











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Primary health care (PHC) is the first level of contact individuals have with the healthcare system. It is the gateway to most services and interventions required, and it encompasses a set of actions to promote, protect, diagnose, treat, rehabilitate, and monitor health needs 1. To provide these health actions and services, a deeper understanding of PHC is key, with emphasis on understanding and analyzing the work environment of the healthcare professionals who work in this field 2.
The PHC environment is not limited to meeting the population's health needs, as it becomes a continuous space for reflection and improvement. Improving work conditions for professionals emerges as an essential component in ensuring the quality and effectiveness of the services provided. This assigns PHC an important role not only in the clinical approach but also in promoting a work environment conducive to the well-being of professionals that contributes to optimizing care for the community 2,3.
Work activities include physical, social, emotional, and technical elements that influence the professional experience. In healthcare, this environment transcends physical facilities, encompassing human interactions, clinical protocols, and interdependence between professionals 4.
Furthermore, nurses' work environment in PHC is determined by its challenging nature, with their work being strongly related to disease prevention, health promotion, and the creation of innovative strategies to meet the specific needs of each community. They face a dynamic environment and often have limited resources and varied demands, which requires management and decision-making skills 5.
Achieving excellence in nursing care requires addressing the factors that mold this type of care, and the work environment is a core element in this process 6. The interaction between the work environment and the quality of care in PHC is unquestionable. A favorable work environment not only has a positive impact on the health and well-being of nurses but also directly influences the quality and efficiency of the care provided to the population 2,7.
In this sense, the urgency of improving the work environment becomes clear, highlighting the need for positive changes and understanding the dynamics of the work environment of nurses in PHC. This emphasizes the importance of strategies aimed not only at valuing these professionals but also at improving their work conditions as a whole 8. In a scenario of constant transformation in the healthcare sector, it is imperative to understand the current state of science on the structure and work conditions of PHC nurses. Therefore, the aim of this study is to identify, in the scientific literature, the aspects related to the work environment that influence the work of nurses in PHC.
Materials and Methods
This is an integrative literature review registered on the Open Science Framework platform, developed in six stages, as follows: defining the research question based on the problem, searching the literature, applying the inclusion criteria, evaluating the studies, analyzing the data, and synthesizing the knowledge with the presentation of the review 9. The selection process for the publications followed the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses - Prisma 10.
In the first stage, the research question was devised using the PICo strategy 11, where "P" stands for population (nurses); "I" for the phenomenon of interest (work environments), and "Co" for the context (PHC). The research question that guided the review was regarding which factors related to the work environment influence the performance of PHC nurses.
In the second stage, the data was searched in August 2023. Six databases were searched: Lilacs (Latin American and Caribbean Health Sciences Literature), Cinahl (Cumulative Index to Nursing and Allied Health Literature), Web of Science, Medline (Medical Literature Analysis and Retrieval System Online), Scopus, and Embase. The search used the controlled descriptors of the Medical Subject Headings (MeSH) and the Descriptors in Health Sciences (DEcS): work conditions (condições de trabalho/ambiente de trabajo); primary health care (atenção primária à saúde/ atención primaria de salud); nursing (enfermagem/'enfermería), combined by the OR and AND Boolean operators. As this is an underexplored topic, keywords (non-controlled vocabularies) were added to direct the search strategy (Table 1).
