











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The definition of Rheumatoid Arthritis has been documented in the medical literature for more than two hundred years, but its etiology remains unknown (Entezami, Fox, Clapmam and Chung, 2011. Despite the fact that infectious agents such as viruses, bacteria and fungi, as well as environmental components like tobacco addiction, and even genetic factors have been regarded as causal factors, none of them has proven to be the cause of this disease (Julia and Marsal 2013; Pratt and Isaacs, 2015).
Rheumatoid Arthritis affects approximately 1% of the world's population, and the consequences for the person's health as the disease progresses are loss of joint mobility, deformity, disability, chronic pain and the presence of negative emotions such as anxiety, depression, stress and hopelessness (Gibofsky, 2012; Santiago, Geenen, Jacobs & Da Silva, 2015; Zhao, Chen & Chen, 2015), in addition to physical and emotional dependence, fatigue, morning stiffness and sleep disorders, among other ailments (Purabdollah et al., 2015).
In Colombia, epidemiological studies have estimated a prevalence of RA between 0.8 - 1.0% of the population. The average age of appearance of the disease is 53.2 years and for the onset of symptoms is 41.3 years, with higher prevalence in women (8 l. 9%); co-morbidity is associated with essential hypertension, osteoporosis, and Sjogren's syndrome (Bautista et al., 2015; Machado, Ruiz & Medina, 2015).
Rheumatoid Arthritis therefore implies a major change in the health-related quality of life (HRQOL) for people who suffer from it (Matcham, Scott, Rayner & Hotopf; Akiskal, 2014). HRQOL is the assessment that a person makes, in accordance with its own criteria, of their physical, emotional and social state at a given time, and reflects the degree of satisfaction with a personal situation at a physiological level (general symptomatology, functional disability, analytical situation, sleep, sexual response) emotional level (feelings of sadness, fear, insecurity, frustration) and social level (work or school situation , social interactions social in general, family relationships, friendships, economic level, participation in the community, leisure activities, among others) (Schwartzmann, 2003).
The person with a diagnosis of Rheumatoid Arthritis must face, not only the symptoms associated with the disease, but the ambiguity of these (Purabdollah et al., 2015), Since Rheumatoid Arthritis is one of the main conditions that most diminishes quality of life (Garip, Eser & Bodur, 2011). However, the prevalence of symptoms in situations of physical and functional deterioration does not exclude the presence of positive emotions such as happiness, which serve as protective frames for the physical and mental health of patients with chronic medical conditions (Angner, Ray, Saag & Allinson, 2009; Angner, Ghandhi, Purvis, Amante and Allinson, 2013; 2015).
According to Palomera (2009) "happiness is composed of three dimensions: positive emotions, negative emotions and vital satisfaction." "Happiness is the result of the degree in which the experiences of positive affectivity exceed experiences of negative affectivity and the degree in which a person perceives that his/her goals and motivations are resolved (p. 273)". In addition, the ability to maintain positive emotionality during periods of illness has also been associated with a better welfare (Lyubomirsky, Sheldon & Schkade, 2005; Steptoe & Wardle, 2005). The literature is consistent in affirming the positive relationship between quality of life and happiness in health (Musschenga, 1997)
On the other hand, cognitive and emotional factors play an important role in the perception the patient has of his disease, influencing the development and course of the same. The perception of the disease refers to a cognitive and emotional representation that the patient makes of his condition, whereby if this implies a threat to his/her health, the representation orients the actions and the use of coping strategies to deal with the disease (Quiceno & Vinaccia, 2010).
In this regard, the perception of the disease is related to a number of outcome measures in Rheumatoid Arthritis, including disability, low mood, pain and decline in physical function (Prajapati et al., 2014). It can even delay the search for medical treatment, which may exacerbate the symptoms of the disease and lead to long-term loss of several functions of daily life such as the ability to travel, personal care, work capacity, financial independence and participation in social roles, among other basic activities (Van der Elst et al., 2015). In different studies, a directly proportional relationship between HRQOL and the percep tion of illness has been found (Quiceno & Vinaccia, 2010).
