











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Among the most common mental disorders in childhood and adolescence are anxiety disorders, which may result in feelings of excessive worry and fear (World Health Organization, 2021). According to the Institute of Health Metrics and Evaluation (2019), 58 million children and adolescents worldwide suffer from this mental health condition. Anxiety has a significant impact on children, their families, their relationships, and their school life (Mohammad et al., 2020). In Ecuador, the prevalence of anxiety disorder per 100 000 children between the ages of 4 and 18 in both sexes is 2 765 (Institute of Health Metrics and Evaluation, 2019).
Anxiety in childhood is not often detected and treated in time. Therefore, it tends to persist and become chronic (Creswell et al., 2020; Essau et al., 2014; Kara, 2022), being a precursor of other problems in adolescents and adults such as depression (Gundel et al., 2018; Kohn, 2018; Morales-Muñoz et al., 2023; Orgilés et al., 2020). One factor to be considered in the assessment of childhood anxiety disorders is the difficulty that children have in identifying and verbalising their own symptoms (Emslie, 2008). For this reason, it is necessary to obtain information from multiple informants, e.g., from parents, care givers, and teachers (Freidl et al., 2017; Spence, 2018). Based on previous research, it has been suggested that parents can provide valuable information to mental health professionals during the assessment process of young children, which can supplement self-reported measures (Hyland et al., 2022; Reardon et al., 2018; Vidair et al., 2011). Utilising various measures can further assist mental health professionals in obtaining comprehensive information to facilitate diagnosis and treatment planning (et al., 2019b).
To date, very few studies in the literature have validated anxiety assessment tests that include a parent-reported version, such as the SCARED-R (Muris et al., 1999), MASC 2 (March, 2012), or SCAS (Spence, 1997, 1998). In particular, the SCAS is one of the most widely used tools to assess anxiety in the child-adolescent population because it has shown excellent psychometric properties, and its brevity facilitates its administration in different contexts (Orgilés et al., 2022). Furthermore, the SCAS has different versions depending on the age of the children evaluated, such as the preschool version (PAS; Spence et al., 2001), the informant (i.e., self-reported (SCAS-C; Reardon et al., 2019), parent-reported (SCAS-P; Nauta et al., 2004), and teacher-reported (Lyneham et al., 2008)). Short versions of the scale have also been developed (SCAS-S; Ahlen et al., 2018).
The original parent-reported version of the SCAS was composed of 38 items and maintains the same structure as the self-reported version (Nauta et al., 2004). It demonstrated excellent psychometric properties (Nauta et al., 2004), as supported by several studies (e.g., Arendt et al., 2014, Whiteside & Brown, 2008). Currently, the SCAS-P is used in different countries and has been translated and validated in studies with various community populations, (e.g., Arendt et al., 2014, DeSousa et al., 2014, Orgilés et al., 2019, Whiteside & Brown, 2008), where it has been shown to be sensitive in identifying children with high levels of anxiety (Reardon et al., 2018). A brief version of the instrument, the SCAS-P-8, was developed, adapted, and validated for the Spanish population in order to facilitate its application in specific contexts, such as in schools or primary care centres, supporting its usefulness in detecting child anxiety problems (Orgilés et al., 2022).
The SCAS-P has demonstrated good psychometric properties for Spanish parents. However, cultural differences and a lack of locally adapted instruments that measure clinical symptomatology in Latin American populations (Larzabal-Fernández et al., 2023) make it necessary to examine whether its psychometric properties are also good in other Spanish-speaking populations. Thus, to provide an evaluation instrument that facilitates the early detection of anxiety problems in Ecuadorian children, this study aimed to examine the psychometric properties and factorial structure of the SCAS-P-8 in a sample of Ecuadorian children from 8 to 12 years of age. Based on previous studies, we hypothesised that the scale would show good reliability and a unifactorial structure.
