text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
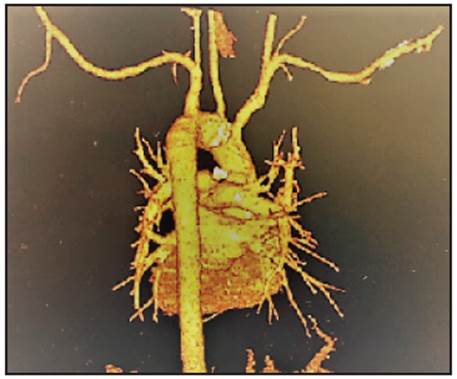
PermalinkA 52-year-old man consulted in the emergency room due to a three-month history of dry cough and oppressive chest pain, associated with dysphonia and dyspnea on exertion. He reported that the symptoms had become more intense over the last week and today he had collapsed. He did not report any history of trauma or personal or family history of coronary disease. His only risk factor was active smoking for the last 10 years. On physical exam, he had a blood pressure of 90/60 mmHg, heart rate of 140 beats per minute and general pallor. No heart or lung abnormalities were found, but he did have generalized lymphadenopathy with a maculopapular rash on the palms of his hands (Figure 1). The electrocardiogram only showed sinus tachycardia. An aortic problem was suspected, and an aortic computed tomography angiography revealed a perforated penetrating ulcer of the aortic arch (Figure 2). Coronary angiography showed no angiographically significant lesions. Human immunodeficiency virus infection was ruled out; however, a serological test for syphilis was positive at a 1:64 dilution. These findings are compatible with the perforation of an atraumatic penetrating ulcer of the transverse aorta due to secondary syphilis.