According to the above, the aim of this study was to evaluate the relationships between quality of life related to health, the perception of disease, happiness, anxiety and depression in 62 patients with a diagnosis of rheumatoid arthritis, residents in the city of Bogotá.
METHOD
Participants
62 adult patients (men and women) participated in this study with a diagnosis of rheumatoid arthritis according to the classification criteria for this disease of the year 2010. The sample was selected through a non-random sampling of the available subjects, who attended a foundation of the city of Bogotá, which provides support to the rheumatic patients. Inclusion criteria were being 18 years or older, not having any diagnosis of cognitive impairment and accepting freely and voluntary to participate in the the investigation.
Instruments
Quality of Life in Rheumatoid Arthritis Scale, QOL-RA The QOL-RA is a specific questionnaire that evaluates the HRQOL of patients with arthritis Rheumatoid. It was origi nally developed and validated to Spanish by Danao, Padilla and Johnson (2001). Cronbach alpha coefficients for this instrument range from 0.87 to 0.90. The Colombian version by Vinaccia, Riveros, Quiceno, and Anaya was used in this research (in press). This scale contains eight items where each one constitutes a dimension, thus a Cronbach Alpha analysis is not carried out. Its eight dimensions are: physical ability, support, pain, stress, health, arthritis, social life and mood; in addition it contains a full scale. The response system is Likert type ranging from 0 (very poor quality of life) to 10 points (excellent quality of life), where the higher the score, the better perception of HRQOL. Cronbach's alpha coefficient for the total scale for this study was 0.949.
The Brief Illness Perception Questionnaire, IPQ-B
Originally developed by Broadbent, Petrie, Main and Weinman (2006). It contains eight items where each one makes up a dimension, and therefore a Cronbach Alpha analysis is not conducted. The response system is Likert type ranging from 0 to 10 points. The dimensions are: consequences, duration, personal control, treatment control, identity, worry, emotional response and understanding of the disease.
Subjective Happiness Scale, SHS
Developed originally by Lyubomirsky and Lepper (1999), possesses a high level of reliability (a <.80). It is comprised by four items that are answered through a Likert system that goes from 1 to 7 points, where the higher the score, the better the subjective perception of happiness. The Cronbach's alpha coefficient for this study was .711.
The Hospital Anxiety and Depression Scale, HADS
The Colombian version of the HADS scale was de veloped by Rico, Restrepo and Molina (2005) with a Cronbach's alpha coefficient of .85. It includes 14 items that are answered in a Likert type system with 4 response options ranging from 0 to 3 points, and has two dimensions that evaluate anxiety and depression related to the current period. The range for each dimension goes from 0 to 21 points, where the higher the score, the higher the level of anxiety or depression. Cronbach's alpha coefficient for this study was 0.824 for anxiety and 0.795 for depression.
Procedure
After obtaining the consent and acceptance from the managers and the Scientific Committee of the foundation that supported the research, patients were invited to participate in the study. Those who accepted the invitation were assembled on the premises of the foundation in groups of maximum 20 people. The purposes and scope of the research were clarified to each group in order for them to sign the informed consent freely and voluntarily. Later, in a self administrated manner and counting with the help of the researchers in charge of the study when patients required it, each patient answered the questionnaires (QOL-RA, IPQ-B, SHS and HADS) and a socio-demographic data sheet. Application time for each participant was one hour on average.
RESULTS
The results of the study were analyzed through the statis tical package SPSS version 22. For the descriptive analysis of the variables age, time of diagnosis, happiness, anxiety and depression, perception of illness and HRQOL, the average was used as a measure of central tendency. Likewise, the standard deviation (D.T. =1.17) and the minimum (min.) and maximum (max.) scores of the different dimensions of the psychometric instruments used were calculated. With regard to nominal variables (sex, marital status, educational level, socio-economic status, occupation, with whom he/ she lives, health system, taking specific medications for the disease or for psychiatric ones) percentages were used.
