











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Chronic kidney disease (CKD) is considered a public health problem (1). The global prevalence of patients with CKD who require renal replacement therapy has increased over the years. In Brazil, among the treatments available for CKD in its final stage, hemodialysis (HD) is the most used (92%) and it requires important adaptations in the life of the patients, as it consists of a treatment associated with several restrictions that compromise their daily activities (2).
Patients with CKD, who are undergoing HD, present a decrease in their functional capacity, causing damage to both, their physical and mental health. (3, 4). Functional capacity is defined as the ability to take care of themselves in daily tasks, which can be described as basic activities of daily living (BADL) or instrumental activities of daily living (IADL) (5,6).
The division into basic and instrumental activities began with the studies by Katz et al. and Lawton et al. respectively (5, 6). The authors presented two functional assessment scales that classified daily activities according to the level of complexity. Lawton and Brody developed a scale to assess IADL with eight activities (5). The scale of Katz is one of the instruments used to assess BADL and it also assesses the functional capacity of older individuals (6). This instrument sets out six categories that are related and reflect development patterns.
Patients undergoing HD suffer numerous physical and emotional symptoms that reduce their comfort and quality of life (7, 8). After the session of HD, many patients report feeling very tired, a condition which is conventionally called post-dialysis fatigue (PDF), described as a debilitating symptom, and viewed as more important than survival for many patients (9, 10). PDF is described as a distressing complaint, in which patients report tiredness and a need for rest or sleep, it is believed to be different from that associated with other treatments. Fatigue is a subjective sense of weakness, lack of energy and tiredness (10). Other common complaints include weariness and exhaustion. As it is a debilitating and frustrating symptom, it deeply interferes with the daily quality of life of the patients (11).
In the pioneering studies of Sklar, patients were asked the question: “Do you feel better or worse after the dialysis session? If worse, please specify how”. Those who responded that they felt worse after dialysis, were diagnosed with PDF. The fatigue complaint would then be investigated with questions directed to its duration, frequency, and intensity (9). The question “how long does it take to recover from a dialysis session?”, is interpreted easily by patients and should be considered a standard question in HD-related studies (12). In a recent study, Bossola et al add a score of 1 to 5 to measure the intensity of the PDF (13).
The lack of a trustworthy, valid and sensitive fatigue scale complicates the precise identification of the symptoms (10). This symptom may be correlated with sociodemographic factors, functional capacity, clinical and psychological variables, and factors related to dialysis (9, 14). The SF-36 vitality subscale can be used, but it fails to capture the negative aspects of fatigue. The high prevalence of the symptoms and the impact on overall quality of life, may explain why fatigue is one of the outcomes for patients receiving HD (15). More recently the Standardized Outcomes in Nephrology- Hemodialysis Fatigue (SONG-HD), suggested that three questions should be asked, with a timeframe of the past week, rating them in a Likert scale from zero (not at all) to three (severely) (16). A better understanding of the factors related to this symptom will help to plan strategies for the management of PDF. Therefore, this study aims to evaluate the relationship between post dialysis fatigue in performing basic and instrumental activities of daily living in HD patients.
Method
It is a cross-sectional study with a quantitative approach, carried out at the Dialysis Unit of Hospital São Lucas da Pontifícia Universidade Católica do Rio Grande do Sul. Based on the percentage of fatigue estimated at 60% (0.6) in this population and considering a sampling error of 0.01, the sample calculation was 98 participants. Inclusion criteria were patients over 18 years of age with CKD who underwent HD and agreed to participate to the study. The study was approved by the Research Ethics Committee. All participants signed the informed consent form. The STROBE checklist was used in the reporting of the study.
Data collection was carried out in January and February 2020, at the beginning of the HD sessions and done by the researchers themselves. Three instruments were used, in addition to access to the electronic medical record of the patients. An instrument with patient identification information, sociodemographic and clinical variables, and dialysis session data was used. In this same instrument, the presence of fatigue was evaluated with the following question “Do you feel better or worse after the dialysis session?” where patients who responded that they felt worse were classified as having fatigue. Then the participants were asked about the symptoms experienced in the post dialysis and recovery time of the session, the transdialysis symptoms on the day of the collection and in the last three sessions were collected from the electronic medical record.
Although there are studies that try to categorize the degree of fatigue after dialysis, the variability in the way fatigue is measured and reported makes it difficult to compare the effect. To our knowledge, a specific scale for patients on hemodialysis has not been established and validated in Brazil (9, 11, 15, 17).Therefore, in this study, it was decided to carry out the assessment of fatigue by the question mentioned above, and not using questions directed to the duration, frequency, and intensity of fatigue. The SONG-HD Fatigue instrument was published after this study was conducted (16).
The second instrument used was the scale of independence in activities of daily living (Katz Scale), which assesses the degree of dependence in six functions, namely: bathing, dressing, using the toilet, transference, continence and feeding; in which its score ranges from zero to six points, with zero being independent in the six functions and six being dependent in all six functions.