Method
Participants
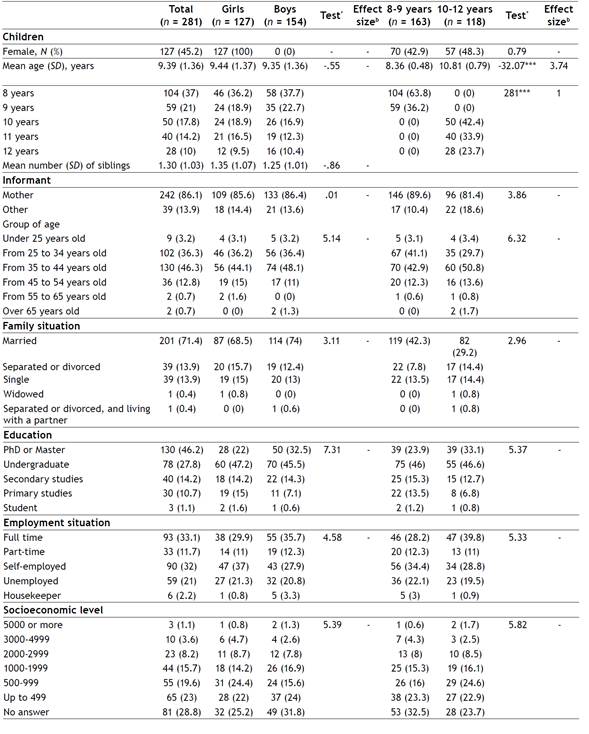
The sample consisted of 281 parents (86.10% mothers) of children from 8 to 12 years of age (M = 9.39; SD = 1.36). Of the children, 127 (45.19%) were girls and 154 (54.80%) were boys. Table 1 presents the sociodemographic information regarding the school year, nationality, number of siblings, family situation, and parental socio-economic and educational level.
Measures
Brief version for parents of the Spence Children’s Anxiety Scale (SCAS-P-8; Orgilés et al., 2022; Reardon et al., 2018). The SCAS-P-8 is an 8-item questionnaire designed to assess symptoms of social anxiety (2 items), separation anxiety (2 items), panic/agoraphobia (1 item), and eneralized anxiety (3 items) based on the current DSM-5 criteria (APA, 2013; Reardon et al., 2018). Responses are rated on a 4-point Likert scale (0-never, 1-sometimes, 2-often, and 3-always), with total scores ranging from 0 to 24, where higher scores indicate higher levels of anxiety. The SCAS-P-8 achieved good psychometric properties, including a reasonable Internal consistency (𝛼 = .82), and an optimal cut-off score for the parent report established at 7.5 (Reardon et al., 2018). The instrument has also demonstrated good psychometric properties in a Spanish-speaking sample (Orgilés et al., 2022), supporting a one-factor structure (Orgilés et al., 2022).
Procedure
The items of the Spanish version of the SCAS were reviewed by a native psychologist affiliated with a university in Ecuador to determine if any adaptations were needed to suit the cultural context. After confirming that no changes were necessary, the scale was piloted with five parents of children aged 8 to 12 to ensure that they understood the scale’s items. Subsequently, an online questionnaire was distributed via social media platforms (Facebook, Twitter, and Instagram). Families were provided with information concerning the study and were invited to participate after providing informed consent. Data was collected from one parent only, and no incentives were offered for participation. The scale took approximately 7 minutes to complete. The study was approved by the Ethics Committee of the Miguel Hernández University of Elche (Ref. ADH.DES.MAIG.MAIG.23).
Statistical analysis
The data was analyzed in several stages, according to the aims of the study. First, we conducted CFA within the framework of R 3.5.2 with Rstudio 1.1.453 (Team, 2018) to test the unifactorial structure of the SCAS-P-8 (Orgilés et al., 2022; Reardon et al., 2018). In line with previous studies, diagonally weighted least squares (DWLS) estimator was used because of its robustness with ordinal data (Forero et al., 2009). Multiple goodness-of-fit indicators were used, including CFI and TLI ≥ .95, RMSEA and SRMR ≤ .08 (Hu & Bentlet, 1999; MacCallum et al., 1996).
Second, the psychometric properties of the Ecuadorian version of the SCAS-P-8 were explored, including mean and standard deviation for each item, corrected item-total correlation, ordinal alpha if the item was removed, and ordinal alpha for the tool. Our decision for calculating ordinal alpha was determined by the fact that this is a more accurate estimator of reliability for ordinal response scales than the popular Cronbach’s alpha (Gadermann et al., 2012). Based on Nunnally (1978), a criterion of 𝛼 ≥ .70 to assess the adequacy of the alpha coefficient for research objectives was established. Composite reliability was assessed, which is not dependent on the number of attributes related to each concept, and an index of 0.70 or above is considered acceptable (Nunnally, 1978). Additionally, we estimated factor convergence using the average variance extracted (AVE) from the items. The higher the value of the AVE, the greater the representativeness of the indicators on the latent variable in which they saturate (Hair et al., 2006).