Table 1 Database Search Strategy. Florianópolis, Santa Catarina, Brazil, 2023
| Database | Search Strategy |
|---|---|
| Scopus, Web of Science, Embase, and Cinahl | ("Working Conditions" OR "Working Condition" OR "Workplace Condition" OR "Workplace Conditions" OR "Workplace Environment" OR "Workplace Environments" OR "Work Environment" OR "Work Environments" OR "Working Environment" OR "Working Environments" OR "Workplace" OR "Workplaces") AND ("Primary Health Care" OR "Primary Care" OR "Primary Healthcare" OR "Health Care Primary") AND ("Nursing" OR "Nursings" OR "Nurses" OR "Nurse") |
| Lilacs via BVS | ("Working Conditions" OR "Working Condition" OR "Workplace Condition" OR "Workplace Conditions" OR "Workplace Environment" OR "Workplace Environments" OR "Work Environment" OR "Work Environments" OR "Working Environment" OR "Working Environments" OR "Workplace" OR "Workplaces" OR "Condições de Trabalho" OR "Ambiente Externo de Trabalho" OR "Ambiente de Trabalho" OR "Condição de Trabalho" OR "Condição do Local de Trabalho" OR "Ambientes de Trabalho" OR "Local de Trabalho" OR "Condiciones de Trabajo" OR "Ambiente de Trabajo" OR "Ambiente del Trabajo" OR "Ambiente en el Trabajo" OR "Condiciones de Trabajo" OR "Condiciones del Lugar de Trabajo" OR "Condición del Lugar de Trabajo" OR "Condición Laboral" OR "Entorno de Trabajo" OR "Entorno del Lugar de Trabajo" OR "Entorno Laboral" OR "Lugar de Trabajo") AND ("Primary Health Care" OR "Primary Care" OR "Primary Healthcare" OR "Health Care Primary" OR "Atenção Primária à Saúde" OR "Atenção Primária" OR "Atenção Primária de Saúde" OR "Atenção Primária em Saúde" OR "Atenção Básica" OR "Atenção Básica à Saúde" OR "Atenção Básica de Saúde" OR "Atención Primaria de Salud" OR "Atención Básica" OR "Atención Primaria" OR "Asistencia Primaria" OR "Asistencia Primaria de Salud") AND ("Nursing" OR "Nursings" OR "Nurses" OR "Nurse" OR "Enfermagem" OR Enferm* OR "Enfermería") |
| Medline via PubMed | ("Working Conditions" [Mesh] OR "Working Conditions" OR "Working Condition" OR "Workplace Condition" OR "Workplace Conditions" OR "Workplace Environment" OR "Workplace Environments" OR "Work Environment" OR "Work Environments" OR "Working Environment" OR "Working Environments" OR "Workplace" [Mesh] OR "Workplace" OR "Workplaces") AND ("Primary Health Care" [Mesh] OR "Primary Health Care" OR "Primary Care" OR "Primary Healthcare" OR "Health Care Primary") AND ("Nursing" [Mesh] OR "Nursing" OR "Nursings" OR "Nurses" [Mesh] OR "Nurses" OR "Nurse") |
Source: Prepared by the authors.
To expand the search possibilities, the journal website of the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior -Capes (Coordination for the Improvement of Higher Education Personnel) in Brazil was accessed via an Internet Protocol (IP) service provided by the Universidade Federal de Santa Catarina.
In the third stage, the following inclusion criteria were set: complete articles available electronically, in Portuguese, English, or Spanish, published between 2019-2023. Reviews, abstracts in event annals, experience reports, dissertations, theses, and studies not related to the objective were excluded. Following the search in the databases, the results were entered into EndNote, where duplicate studies were removed. The articles were then uploaded to the Rayyan web platform 12 to facilitate the organization and evaluation process of the previously defined inclusion criteria. The studies were selected by two researchers independently and simultaneously, in line with the established criteria. In the event of disagreement between the evaluators, a third reviewer in the field was consulted to settle the disagreement.
To extract and categorize the data, an instrument adapted from an integrative review 13 was used with the following items: Author/year; title of the publication; sample and location of the study; objective; methodological aspects, main results, and conclusions; and influencing factors in the work environment that affect nurses' professional practice (positive and negative).
In the critical evaluation step, the studies considered to be of high quality were those with consistent results, an adequate sample, appropriate control, and pertinent conclusions, based on a comprehensive literature review with full references to scientific evidence. Moderate quality studies were those with reasonably consistent results, a sufficient sample, some control, and fair conclusions, based on a comprehensive literature review with some reference to scientific evidence. Low-quality studies have limited evidence, inconsistent results, an insufficient sample, and conclusions that lack a firm foundation 14.
Given the importance of combining methodological quality and evidence strength, the researchers decided to evaluate the studies' level of evidence according to the Johns Hopkins Nursing ¡ Evidence-Based Practice 14, which has the following classification: level 1 - 1.a) experimental study, randomized controlled trial (RCT); 1.b) explanatory mixed methods project that includes only one level 1 quantitative study; 1.c) systematic review of ran- | domized clinical trials (RCTs), with or without meta-analysis; level 2 - 2.a) quasi-experimental study; 2.b) explanatory mixed methods project that includes only one level 2 quantitative study; 2.c) systematic review of a combination of RCTs and quasi-experimental studies, or only quasi-experimental studies, with or without meta-analysis; level 3 - 3.a) systematic review of a combination of RCTs, quasi-experimental and non-experimental studies, or only non-experimental studies, with or without meta-analysis; 3.b) exploratory, convergent, or multiphase mixed methods studies; 3.c) explanatory mixed methods project that includes only one level 3 quantitative study; 3.d) qualitative study; 3.e) systematic review of qualitative studies with or without metasynthesis. Evidence of non-research: level 4 - opinion of respected authorities and/or nationally recognized specialist committees or consensus panels based on scientific evidence, which includes clinical practice guidelines and consensus panels/ position statements, and level 5 - based on experimental and non-research evidence, which include scoping reviews; integrative reviews; literature reviews; quality improvement, program or financial evaluation; case reports; nationally recognized specialist opinion based on experimental evidence.