Additionally, the Cronbach's alpha coefficient was used for the reliability analysis of the psychometric instruments applied in the study. The Pearson's r coefficient was calculated for the correlation analysis between age and time of diagnosis (demographic variables) and for the different dimensions of the questionnaires of quality of life related to health (QOL-RA, IPQ-B, SHS and HADS), having previously calculated the distribution of variables (Kolmogorov-Smirnov). Finally, a multiple linear regression model was employed considering the selection method by steps to analyze the weight of the predictor variables such as age, time of diagnosis, happiness, anxiety and depression and perception of disease on HRQOL (criterion variable)
Descriptive Analysis according to sociodemographic characteristics
Table 1 presents the descriptive data of the socio-demo-graphic and clinical variables of the research. In this study, a prevalence of the female sex over the male can be appreciated, with an average age of 59.7* years and a range between 32 to 79 years. There was a predominance of the sample in the categories married and separated/divorced according to marital status. Most of them achieved an educational level of basic secondary (high school) and belong to a Colombian medium low socioeconomic status (level 1, 2 and 3). Similarly, a great portion of the sample were retired from their working life and a smaller percentage was dedicated to household activities. In addition, a large proportion of the participants lived with relatives and there were very few who lived on their own. With respect to clinical variables, it is observed that patients had 17 years average of having been diagnosed with AR, within a range from 2 to 60 years. Most were covered by a health insurance system (health promotion company), did not take psychiatric medication but did follow a specific treatment for their disease.
Table 1 Sociodemographic characteristics of the sample (n=62)

Nota: n= Number of participants; D.T= Standard deviation; Min= Min.; Max .= Max.
Table 2 presents the descriptive data obtained from the instruments used in table 2.
Table 2 Descriptive statistics of happiness, anxiety, depression, perception of illness and HRQOL variables

Note: n= number of participants; D.T= Standard deviation; Min. = Min.; Max.= Max.
At a general level, there was a level of reliability, from acceptable to very good, in different dimensions and full scales of the psychometric instruments used in the study as shown in table 2.
Regarding the descriptive results shown in table 2, it is observed that happiness (SHS), had an average score. With respect to the HADS scale, according to the criteria of Rico et al. (2005), in order to indicate if patients in Colombia present these symptoms or not, this study shows that the anxiety dimension had a score that limited with the cut-off point of 8 for the anxiety sub-scale, while depression had a low score with respect to the cut-off point of 9 for the depression sub-scale. In relation to the perception of disease (IPQ-B), the highest average scores were in the dimensions of duration, control of treatment and understanding of the disease, while the dimensions of consequences, personal control, identity, worry and emotional response had a mo derate score. As for the QOL-RA of the HRQOL scale, the highest average scores were obtained in the dimensions of support, social life and mood, and average scores in physical ability, pain, stress, health, arthritis, social life, mood and in the QOL-RA full scale.
Pearson correlation analysis
Table 3 presents the results of the Pearson correlation analysis between age, time of diagnosis, (MSM) happiness, anxiety depression (HAD), perception of disease (IPQ-B) with a HRQOL (QOL-RA), where a statistically significant relationship between some variables of the study was found at the 0.01 and 0.05 levels.
Table 3 Pearson correlation analysis between age, diagnosis time, happiness, anxiety, depression, perception of illness and HRQOL
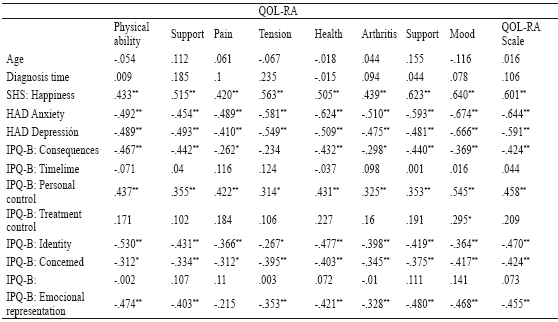
*p < .05, two tails
**p < .01, two tails
With regard to the Happiness Scale (SHS), moderate and high positive correlations with all dimensions of the questionnaire of CVRS QOL-RA were found, such as physical ability, support, pain, stress, health, arthritis, social life and mood, as well as with the full scale. Similarly, the anxiety and depression scale HAD had moderate to high negative correlations with all dimensions of HRQOL.