Third, to test the SCAS-P-8 invariance over children’s sex (“male” and “female”) and age (“from 8 to 9 years old” and “from 10 to 12 years old”), Multiple Group Confirmatory Factor Analysis (MG-CFA) was performed in the framework of R 3.5.2 with Rstudio 1.1.453 (Team, 2018). Following the recommendations registered in the literature (Cheung, & Rensvold, 2002; Kimber et al., 2015; Timmons, 2010), evidence of invariance was provided by comparing less restrictive models (e.g., configural invariance) and more restrictive models (e.g., weak invariance). A value of change in CFI (ΔCFI) and TLI (ΔTLI) smaller or equal to 0.01, and a ΔRMSEA value smaller or equal to 0.015 were indicators of invariance across groups. Lastly, the characteristics of the sample and the differences by age and sex in the SCAS-P-8 were studied using descriptive statistics by way of the SPSS v26 programme.
Results
Structural validity
CFA results indicated that the one-factor model yielded an adequate CFI value; however, the TLI value was slightly lower and the RMSEA and SRMR values were higher than recommended: x2(20) = 102.53, CFI = .96, TLI = .94, RMSEA = .12, 95% CI (.09, .14), SRMR = .09. The factor loadings of all items exceeded .50, ranging from .52 to .79, except for Item 1 whose factor loading was .48.
Based on the study conducted by Orgilés et al. (2022) and modification rates obtained, the items evaluating social anxiety (4 and 7) were correlated. The final fit of the Ecuadorian version of the SCAS-P-8 to a one-factor structure was adequate: x2(20) = 38.80; CFI = .97; TLI = .97; RMSEA: .06, 90% CI (0.03, 0.08); SRMR = .06. All the factor loadings were above .45, ranging from .46 to .68. Factor loadings were as follows: item 1 (.46), item 2 (.68), item 3 (.49), item 4 (.59), item 5 (.56), item 6 (.63), item 7 (.68) and item 8 (.68).
Psychometric properties and reliability evidence
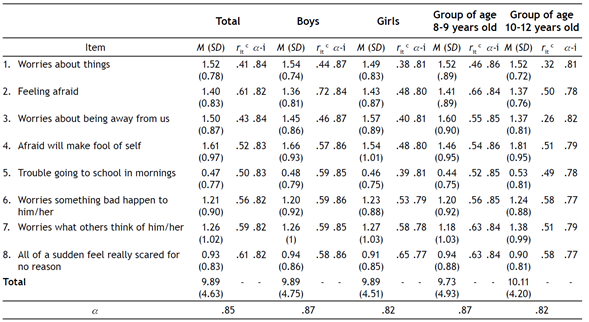
The mean for the SCAS-P-8 was 9.89 (SD = 4.63) and the total ordinal alpha was .85. The reliability of the full scale did not improve in case of deleting items, therefore, all were retained. Corrected item-total correlations for the SCAS-P-8 varied from .41 to .61, indicating an acceptable homogeneity. The composite reliability was 0.81, indicating that approximately 81% of the observed variance in the items is attributable to the common variance among them, while the remaining 19% is due to the unique variance of each item or variable. Therefore, the items or variables are strongly related to each other, and the construct of anxiety is being assessed in a consistent way. The AVE index was 0.40, which is considered moderate and suggests that approximately 40% of the variance in the items is being explained by the underlying construct. While this value does not reach the threshold of 0.50 for optimal convergent validity, it remains reasonably acceptable (Hair et al., 2006). Descriptive statistics of the SCAS-P-8 (including corrected item-test correlations, means, and standard deviations) is shown on Table 2 for the total sample and subsamples, including boys, girls, children aged 8-9 and those aged 10-12 years old.
Sex and age invariance
Sex and age invariance for the SCAS-P-8 was examined for the final model in the Ecuadorian version of this tool (one-factor model, including a correlation between items 4 and 7, which evaluate social anxiety).