The third instrument is the scale of instrumental activities of daily living (Lawton Scale), which assesses the degree of dependence in nine functions, namely: use of the telephone, transport, shopping, preparing meals, tidying the house, work household, washing and ironing clothes, use of medicines and managing money; where the score for each item varies from three to one, with three being able to perform without help, two being able to perform with partial help and one, unable to perform.
Descriptive and inferential statistics were used, where continuous variables were presented by measures of central tendency (mean and median),variability (standard deviation and amplitude) and, categorical variables as absolute and relative frequency. Data normality was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests, and Pearson's Chi-square test was performed to assess the association of data. The level of significance was p<0.05. Data analysis was performed using the Statistical Package for Social Sciences (IBM SPSS) version 22.
Results
From the 111 patients in the unit at the time of collection who met the established inclusion criteria, 10 did not accept to participate in the study, where six did not show interest in the topic, one was undergoing dialysis in the intensive care unit, two had Alzheimer's and one died. Ending with a sample of 101 participants. Table 1 shows the sociodemographic variables of the participants, and their association with the presence or absence of FPD. From the 101 patients interviewed, 63 (62.4%) had PDF. Recovery time after HD session had a median of 3.5 hours with a minimum of 0 and a maximum of 24 hours. The presence of PDF had statistical significance as longer time on HD in months (p<0.041), longer recovery time after the session (p<0.001) and dialysis during day shifts (p<0.013). There was no association of PDF with the other variables. A multivariate analysis confirmed the association of presence of fatigue in the morning shift (p=0,005), cramps on the dialysis day (p=0,034), and tiredness (p<0,001).
Table 1 Sociodemographic and clinical categorization of the sample, with the association of variables and the presence or absence of Post Dialysis Fatigue. Porto Alegre, 2020 (n=101)

Note: Pearson's Chi-square test; **Fischer's exact test; $Mann Whitney Test &Student's T Test
Source: the authors
The most frequent transdialysis symptoms on the day of the interview and in the last three sessions, were hypotension, cramps, headache, and tiredness. As for symptoms related to PDF; fatigue, dizziness, weakness, and hypotension stood out. The other items and scores referring to symptoms are shown in table (Table 2), where the tiredness symptom (p < 0.032) was statistically significant.
Table 2 Association between the main symptoms reported with the presence of post dialysis fatigue . Porto Alegre, 2020 (n=101)

Note: P: *Fischer's exact test; **Student's T-test.
Source: the authors
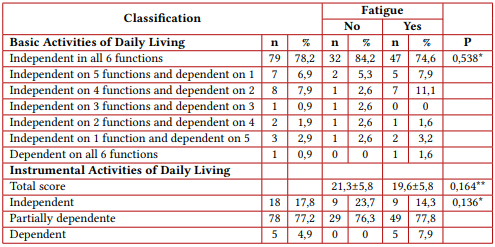
In the BADL Assessment (Table 3), the item with the highest degree of dependence was dressing up, followed by taking a shower, continence and transfer. Regarding the IADL (Table 3), the activity in which patients scored the most in the “without help” category was using the telephone. In the “partial help” category, the most scored activity was tidying the house, and in the “I can't” category, washing and ironing clothes predominated. Table 3 shows the association between the classification of the instruments and the presence or absence of PDF. We did not find a statistically significant difference in the association between fatigue and the assessment instruments for activities of daily living and activity of instrumental life.
Table 3 Relationship between the classification of instruments used to assess the degree of dependence and the presence of fatigue. Porto Alegre, 2020 (n=101)
Source: the authors
Variables with p<0.2 in univariate and bivariate analyses, were included in the regression model (session shift, education level, months on hemodialysis, headache, cramp, fatigue, session recovery time in hours, and total score of instrumental activities of daily living). Subsequently, variables without statistical significance in the first step of the analysis were excluded (level of education, months on hemodialysis, headache, session recovery time in hours, and total score of instrumental activities of daily living). In the final analysis, the following variables remained independently associated with fatigue. Performing the hemodialysis session in the morning increases the prevalence ratio (PR) of fatigue by 39.2% (95%CI from 10.6% to 75.2%) compared to its performance at night (p=0.005). Having cramps during the procedure increases the PR of fatigue by 64.9% (95%CI from 3.8% to 162.0%) (p=0.034). Feeling tired during the session increases the PR of fatigue by 424.7% (95%CI from 205.2% to 802.0%) (P<0.001) (see Table 4).

Discussion
The present study found that more than half of the patients on dialysis had PDF, which was not statistically associated with dependence on BADL or IADL. The mean age of the population studied was 59±7, where the majority were men; data that is in agreement with the current Census of the Brazilian Society of Nephrology (2). As it is a predominantly male sample, the items “tidying the house” and “washing and ironing clothes” obtained higher scores in the category “I can't”. According to the Lawton scale validated by the Ministry of Health in the Basic Care Notebook for aging and health of the elderly, there may be variations in these items according to sex and can be adapted to other activities, but which were not suitable in this study (18).