With respect to the Perception of Disease Questionnaire (IPQ-B), this instrument shows that the dimensions of personal control, identity and concern had low and moderate negative correlations with all dimensions of HRQOL. On the other hand, the dimension of consequences had low and moderate negative correlations with all dimensions of HRQOL except with nervous tension. Similarly, the emotional response dimension had low and moderate negative correlations with all dimensions of HRQOL except with the dimension of pain. Finally, the control of treatment dimension, of the IPQ-B had a low negative correlation with the mood dimension of HRQOL.
Multiple linear regression analysis
According to results found in the final models of Multiple Linear Regression, and considering the CVRS as dependent variable (DV), it was found that the CVRS (QOL-RA) presented a determination coefficient R2c = 49.4 %, explained negatively by the anxiety dimension of the HAD Scale (ß =-0.453; t =-4.241; p = .000), and positively for the Happiness Scale, SHS (ß = 0.364; t = 3.411; p = .001).

DISCUSSION
In this study, the majority of participants were women with an average age of nearly 60 years, a secondary education level, a marital status either married or divorced / separated, who had retired from work, belonging to a medium / low Colombian socioeconomic stratum and who, in average, had a diagnosis of Rheumatoid Arhtritis for 16 years and 6 months.
It is worth mentioning that some of the instruments used in this study have not been validated in the Colombian context. There are only characterizations of the instruments IPQ-B Perception of Illness (Vinaccia Quiceno and Remor, 2012) and the Subjective Happiness Scale - SHS (Quiceno et al., 2012, 2013), whereas on the other hand, there is a Colombian validation ofthe Hospital Anxiety and Depression Scale HADS (Rico et al, 2005) and of the Quality of Life in Rheumatoid Arthritis Scale QOL - RA (Vinaccia, Riveros, Quiceno and Anaya, in evaluation).
Regarding the descriptive results of the study in accordance with the perception of disease (IPQ-B), the patients in this study know that their illness has a long-term prognosis and understand what it means; report symptoms and signs of their condition which limit them in some way in their daily lives; perceive that they have a moderate control of the medical treatment, and refer that they try to manage their disease to the best of their abilities. On the other hand, they perceive that the disease somehow affects their lives, experience some concern about the consequences the disease may cause them at the physical, social, economic and emotional level, and express emotional responses such as anger, annoyance, fear and sadness.
With regard to happiness (SHS), the participants in this study had lower scores (M = 4.06) compared to other researchers developed in Colombia using the same scale with samples of university students (M = 5.0) (Quiceno et al., 2013) and with men deprived of freedom (M = 5.0) (Quiceno et al., 2012). In this regard, in the patients with RA of this study, happiness levels are not so favorable compared to Colombian healthy samples, although different studies affirm that the Colombian population has very high rates of happiness and optimism, regardless of the negative or positive events that happen to them (CENEC, 2001; Cross & Torres, 2006; Sinisterra, 2007).
On the other hand, considering the levels of anxiety and depression (HADS), at a general level there were no symptoms of clinical depression in these patients (Rico et al., 2005), while there were in anxiety, since scores were slightly above the cut-off point for the Colombian sample (M = 8.34). These results differ in relation to the symptoms of depression in patients from the study of Matcham et al, 2014, but are similar to the study of Ryan (2014) in levels of anxiety in patients with RA.
In accordance with the HRQOL (QOL-RA), the patients of this study had higher average scores in the dimensions of support, social life and mood, and average scores in the dimensions of physical ability, pain, nervous tension, health, arthritis, social life and, mood, and in the full scale of QOL-RA. The results of the full scale of the QOL-RA in this study with patients natives of the city of Bogotá (M = 6.62) are slightly similar to those obtained in studies of Vinaccia, Fernandez, Moreno and Padilla (2006) (M = 6.40), and differ a little from the study of Vinaccia, Tobon, Moreno, Cadena and Anaya (2005) (M = 5.28) with samples of AR natives of the "paisa culture" of Medellin. It can be seen that, despite the differences in the stage of the disease and culture in these three studies, the levels of HRQOL are kept almost similar. In other words, the cultural differences in this type of disease are not so marked in Colombian samples, which differs from other studies that have suggested the influence of ethnic and cultural factors in the perception of the quality of life both in the general population as in samples with any chronic disease (Goh, Rusli and Khalid, 2014; Verhagen, Ros, Steunenberg and Witt, 2014).
