cerebrovascular accident (OR: 0.69; CI: 0.02-20.48), heart disease (OR: 3.16; CI: 0.62 - 16.09) arrhythmia (OR: 5.41; CI: 0.32-91.46), prior syncope (OR: 0.57; CI: 0.17-1.95), pacemaker implantation (OR: 0.19; CI: 0.00-10.15), ICD implantation (OR: 0.29; CI: 0.01 -18.93) and lack of prodrome (OR: 0.86, CI: 0.29 - 2.59) did not show the same behavior.
The operative characteristics of the STePS prediction rule are described in Table 4.
Table 4 Operative characteristics of the STePS predition rule criteria.
| Criteria | Sensitivity | Specificity | PPV | NPV | AUC-ROC |
|---|---|---|---|---|---|
| Abnormal EKG | 97.44 | 27.12 | 46.91 | 94.12 | 0.623 |
| Trauma | 28.21 | 81.36 | 50.00 | 63.16 | 0.548 |
| Lack of prodrome | 51.28 | 54.24 | 42.55 | 62.75 | 0.528 |
| Male sex | 48.72 | 62.71 | 46.34 | 64.91 | 0.557 |
| PPV: Positive predictive value, NPV: Negative predictive value, AUC: Area under the receiver operating characteristic curve. | |||||
Finally, the total number of prediction rule criteria applicable to each patient was calculated. The area under the curve of this graph is 0.64 (95% CI; 0.53-0.75) (Figures 1 and 2).

Discussion
Our greatest finding is that when we evaluated the operative characteristics of the STePS prediction rule in our population, we found no utility for predicting short-term serious events. These different results from those of the original study are characterized by the following findings 7.
First, in our cohort there were no cases of mortality or readmission 10 days after the syncopal event, while there were three fatalities (1.4%) in the STePS study, all within the first 48 hours and in individuals over the age of 60. However, in our cohort, 51% of the patients (n=50) required some type of major therapeutic procedure, while in the baseline study only 13.3% required these procedures. A probable explanation of this finding is that our population had a greater degree of severe heart disease and comorbidities than the STePS cohort, in the sense that there was a higher proportion of patients who required ICU admission (28.57 vs. 2.29%). These differences may be related to the characteristics of the study population which, although younger (62 ± 21 vs. 72 ± 15 years) in our study, had more prior heart disease (31.6 vs. 24.5%) and a greater frequency of heart failure (22.4 vs. 3.5%), respectively.
In our population, we found a difference in the variables of age >65 years (p=0.02), history of heart failure (p=0.047), chronic kidney disease (p=0.002) and heart disease (p=0.01) between patients who were admitted to the ICU and those who did not need it. We believe that these four parameters could be significant predictors of serious short-term outcomes, since ICU admission was the most frequent outcome in the study cohort, accounting for 56% of all serious 10-day outcomes. These associations were not documented in the primary study.
In our study, only two of the four STePS rule parameters proved to be risk factors for serious 10-day outcomes: an abnormal electrocardiogram (OR 13.98, 95% CI 1.29-151.9) and concomitant trauma (OR 5.22, 95% CI 1.20-22.67). However, this association was not found for the variables of male sex and lack of prodrome, which was reported in the STePS study.
We found that the STePS prediction rule performs modestly in predicting an outcome of serious events at 10 days, given that the discriminatory power is low, with an AUC-ROC value of 0.64 (95% CI: 0.53-0.75), especially considering that the confidence interval is wide, including a lower limit of 0.53, which would correspond to the same predictive power as chance. The behavior of each of the rule's components, individually, is similar, with the electrocardiogram abnormalities parameter having the highest value (AUC-ROC 0.623), although still modest, since in no case was the AUC-ROC greater than 0.8. The original study did not carry out this analysis of the global discriminatory power or the predictive power of each of its variables with regard to short-term serious outcomes.
With a more detailed analysis of the operative characteristics of each of the rule's components, we found that the only parameter with good sensitivity was an electrocardiogram abnormality (97.44% sensitivity), while the only one with an acceptable specificity was concomitant trauma (81.36% specificity). This is related to the previously described finding of a predictive association between these parameters and the short-term outcome both in our cohort as well as in the original STePS study. Thus, having a normal electrocardiogram on admission rules out, with a high degree of confidence, the possibility of having a serious outcome within 10 days after the syncopal episode, as long as there is no concomitant trauma, which would increase the probability of an adverse outcome. Analyzed another way, having a STePS score of 0 would rule out a serious outcome in the short term. However, there is no STePS cut-off point (from 1-4 points) which will accurately determine those who will develop adverse outcomes.
On the other hand, there are other clinical tools in the literature for predicting short-term outcomes in patients with syncope, and which in most cases have validation studies with results which differ from those of the pioneer studies 8-10. The first and best known is the San Francisco rule, which, in the study from which it was derived, showed that the presence of any of the variables of abnormal electrocardiogram, hematocrit <30%, dyspnea on admission, systolic arterial pressure (SAP) <90 mmHg on admission, and history of heart failure was correlated with death or adverse events within seven days of syncope, with a 96% sensitivity and 62% specificity 12. The same researchers subsequently carried out an internal validation study with a similar performance of 98% sensitivity and 58% specificity 13. In this regard, several validation studies of this rule have been performed in different populations without achieving similar results, finding a sensitivity of 74-89% and a specificity of 42-57% 14,15. Likewise, a systematic review of the literature emitted the same conclusion, identifying 12 studies with a total of 5,316 patients and a consistently lower yield of the San Francisco rule than that of the original study (87% sensitivity and 52% specificity) 16.
The ROSE scale is another rule, which was derived and validated in 2010 in Edinburgh, in the emergency room of a local hospital 17. The authors recorded a sensitivity of 87% and a specificity of 66% for predicting serious outcomes 30 days from the index event in those who met at least one of the rule's criteria (BNP >300 pgr/mL, heart rate < 50 bpm, positive fecal occult blood, hemoglobin <9.0 gr/dL, chest pain, and oxygen saturation <94%). In the internal validation of the study, the authors found a lower sensitivity of the rule in 550 patients recruited using the same criteria as the original cohort. There are no other validation studies for this scale for short-term outcomes; however, a study which evaluated its performance for one-year mortality and serious outcomes found a sensitivity of 71.6% and a specificity of 71.1% 18.
Conclusions
In this prospective observational study of patients hospitalized for syncope, the STePS prediction rule did not perform favorably in predicting serious outcomes within 10 days of the syncopal event. The STePS rule has no cut-off point (from 1-4 points) which accurately determines who will develop adverse outcomes. Only an individual association of the variables of electrocardiogram abnormalities and concomitant trauma with the need for major therapeutic procedures within 10 days of syncope was shown (mainly ICU admission). We found that a history of chronic kidney failure, heart disease, age over 65 years and heart failure (which were not included in the initial STePS prediction rule) were possible additional risk factors for serious 10-day outcomes.