Regarding sex invariance, the configural invariance showed an excellent fit to the data (MLR x2 = 16.91; df = 38; CFI = 1; TLI = 1; RMSEA= 0), as shown on Table 3. The first more restrictive model, the weak invariance model, fit the data well. No changes in CFI, TLI and RMSEA between the configural and restrictive models were found, suggesting that the items used to estimate the factor loadings have the same meaning for girls and boys. The strong invariance model was the next restrictive model, and it also fit the data well. Considering ΔCFI, ΔTLI, and ΔRMSEA values, the factor loadings and item intercepts are invariant between sexes. The last level of invariance tested was the strict invariance model. Results suggest that the average item score comparison is valid between boys and girls. Therefore, the Ecuadorian version of the SCAS-P-8 proved to be invariant by sex in this sample. To determine whether children’s age affected that measurement model, the sample was split into two groups: 1. Children aged 8-9 years old and 2. Children aged 10-12 years old. As shown on Table 3, the analyses supported the most restrictive level of invariance (strict invariance model), indicating that the SCAS-P-8 seems to be invariant by groups of age in this study.
Table 3 Gender and age invariance: Summary of goodness-of-fit indices
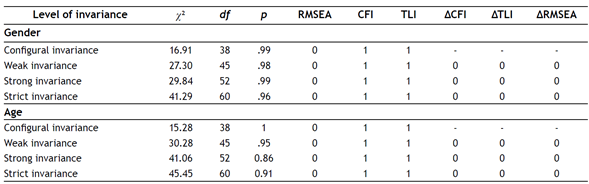
Note. x2 = Santorra-Bentler Scaled Chi-Square; df = Degrees of Freedom; CFI = Comparative Fit Index; TLI = Tucker Lewis Index; RMSEA = Root Mean Square Error of Approximation; ΔCFI = Increase of the CFI value; ΔTLI = Increase of the TLI value; ΔRMSEA = Increase of the RMSEA value.
Gender and age differences
Given the acceptable measurement invariance across sex and age, we compared the latent factor mean across sex and age. No difference in the SCAS-P-8 was observed between girls (M = 9.89; SD = 4.51) and boys (M = 9.89; SD = 4.75), t = -.003, p = .99. No difference in the SCAS-P-8 was observed between children aged 8 to 9 years old (M = 9.73; SD = 4.93) and those aged 10 to 12 years old (M = 10.11; SD = 4.20), t = -.68, p = .49. These results suggest that the level of anxiety is equivalent by sex and age in Ecuadorian children between 8 and 12 years old, according to the assessment of their parents.
Discussion
Accurate assessment of anxiety symptoms in children is crucial for proper diagnosis, treatment planning, and monitoring treatment outcomes (Silverman & Ollendick, 2005). The use of reliable assessment instruments can aid in the early detection of anxiety disorders, which in turn can lead to more effective treatment and better outcomes for children. The current study aimed to assess the psychometric and structural properties of the Ecuadorian version of the SCAS-P-8 and examine its gender and age factorial invariance. Results indicated that the SCAS-P-8 is a psychometrically reliable tool for measuring anxiety among Ecuadorian children from 8 to 12 years of age, based on parental assessments. The findings indicated that the one-factor structure provided a good fit for the data, and that the structure is invariant across gender and age, indicating that it is suitable for both boys and girls of different ages with comparable accuracy.
Results indicated that the one-factor structure provided a good fit for the data, with adequate TLI, RMSEA, and SRMR values. This structure has been previously supported for the SCAS-8, both in the children and parent versions (Reardon et al., 2018; Rodríguez-Menchón et al., 2022). Factor loadings ranged from .46 to .68, with Item 1 (“Worries about things”) and Item 3 (“Worries about being away from us”) showing lower factor loadings and correlations. These results differ from the study of the SCAS-C-8 set forth by Rodríguez-Menchón et al. (2022), which showed lower loadings and correlations in Item 5 (“Trouble going to school in the mornings”) and Item 6 (“Suddenly start to tremble or shake”). The lower loadings and correlations found in the present study may have been explained by the difficulty of operationalising the construct of “worry”. Both items were kept in accord with Rodríguez-Menchón et al. (2022) due to the shortness of the scale and the need for further cross-cultural comparisons.
In terms of psychometric properties and reliability evidence, the mean score for the SCAS-P-8 was 9.89 (SD = 4.63) and the total ordinal alpha was .85. The corrected item-total correlations for the SCAS-P-8 varied from .41 to .61, indicating an acceptable level of homogeneity. No improvement in the reliability of the full scale was observed upon deleting items.