The data were analyzed qualitatively and the evidence from the primary study was synthesized descriptively. In addition, the evidence was carefully grouped into thematic categories, which provided a structured and coherent organization of the content, facilitating interpretation and understanding of the relationships and patterns identified in the study.
This review used the ROBIS instrument 15 to assess the risk of bias. In step 3, "Assessing the general risk of bias," all domains showed low risk: study eligibility criteria (low risk, considerable effort), study identification and selection (low risk, considerable effort), data collection and study assessment (low risk, with suitable criteria, data extraction, and assessment of risk of bias performed by two reviewers, and extraction of relevant study characteristics and results), and synthesis and results (low risk, unlikely to produce biased results).
Results
Initially, 1,417 records were found in the databases, of which 55 were selected for full analysis, following the established criteria. After rigorous evaluation, 20 primary studies were considered eligible and included in the final sample of this review. Figure 1 shows the steps in the selection process for the primary studies in this integrative review.
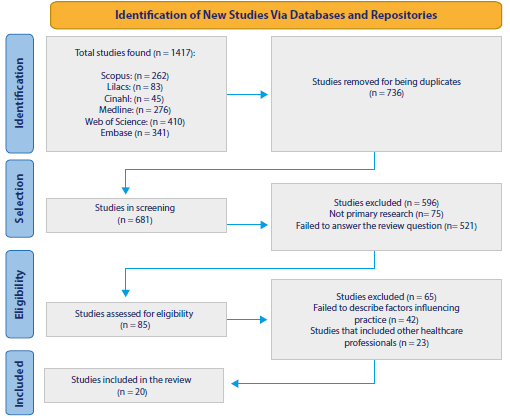
Source: Adapted from Prisma.
Figure 1 Identification and Selection of Publications Based on the Prisma Statement, Florianópolis, Santa Catarina, Brazil, 2023 Flowchart
The final sample consisted of 20 articles, published between 2019 and 2023, with most of them in 2020 (30 %; n = 6), in languages including Portuguese, English, and Spanish with 55 % (n = 11), 40 % (n = 8), and 5 % (n = 1) publications, respectively. These studies were conducted in several countries, such as Saudi Arabia, South Africa, Australia, Brazil, the United States, Spain, Colombia, and Portugal.
Notably, Brazil was the country with the highest number of publications, representing 55 % (n = 11) of the studies. Regarding the methodological approach, it can be noted that qualitative studies comprised 55 % (n = 11) of the sample, quantitative studies comprised 40 % (n = 8) of the contributions, and a mixed-method study represented 5 % (Table 2).
