











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Ameloblastoma is a benign slow-growing odontogenic neoplasm, that forms from the neoplastic odontogenic epithelium within a mature fibrous stroma devoid of ectomesenchyma. Characterized by expansion and tendency to local recurrence if it is not properly treated 1,2; it presents as a radiolucent unilocular or multilocular lesion, which can lead to the expansion and thinning of the bone cortex 3. Clinically it can be classified into 3 types, solid or multicystic, unicystic and peripheral. The solid type generally presents greater local aggressiveness, which differs from the unicist variant 4,5.
About 80% of all ameloblastomas are located in the mandible, mainly in the molar region 6,7. Due to socioeconomic situations and limited access to health services, some patients with ameloblastoma in developing countries often experience massive growth injuries before seeking care 8,9.
The typical treatment for ameloblastoma is radical resection with safety margins. Conservative treatment can also be used and has limited indication, which may include methods such as decompression, enucleation, curettage, peripheral ostectomy and chemical or physical cauterization 10-13. Given the above, the objective of this work was to describe a case of unicystic ameloblastoma in the mandible, treated in a more conservative way.
Case Report
A 53-year-old male patient was referred to a buccomaxillofacial surgery and traumatology service for consultation in November 2018. In the anamnesis, the patient reported a three-year increase in volume as the main complaint. On extra oral physical examination, he presented facial asymmetry (Figure 1a). In the intraoral physical examination, there was an increase in volume in the anterior region of the mandible, of hard consistency and coloration similar to mucous (Figure 1b).

Figure 1. Initial clinical aspect. A - Front view of the patient, showing facial asymmetry. B - Intraoral view of the patient, showing an increase in the volume of normal mucosa color in the mandible.
Panoramic radiography was performed, which showed multilocular radiolucent lesion (Figure 2). The aspiration puncture revealed a brownish liquid content, suggesting that it was a cystic lesion.

Figure 2 Panoramic radiograph showing radiolucent, well-defined, multilocular lesion, extending from the body of the mandible on the left side to the region of the tooth 45. The lesion caused root resorption, tooth displacement, bulging and thinning of the base of the mandible on the left side.
Therefore, under local anesthesia, a decompression device was placed and an incisional biopsy was performed, the diagnosis of which was suggestive of unicit ameloblastoma.
Due to the size of the lesion, it was decided to maintain the decompression device, requiring quarterly follow-up, to evaluate the bone neoformation (Figure 3), and the extraction of the lower teeth. After one year, it was noted that there was no bone neoformation, so conservative marginal resection was performed maintaining the basilar of the mandible, next to the affected mucous, and peripheral ostectomy (Figure 4).
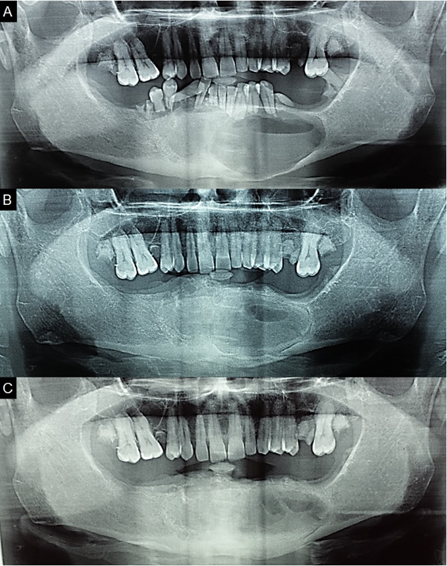
Figure 3 Panoramic radiograph. A, B and C: Panoramic radiographs showing new bone formation in the region.
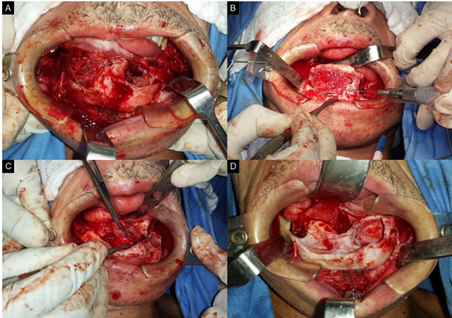
Figure 4. Surgical approach to the lesion. A - Exposure of the tumor. B - Peripheral ostetomy. C - Removal of the tumor. D - Bone defect after peripheral ostectomy.
After excision of the lesion (Figure 5), the material was sent for histopathological analysis, whose findings were of unicystic ameloblastoma, of the luminal type (Figure 6). The postoperative period occurred without any complications, after one month the patient did not present any facial alteration or infection (Figure 7) and is being monitored without signs of recurrence.