In terms of correlation analysis, it can be seen that for these patients there were no significant correlations between age and time of diagnosis of the disease with an HRQOL. In terms of the Perception of Disease Scale (IPQ-B), the dimensions of life, control of treatment and understanding of disease had no correlations with the HRQOL. However, the other dimensions as consequences, identity, worry and emotional response were negatively associated with different dimensions and the full scale of HRQOL (QOL-RA), while the personal control dimension had a positive correlation with the HRQOL. In this regard, Quiceno and Vinaccia (2010) found in a review of literature with different physical pathologies that the perception of disease correlated with quality of life, demonstrating that the negative perceptions of the disease have a direct impact on the physical and mental well-being of people with any chronic condition (Fowler and Baas, 2006;) Groarke, Curtis, Coughlan and Gsel, 2004; Paschalides et al., 2004).
Similarly, it has been found that the HADS scale, that measures anxiety and depression, had negative correlations with all dimensions and with the full scale of QOL-RA. Different studies have shown revealed significant levels (21% to 70%) of anxiety in RA (Covic et al., 2012; Isik, Koca, Ozturk and Mermi, 2007) and the influence of this negative emotion on HRQOL (Nas et al., 2011; Ozcetin et al., 2007).
Positive correlations with all dimensions and the full scale of QOL-RA can be seen in relation to the Happiness Scale (SHS). In this regard, the research on happiness as subjective well-being construct has been investigated in health psychology as an important indicator of quality of life in samples of chronic patients in hemodialysis process (Bennet, Weinberg, Bridgman and Cummins, 2015; Musschenga, 1997), in elderly people with different medical diagnoses (Steptoe, Deaton and Stone, 2015) and schizophrenia (Palmer, Martin, Deeep, Glorioso and Cesky, 2014).
On the other hand, multiple linear regression analysis shows that the anxiety dimension of the HADS scale had a negative weight on the quality of life, while the happiness of the SHS had a positive weight on quality of life. Similar results have been found in samples of chronically ill individuals (Hoppe, 2013 ;) NAS et al., 2011; Ozcetin et al., 2007; Veenhoven, 2008) and in patients with chro nic pain (Muller et al., 2015; Tran et al., 2015; Ryan and McGuire, 2015).
Finally, as limitations of the study, there is, first of all, the limited size of the sample (62 people), which was conditioned to the pathological characteristics (diagnosis of rheumatoid arthritis) of the study participants; secondly, the absence of solid epidemiological studies about this disease in Colombia and about the population with rheumatoid arthritis of the city of Bogota; and thirdly, the lack of instruments validated for the population under study.
The results of this research demonstrate the importance of both the salutogenic variables (happiness) and the pathogenic ones (anxiety, depression) on HRQOL of patients with rheumatoid arthritis. The diagnosis of a chronic illness such as RA profoundly affects the lives of people who suffer from them, since their life project has to be reviewed and often they may not know what its course will be, given that the characteristics of evolution are often unpredictable (Vinaccia, Ramirez & Toro, 2001). Several investigations have found in these patients different types of deficits in learned hopelessness (both at a motivational level, for the reduction in daily living activities; and at a cognitive level for the reduction of efforts to develop new adaptation strategies), that affect the emotional area with increased depression and anxiety, and diminished self-esteem (Vinaccia, Cadena, Juárez, Contreras & Anaya, 2004).
Considering that there is vast empirical information on the protector role of positive psychosocial variables and positive emotions for a better psychological and physical well-being in patients with RA (Quiceno and Vinaccia, 2011), it is necessary to develop programs for the promotion of positive emotions, resilience and training of self-control techniques in RA patients (Quiceno, Vinaccia and Remor, 2011; Gráninger, 2015).