Table 2 Descriptive Synthesis of the Selected Primary Studies, Florianópolis, Santa Catarina, 2023
| Author/year | Objective | Sample/ Country | Type of Study |
|---|---|---|---|
| Barth et aL/2019 (A1) 16 | To analyze the situations that cause moral distress in PHC nurses across different regions of Brazil. | 13 nurses/ Brazil | Qualitative/ descriptive |
| Atehortúa Mira et aL/2019 (A2) 17 | To understand the state of nursing in the implementation of PHC in Antioquia, Colombia. | 13 nurses/ Colombia | Qualitative/ ethnographic |
| Mendonça Moreira et al./2019 (A3) 18 | To describe the factors that trigger dissatisfaction in nurses working in Primary Health Care. | 19 nurses/ Brazil | Qualitative/ descriptive |
| Oliveira et aL/2019 (A4) 19 | To analyze the daily work routine of Family Health Strategy (FHS) nurses who work in rural areas. | 11 nurses/ Brazil | Qualitative/ descriptive |
| Oliveira e Pedraza/2019 (A5)20 | To evaluate the work environment and professional satisfaction of nurses working in the FHS in the state of Paraíba, establishing a comparative analysis between conventional teams and the "More Medical Doctors" Program. | 50 nurses/ Brazil | Quantitative/ cross-sectional |
| Biff et al./2020 (A6) 21 | To identify the elements that contribute to reducing and increasing the workloads of nurses in the FHS. | 40 nurses/ Brazil | Qualitative |
| Halcomb et al./2020 (A7) 22 | To identify the immediate support needs of Australian primary health care nurses during the COVID-19 pandemic. | 637 nurses/ Australia | Quantitative/ cross-sectional |
| Mendes e al./2020 (A8) 23 | To identify the workloads of nursing teams working in the FHS in all five regions of Brazil and their relation to the burnout experienced by these professionals. | 45 nurses/ Brazil | Qualitative |
| Martins et al./2020 (A9) 24 | To understand the motivational factors experienced by nurses at a Health Center Grouping in the Lisbon region. | 9 nurses/ Portugal | Qualitative/ descriptive |
| Matlala et al./2020 (A10) 25 | To establish nurses' perceptions of factors affecting the delivery of quality healthcare services in selected public primary health care clinics in rural areas of the Capricorn District, Limpopo Province. | 155 nurses/ South Africa | Quantitative/ cross-sectional |
| Celestino et al./2020 (A11) 26 | To analyze the psychosocial risks related to the work of FHS nurses and the management strategies required to minimize them. | 18 nurses/ Brazil | Qualitative |
| Abdoh et al./2021 (A12) 27 | To determine the prevalence of stress and its associated factors in primary health care nurses in the city of Medina, Saudi Arabia. | 200 nurses/ Saudi Arabia | Quantitative/ cross-sectional |
| Busnello et al./2021 (A13) 28 | To analyze the incidence of different types of violence in the workplace of nurses in the FHS and the implications for work and workers. | 47 nurses/ Brazil | Mixed/ explanatory-sequential study |
| Ashley et al./2021 (A14) 29 | To explore the psychological well-being of PHC nurses in the context of the COVID-19 pandemic. | 25 nurses/ Australia | Qualitative/ descriptive |
| Albendín-García et al./2022 (A15)30 | To identify the risk factors related to personality variables that can explain the different models of burnout severity and quantify their effect on prognosis at the varying levels of each dimension of the burnout syndrome in primary care nurses. | 242 nurses/ Spain | Quantitative/ cross-sectional |
| Fabri et al./2022 (A16)31 | To verify the association between violence in the workplace and the quality of professional life of nurses in Basic Health Units (BHUs). | 101 nurses/ Brazil | Quantitative/ cross-sectional |
| Felix et al./2022 (A17) 32 | To analyze the work conditions, infrastructure, and management organization of PHC units. | 45 nurses/ Brazil | Qualitative/ descriptive |
| Kueakomoldej et al./2022 (A18)33 | To research nurses' practice environment and workforce outcomes, including burnout, turnover intention, and job satisfaction in community health centers. | 269 nurses/ United States | Quantitative/ cross-sectional |
| Viana e Ribeiro/2022 (A19) 34 | To understand how nursing professionals describe aspects that interfere with their work in the FHS. | 10 nurses/ Brazil | Qualitative/ descriptive |
| Wali et al./2023 (A20) 35 | To measure the job satisfaction of nurses working in the National Guard's Primary Health Care Centers and to identify the varying sources of pressure in their workplace. | 77 nurses/ Saudi Arabia | Quantitative/ cross-sectional |
Source: Prepared by the authors.
Regarding the assessment of the level of evidence, it was noted that most publications, i.e., 55 % (n = 11), were classified as level 3.d. For a more comprehensive overview of the characteristics of the studies that composed the final sample, Table 3 shows the main results and the methodological quality of the selected studies.