This study aimed to examine differences between girls and boys, and between children aged 8 to 9 years old and those aged 10 to 12 years old, regarding their reported levels of anxiety as assessed by their parents. Surprisingly, our analysis did not reveal any significant differences in anxiety levels between girls and boys, nor did we observe variations in anxiety scores across different age groups. These findings are noteworthy and warrant further explanation. In contrast to previous research conducted in various countries (Arendt et al., 2014; Orgilés et al., 2011; Rodríguez-Menchón et al., 2022), our results differ in terms of gender-related anxiety differences. Notably, other studies have found differences when using the children-reported version of the brief scale but not when using the parent-reported brief scale (Reardon et al., 2018). Several potential explanations for these differences exist. First, it is plausible that certain cultural norms and parenting practices in Ecuador create an environment where anxiety symptoms are perceived and reported similarly in both boys and girls. Furthermore, there have been no prior epidemiological investigations into anxiety symptoms specifically in Ecuadorian children, indicating a need to explore this disparity between genders to clarify the findings. Second, some authors suggest that gender differences in anxiety might be more pronounced in adolescence than in childhood (Arendt et al. 2014), which is supported by findings from a recent study on the SCAS in Mainland China, where differences in mean SCAS scores were much greater between genders in adolescence compared to differences in childhood (Zhao et al., 2012). As the current study’s sample did not include adolescents, this might have influenced the lack of gender differences observed in anxiety levels. Third, it is possible that parents participating in the study might have been more aware of anxiety symptoms in their children, resulting in a sample with a higher proportion of anxious boys compared to the general population. Future epidemiological research including multi-informant assessment to evaluate gender differences in anxiety symptoms is warranted.
Regarding the absence of significant age-related differences in anxiety, our findings contrast with studies reporting age-related variations in anxiety symptom trajectories, with older children typically exhibiting higher levels of anxiety symptoms than younger children (Allan et al., 2014). One possible explanation for these dissimilarities could be related to the relatively narrow age range of our sample (8 to 12 years of age). It is plausible that the developmental changes in anxiety symptoms might be more subtle within this particular age span, and any potential age-related differences could emerge outside the scope of our study. Further investigation with a broader age range might provide a more comprehensive understanding of the developmental patterns of anxiety in Ecuadorian children.
Finally, the SCAS-P-8 one-factor structure was invariant across age and sex, which indicates that the SCAS-P-8 measures anxiety in an equivalent way across different age and gender groups in this sample, and that the differences in the scale scores are meaningful and can be compared.
It is also important to consider the limitations of the present study when interpreting the results. One limitation is the relatively small sample size, which may have affected the reliability of the SCAS-P-8. Another limitation of the study is that validity and test-retest reliability were not examined in this study. Also, while the SCAS-P-8 has been shown to be a reliable measure of anxiety symptoms when completed by parents, it would be interesting to compare the results of parent and child reports to see if there is agreement between informants. This would help to further validate the use of the SCAS-P-8 in measuring anxiety symptoms in children. Another limitation is that this study was conducted only a in community sample, and the generalisation of the results to clinical samples should be made with caution.
Despite these limitations, the results from the present study provide important contributions to the field of anxiety assessment. To the best of our knowledge, this is the first study to examine the psychometric properties of the SCAS-P-8 in an Ecuadorian population. The results suggest that the SCAS-P-8 is a psychometrically reliable tool for measuring anxiety in Ecuadorian children, according to the assessment of their parents. The results of the factorial gender and age invariance analyses conducted in this study indicate that the measurement properties of the Ecuadorian version of the SCAS-C-8 are not influenced by gender or by age group, meaning that the scale is measuring anxiety in the same way for both males and females across different ages.
In summary, the findings of this study indicate that the Ecuadorian version of the SCAS-P-8 is an adequate measure for assessing anxiety symptoms in children from 8 to 12 years of age, as reported by their parents. These results are in line with prior research on anxiety assessment in pediatric populations and represent a significant contribution to the field of anxiety measurement in childhood. Given its brief and accurate nature, the SCAS-P-8 is considered to be a useful tool for use in both research and clinical settings for evaluating anxiety symptoms in children in Ecuador 1.