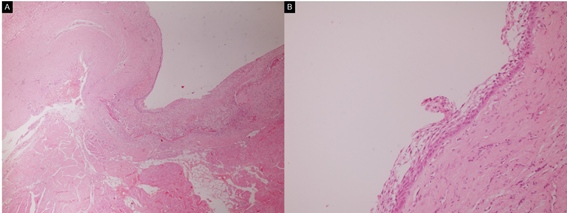
Figure 6 Histological analysis of the surgical specimen. A - Proximity of the tumor to the areas of fatty and striated skeletal muscle (hematoxylin-eosin stain, x40). B - The basal layer, presents cuboidal and columnar cells, of hyperchromatic nuclei, some of which have inverted polarization and arranged with palisades, the other layers are loosely arranged (hematoxylin-eosin stain, x 400).

Discussion
Ameloblastoma is an uncommon benign odontogenic tumor, locally aggressive, which rarely causes metastasis, can reach considerable dimensions, causing facial deformity and functional impairment and if not treated properly it can reapper 14,15. Unicystic ameloblastoma (UA), which is a clinical variant of ameloblastoma, is a cystic lesion, which presents clinical and radiographic characteristics of a cyst and histopathologically is formed by ameloblastomatous epithelium 16,17. This injury was first described by Robinson and Martinez in 1977 18,19. The UA preferentially affects young patients, during the second decade of life, with an average age of 16 years and with a slight predilection for males. The lesion is usually asymptomatic, occurs in the posterior region of the mandible and is characterized by a painless swelling 6,20. The patient in question had characteristics that fled slightly from the pattern found in the world literature, due to the age and location of the tumor.
Radiographically is usually a well-defined unilocular radiolucent lesion 4,14,20, although less frequent, the multilocular aspect has been reported 5,17. UA is classified histologically into groups, luminal, intraluminal and mural. In the luminal variant, the tumor is confined to the cystic lining. In the intraluminal variant, neoplastic epithelium is projected towards the cystic cavity. In the mural type, the capsule is infiltrated by the neoplastic epithelium. AU is usually less aggressive than solid, probably this behavior is associated with histological characteristics 18,19. The studied patient presented a multilocular radiographic lesion, which, although less prevalent, has been reported.
The definitive treatment of ameloblastoma is surgical and it is usually a safe resection, with the possibility of removing soft tissue. However, the extent of surgical intervention and the adoption of conservative or radical measures remains controversial 4. The management of ameloblastoma represents a challenge for surgeons, because it requires not only adequate resection, but also functional and aesthetic reconstruction of the residual defect 21. Surgical treatment can be separated into conservative and radical methods, depending on histological, radiographic and clinical characteristics, such as location, size of the lesion and age of the patient 22,23.
Radical treatment is characterized by mandibulectomy or segmental resection of the lesion with safety margins 4,5. This form of treatment is associated with low recurrence of the lesion, however it can cause numerous complications, such as facial deformities, dysfunctions, and psychological changes 4,22. Conservative AU treatment consists of enucleation and/or marsupialization, combined or not with supportive techniques, such as curettage, peripheral ostectomy and cauterization. This technique is associated with less functional and aesthetic impairment, however, it may have a higher recurrence rate 4,5.
Decompression has long been used as a treatment for odontogenic cystic lesions, mainly in large extensions in the mandible. This technique promotes bone neoformation and prevents extensive surgery 2. It is applied more frequently for unicystic ameloblastoma, although some surgeons also use it as a success for multicystic ameloblastoma 1,2,24.
Peripheral ostectomy/curettage aims to remove the infiltrative tumor islands that may exist in the residual bone walls after simple enucleation. In order to destroy remnants of tumor islands, chemical cauterization can also be performed, through carnoy’s solution, or physical, using liquid nitrogen 25.
Conservative treatment represents a reliable approach to the management of unicystic ameloblastoma, presenting good aesthetic, functional and with low-risk of recurrence results 2,4,10,23,24. In the patient described, the conservative technique was chosen, due to the initial size of the lesion and the clinical type of the tumor. Even if marginal resection was performed, it only happened after decompression and a significant reduction of the neoplasia. Carnoy's solution was not used, due to the risk of injury to the lower alveolar nerve and neither liquid nitrogen, due to the thickness of the bone remnant and the possibility of fracture, thus opting for peripheral ostectomy.
Conclusion
The reported case emphasizes the importance of more conservative treatment, especially for large-volume unicystic ameloblastoma. This approach has been described and associated with positive aesthetic and functional results, in addition to a lower recurrence rate, being positive when considering the impact of a more radical treatment on the patient.