Table 3 Information Regarding the Main Results and Conclusions, Level of Evidence, and Methodological Quality of the Studies, Florianópolis, Santa Catarina, 2023
| Study | Main Results and Conclusions | NE* | Methodological quality |
|---|---|---|---|
| (A1) | The work conditions, the organization, the professional and interpersonal relationships, the conflicts in these relationships, and the forms of healthcare management are the triggers for moral distress. | 3.d | Moderate quality |
| (A2) | Professionals are faced with personal, professional, and work-related events that influence their commitment, both in terms of persisting and continuing to work and of quitting and abandoning the processes. | 3.d | Moderate quality |
| (A3) | Nurses' satisfaction is closely related to their profession. Dissatisfaction is caused by poor work conditions, factors such as work overload, lack of physical and material resources, inappropriate infrastructure, and professional undervaluation, among others. This can result in chronic stress and illness. | 3.d | High quality |
| (A4) | Nurses in rural areas have an intense relationship with the population, but their daily work is surrounded by several organizational barriers, ranging from the team's commute to the workplace to the operationalization of health measures, all of which are mediated by the aspects of rurality. | 3.d | Moderate quality |
| (A5) | Critical work organization conditions negatively influence job satisfaction, with problems in the management of the work process that target increased productivity. | 3.a | Moderate quality |
| (A6) | The elements that influence the increase in workloads the most are the precariousness and structural deficits in the work environment, materials, and equipment, in addition to the numerical deficit in the workforce and the excessive demand for care. | 3.d | High quality |
| (A7) | Core issues related to health, personal safety, quality of care, and job security need to be addressed to better support and help retain nurses and optimize their role in primary health care during a pandemic. | 3.a | High quality |
| (A8) | The workloads were related to structural and managerial problems, especially the psychological ones due to excessive demand and lack of professionals; the physiological ones due to the overload of tasks that generate physical pain and exhaustion; the physical and mechanical ones due to inadequate work environments and equipment; the biological ones due to the presence of microorganisms; and the chemical ones due to exposure to dust and fumes. | 3.d | High quality |
| (A9) | The main motivating factors for nurses are rewards, nursing career development, recognition, workplace/practice environment, performance-based funding, leadership, and professional fulfillment. Career development was the most important factor. | 3.d | Moderate quality |
| (A10) | The quality of healthcare services is still hindered by several factors, such as the overwhelming workload, the team's behavior and the hygiene of the work environment, the precarious infrastructure and the fact that nursing professionals perceive the environment as lacking in equipment. | 3.a | High quality |
| (A11) | Psychosocial risks related to the work environment were identified: insufficient professional training, compromised interpersonal relationships, work-family interface and psychological violence; and those related to the work content: insufficient work equipment, lack of human resources, and extensive workload. | 3.d | High quality |
| (A12) | Stress was found to be prevalent among nurses (9.5 % mild stress, 12 % moderate stress, and 30 % severe or very severe stress). Occupational stress was correlated with factors related to the work, the organization, and the system. | 3.a | High quality |
| (A13) | FHS nursing professionals are constantly exposed to violence in their work environment, with episodes of aggression that lower their satisfaction with the workplace. All types of harassment are more difficult for professionals to perceive and report. | 3.b | High quality |
| (A14) | The psychological impact caused by negative experiences increased anxiety and stress levels. | 3.d | High quality |
| (A15) | The high demand for care overloads professionals, in addition to a lack of human and material resources and job dissatisfaction, which affects physical and psychological health. | 3.a | High quality |
| (A16) | Violence in the workplace was associated with quality of occupational life since low satisfaction with compassion was related to moral harassment and the lack of encouragement to report violence, and secondary post-traumatic stress was associated with physical violence and the absence of standardized procedures in the face of violent incidents. | 3.a | High quality |
| (A17) | The shortage of professionals to manage primary care services places a heavy burden on nurses, who have to accumulate the responsibilities of providing care to health service users and organizing administrative demands. | 3.d | Moderate quality |
| (A18) | Primary care nurses rated their practice environments positively and more than 89 % reported satisfaction with their work. | 3.a | High quality |
| (A19) | Overwork and professional depreciation demotivate, frustrate, and compromise the performance and emotional health of nursing professionals working in the FHS. | 3.d | High quality |
| (A20) | Due to the vital role of nurses in patients' lives, sources of dissatisfaction and pressure in nurses' work must be addressed and managed. | 3.a | High quality |
*LE: Level of evidence.
Source: Prepared by the authors.
Based on the studies analyzed, the thematic categories that emerged were "psychological and emotional elements," "human resources, materials, and infrastructure," "interpersonal relationships," "dissatisfaction," "violence in the workplace," and "overload." These thematic categories are key to understanding the triggering factors that influence nurses' performance in the workplace (Table 4).