Bossola (20), in a prospective and multicenter study, found an association between age of participants (71.5±12.7 years), ABVD and session recovery time (6.3 hours), where the Sklar (9) study was used to identify fatigue, which corroborates with the findings of our study. In another study by the same author, which aimed to investigate the relationship between PDF and dependence on BADL and IADL, this was significantly higher in patient’s dependent on BADL. Although this study found an association of FPD with ABVD and IADL, the dialysis, hematocrit and Kt/V variables were similar to our study (19), biochemical markers as albumin, creatinine, Kt/V, urea reductions ratio have been inconsistent in association with fatigue (10). In a recent study, 164 patients from five hemodialysis units were included, and PDF was found in 60.5% of them, the median time to recover was 180 minutes; both findings similar to our study.(13)
The time required for post-dialysis recovery is similar to that found by Sklar, who reported the need for an average of 4.8 hours of rest or sleep for the symptoms of fatigue to pass within an interval of 0 to 24 hours (9). According to the study by Davenport, the recovery time presented was 1-4 hours, in the multivariate analysis (21). Unlike our study, recovery time greater than 1 hour was more common in women, with reports of previous depression and history of antidepressant use, variables that were not evaluated in the present study (20).
According to Lindsay, the answer to the question, "How long does it take you to recover from a dialysis session?" is easily interpreted and sensitive to changes, so it should be considered a standard question in HD-related studies in which the result of health-related quality of life is examined (21). Some studies bring the assessment of fatigue through a question and others try to quantify the intensity of fatigue through scores. However, it is important to have uniformity in the assessment and reporting of this symptom, and so far, there is no consensus, rather there is a diversity in the ways to assess fatigue that makes it complicated to compare and interpret results (15, 22).
The study of Sklar, evaluating different types of therapy (isolated ultrafiltration, hemodiafiltration and hemodialysis) found a higher frequency of FPD in patients who underwent hemodialysis or isolated ultrafiltration sessions (17). Nonetheless, in the present study, these parameters were not evaluated, as isolated ultrafiltration and hemodiafiltration are not performed at the study site. Still on the findings of Sklar, there was a high frequency of headache among all types of treatments, and PDF was statistically more associated with dizziness and cramps than with nausea and headache (17). These symptoms are frequently found as transdialysis complications, regardless of the presence of fatigue, and they are also found in previous publications carried out in the same place as this study (25, 24).
Considering that the definition of fatigue is a distressing complaint, in which patients report tiredness, weariness and exhaustion; when the main reported symptoms are associated with the presence or absence of PDF, the tiredness symptom became statistically significant in this study. It was not surprising to find that patients who undergo dialysis in the night shift have fewer reports of fatigue, given that they leave dialysis straight home and sleep, minimizing symptoms, tiredness, and sleepiness as a post-session complaint; differently of those who still have the whole day ahead of them. Lindsay et al. reported that patients doing nocturnal dialysis had a shorter recovery time after a dialysis session corroborating with our findings (21).
Studies that address the treatment of PDF are still recent, considering specific issues of the profile of patients with CKD, so it is not only important to identify, but also to implement treatment strategies at the nursing level that can minimize the presence of this symptom. One of the possibilities listed by Tsay, was acupressure on the feet and legs, which showed positive results in patients who received this technique. Acupressure is a non-invasive alternative therapy that employs pressure and massage at specific points that stimulate brain chemistry by affecting the release of neuropeptides, it activates opioid systems providing pain relief, and accelerates the transmission of electromagnetic signals that can activate the flow of endorphins and monoamines and, in turn, reduces the levels of agitation and nausea; thus, enabling a better quality of life. This study is important for health professionals, as it offers an alternative way to help manage the presence of fatigue (25).
The term fatigue is present in all specialties, however, it is necessary to establish a standardized approach for the assessment of this symptom aimed at patients undergoing HD, considering their clinical variables and degree of dependence, as some studies show an association with this data.
A recently published paper has suggested the use of an instrument to assess fatigue, however the data from this study was collected before the publication (16). As this is a cross-sectional study and is limited to evaluating a single population in Brazil, even if the sociodemographic and clinical characteristics are in line with the Brazilian census of nephrology, it is necessary for more studies to be carried out to know whether these data represent the Brazilian population in HD.
Conclusion
More than half of HD patients have PDF, its presence is lower in patients who undergo dialysis during the night shift, and it is significantly associated with the vintage on HD, with longer recovery time from the session. No association was found with other treatment variables, BADL and IADL. This study expands our knowledge about HD and fatigue, describing the symptoms involved so that interventions can be studied in the future, to reduce the impact of fatigue, in addition to creating a score that standardizes this assessment.