Table 4 Thematic Categories and Triggering Factors that Impact Nurses’ Professional Practice
| Thematic Categories | Sub-Themes | Triggers | Implications for Practice |
|---|---|---|---|
| Psychic and emotional elements 22,24,27,29 | Stress | Interaction with patients and their families. |
|
| Instances of bullying in the workplace. | |||
| Increased work hours. | |||
| Emotional exhaustion | High levels of demands associated with their employment conditions. | ||
| Human resources, supplies, and infrastructure 1,7-26,30,32 | Employee deficit | High demand for care and overload. |
|
| Long work hours. | |||
| Job deviation. | |||
| Reorganization of the work process. | |||
| Resource shortages and precariousness | Insufhcient or non-functional work equipment and material resources. |
|
|
| Inadequate physical structure | Inadequate ofhces to provide healthcare services. |
|
|
| Dimly lit rooms and locked halls. | |||
| Increased humidity, insects, and poor ventilation. | |||
| Interpersonal relationships 16,17,20-24,30 | Professional- professional | Distribution of responsibilities in teamwork. |
|
| Better local communication between team members. | |||
| Team relationship. | |||
| Professional- manager | Increased support from managers in the workplace. | ||
| Recognition from management. | |||
| Dissatisfaction 16-18,20,32,33,35 | Low pay | Job precarization. |
|
| Increased turnover intention. | |||
| Downgrading | Recognition. | ||
| Violence in the workplace 26,28,31 | Physical violence | Patient aggression. |
|
| Lack of safety in the workplace. | |||
| Moral harassment | Exposure of nurses in media such as radio and social networks. | ||
| Taunts and intrigue. | |||
| Overload 16,19,23-25,34 | Increased work hours | Overload of care and management tasks. |
|
| Increasing population demands. |
Source: Prepared by the authors.
Discussion
The methodological process integrated data that enabled the identification of aspects related to the work environment that have an impact on nurses' practice in PHC. Considerable research was found in this field, especially in the Brazilian context. The evidence found reflects that several elements of the work environment influence and correlate with the work of PHC nurses and have an impact on productivity, organization, planning, and healthcare measures directed to the population. One of the main factors is related to the psychological and emotional elements faced by workers when performing their duties. Among these factors, stress stands out as a key point, triggering adverse effects on the daily work routine 24,27,29.
Studies show that constant interaction with patients and their families is a significant source of stress, resulting in frustrations that have an impact on the professional experience 27,36. Closeness and empathy in the relationship with patients are essential characteristics for providing effective healthcare, but this level of closeness can also trigger emotional challenges, highlighting the complex and diverse nature of the demands presented by patients in PHC. When faced with a range of health conditions and social and emotional needs, nurses can feel overwhelmed and stressed, especially when the expectations of patients and their families are high 37. Similar to these findings, a study with 295 nurses found that the stress resulting from this continuous interaction can have a significant impact on nurses' mental health, contributing to emotional exhaustion, anxiety, and even burnout symptoms 38.
In addition, it was found that the pressure to avoid errors and the increased work hours can also contribute to increased psychological stress, affecting the quality of life in the workplace. It is worth noting that these problems have become even more evident in recent years, particularly due to the COVID-19 pandemic. The global health crisis has intensified stress levels, heightening the pressure already present in nurses' work environments 22,39. This not only affects the emotional well-being of professionals but can also result in physical consequences such as chronic fatigue, sleep disturbances, and other stress-related health problems 40.
Studies show that the constant pressure to avoid errors is an intrinsic aspect of the healthcare field, especially for professions such as nurses 25,41. The critical nature of the decisions made in patient care amplifies this pressure. The permanent pursuit of precision and excellence, although essential, can create a stressful workplace, where professionals face a significant burden of responsibility for every decision and action taken 40.
Regarding the work environment, several elements contribute to the complexity of nurses' work, and the conditions associated with human, material, and infrastructure resources have a significant role in determining the performance of professionals and the efficiency of the healthcare services provided 17-26,30,32. Staff shortages are a persistent reality that has a direct impact on teams' ability to provide quality healthcare. The high demand for care, combined with the shortage of professionals, results in an overload on the nursing staff, with negative effects on productivity, the achievement of work objectives, and the effectiveness of healthcare measures 18,23,26.
The poor physical structure of healthcare units, such as insufficient consultation rooms, entails additional challenges. Three studies cited the challenge of providing individual appointments in privacy and the need to adapt to these work conditions, as such issues emerge due to inadequate infrastructure 21,24,32. Another study indicates that this problem is quite recurrent, especially in regions and locations where budget limitations and the demand for healthcare services are more pronounced 42.
This review highlights the interaction between healthcare professionals and the allocation of responsibilities in teamwork as key factors. Improving the work process, encouraging cooperation, and promoting regular meetings are elements that contribute to the quality of care 21,22,24. This finding is in line with another study which indicates that encouraging regular meetings is a productive strategy for fostering efficient communication between healthcare team members. These meetings provide a dedicated space for discussing cases, exchanging information, clarifying doubts, and joint planning 24,43. In addition, encouraging cooperation between team members in PHC is essential for cultivating a collaborative environment, where individual skills are leveraged in favor of patient care 44.
Support from managers in the work environment and recognition of the importance of these environments by leaders are factors that have a direct impact on job satisfaction. Increased support leads to a healthier and more motivating working environment, promoting nurses' well-being 16,19,24. In turn, low pay and precarious work conditions lead to professional dissatisfaction, hindering continuing education, continuity of care, and generating a tendency of turnover in nursing 32.
The data provided in the articles analyzed are in line with that in the literature, corroborating the understanding that inadequate pay and precarious working conditions are determinant factors for professional dissatisfaction in the nursing field and consequently affect the practice and dynamics of work in PHC 18,45. The discrepancy between the load of responsibilities, the complexity of tasks, and financial compensation adds to professional frustration and dissatisfaction. This can result in delays in tasks, planning, and the continuity of care provided to the population in PHC 18. This factor correlates with higher odds of intention to quit the profession among nurses working in PHC. The search for better opportunities, both financially and in terms of professional quality of life, becomes an option for dissatisfied professionals 35,46.
In terms of violence in the workplace, the summary presented shows that this is a significant aspect that influences nurses' work in PHC 28,31. Aggression and physical violence by patients cause anguish and mental suffering, and interfere with sleep, creating a work environment permeated by fear and hindering professional-patient interaction 26.
The need to face assaults not only affects nurses' individual health but also the dynamics of the team and the quality of care provided. In addition, the lack of safety in the PHC environment is a constant concern highlighted in studies on the impact of violence in the workplace 47. The lack of effective security measures increases the vulnerability of professionals to violent events, increasing the risk of incidents that are harmful to their physical and emotional integrity 48.
Meanwhile, the overload caused by the increase in work hours and the accumulation of care and management tasks leads to negligence, a drop in productivity, and interference in the planning and execution of health care 23,25,34,35. Increased work hours, often the result of long shifts and growing demands in healthcare services, contribute to nurses' physical and mental exhaustion (18). Studies indicate that the fatigue resulting from this exacerbated prolongation of work hours is directly associated with a higher susceptibility to making mistakes, and a decrease in attention and concentration, which compromises the ability to make decisions and perform tasks accurately 35,49.
In addition, the work environment in PHC is becoming increasingly challenging. Nurses and everything that surrounds their daily work must be considered, as the settings in which they perform their duties can have a significant influence on their performance and professional well-being. Healthy environments tend to result in more efficient and satisfactory work for the staff, as well as having a positive impact on health outcomes in PHC 50.
It is worth noting that although there are publications evaluating the work environment in PHC 51,52, these studies do not focus specifically on nursing and do not associate the work environment with the triggering factors that influence nurses' performance in this setting. In addition, the period of the reviews and the focus of analysis also differ from the objectives of this study.
Conclusions
This literature review has identified the various elements of the work environment that have a negative impact on nurses' work in PHC. Aspects such as precarious work conditions, an overload of tasks, a shortage of human and material resources, inadequate management, and the incidence of violence at work have negative repercussions not only on productivity, but also on the quality of care provided, on nurses' mental health and, consequently, on the services provided to the community.
It is therefore vital to implement measures aimed at improving the workplace for nurses, ensuring excellence in the care provided in PHC, and preserving the health of professionals and, by extension, the population they serve. Investing in infrastructure improvements in healthcare units, increasing the number of nursing professionals, and providing more suitable work conditions are key measures to mitigating work overload, reducing stress levels, and promoting professional satisfaction.
Study limitations
Among the limitations of this study, it is worth noting the delimitation of the publication period to the last five years preceding the study and the consideration of the diverse realities faced by nurses in different countries, especially in the PHC setting. The diversity in healthcare structures, government policies, available resources, and organizational culture between countries can result in different realities in terms of understanding the work environment of nurses. It is also worth noting that the studies analyzed were restricted to publications in Portuguese, English, and Spanish.

