











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Prevalence of eating disorders has become growing concern among college students in India. Eating disorders are the common psychiatric illnesses with a persistent disturbance in eating patterns or bibr behaviors intended to control weight, body size or shape.1 Eating disorders also affect physical and nutritional health, psychological functioning and if untreated, they can be fatal.2 Earlier studies have shown that eating disorders have the highest mortality rate of any mental illness.3 According to DSM-5, the types of eating disorders are Anorexia Nervosa, Bulimia Nervosa, Binge Eating Disorder, Pica, Rumination Disorder, Avoidant/Restrictive Food Intake Disorder (ARFID), Bibr Specified Feeding or Eating Disorder (OSFED).4
Epidemiological studies have shown that anorexia nervosa (AN) and bulimia nervosa (BN) are more common among females than males.5 Generally, it is believed that body weight and its perception play an important role in the physical and mental well-being of a person.6 Widely published literature indicates gender differences in relation to body weight perception, weight dissatisfaction and disordered eating behaviors.7 Though, both women and men suffer from eating disorders, men with eating disorders have been overlooked, understudied, and underreported.8
Published research report that young academics in the area of health such as nutrition, physical education, nursing and medicine were high risk for Eating Disorders.9 Further, in a survey it was revealed that two-thirds of psychiatrists had seen at least one case of ED, indicating that EDs are not uncommon in urban India.10 In India, research on issues related to EDS mainly focused either among adolescents or female university students are well documented.11 However, there is dearth of literature available among health science students.12 In addition, there are no studies that examined gender differences related to eating behaviors from India. Thus, the present study was aimed to assess gender differences in Body Mass Index, body weight perception, weight satisfaction, disordered eating and weight control strategies among Indian Medical and Nursing Undergraduates
Methods
This study was carried out among medical and nursing undergraduates from renowned colleges from Bangalore, South India between August to October 2014. This was a descriptive cross sectional study conducted among conveniently selected sample. The study criteria include students those were enrolled in to medical and nursing undergraduate courses. Students those were diagnosed to be having psychiatric illnesses and below 18 years were excluded from the study. There were 494 individuals were eligible to participate in to the study. The students who had not volunteered (refused consent) (n=12), absent during data collection period (n=18) and incomplete questionnaires (n=10) were excluded out from the study’s population. Hence, the final sample for the present study comprised of 454 undergraduate medical (n=241) and nursing (n=213) students with high response rate (91.9%).
Definitions
In the present study, eating attitudes include thoughts, beliefs, feelings, behaviors and relationship with food.13 Body weight perception refers to the personal evaluation of one's weight as “underweight” or “normal weight” or “overweight” irrespective of actual body mass index14 Body Mass Index (BMI) in this study was calculated based on self-reported height and weight. The BMI was calculated by dividing body weight in kilograms by the square of height in meters and BMI classification was according to Asian population by the WHO (2004). A BMI ≥ 27.50 indicates a higher risk for obesity, a BMI = 23.00 - 27.50 an increased risk of being overweight, a BMI = 18.50 - 23.00 defines the normal range, and a BMI of less than 18.50 is considered as underweight.
Measures
Socio-Demographic Questionnaire.
This questionnaire collected socio-demographic variables regarding participants’ back ground information i.e. age, gender, education, year of education, religion, background, current weight, height, weight satisfaction( with three responses, ‘satisfied’, ‘not satisfied’, ‘not sure’), and weight perception (with three responses ‘underweight’, ‘normal weight’, ‘over weight’).6
SCOFF questionnaire.
The SCOFF (Sick, Control, One, Fat, Food) questionnaire developed by Morgan et al.15 It is a short and simple screening tool for eating disorders with five items. Every ‘yes’ answer to a question is equivalent to one point. A score of two or more points indicates the patient may be suffering from an eating disorder. This is a highly effective in screening tool for suspicion of eating disorders with good psychometric properties (kappa statistic=0.73 to 0.82).16
Eating Attitudes Test -26.
The Eating Attitude Test-26 (EAT-26) is a self- reported questionnaire widely used to identify the presence of any eating disorder.17 This scale has two sections. Section A consists of 26 items to assess eating attitudes with three subscales namely; Dieting (13 items-1,6,7,10,11,12,14,16,17,22,23,24,26), Bulimia & Food Preoccupation (6 items-3,4,9,18,21,25) and Oral control (7 items-2,5,8,13,15,19,20). Options for the responses are in four-point Likert-scale (3 = always, 2 = usually, 1 = often, 0 =sometimes/rarely/never), where higher scores indicating a higher likelihood of maladaptive eating attitudes and behaviors. The total sum of EAT-26 scores ranges from 0 to78. A score of 20 or above is regarded as at risk of eating disorders and diagnostic follow-ups are required.18Section B consisted of six items to assess various aspects of distorted eating behavior, including bulimic tendencies, body image perception and degree of willful control over eating behavior.
Patient Health Questionnaire.
The PHQ-9 is a self-reported, nine-item questionnaire specific to depression with good psychometric properties.19 This is a four-point Likert-scale (0 =not at all, 1 =several days, 2 =more than half the days, or 3 =nearly every day) with score range 0-27 (0 indicating no depressive symptoms and 27 indicating all symptoms occurring nearly daily). The score <4 indicates minor depression, 5-14 suggests moderate depression and >14 indicates severe depression.
Data collection procedure
After obtaining permission from college administrators, the participants were approached by the primary author after their regular lectures. The students were informed about the aims of the research. After acquiring verbal consent from the participants, English versions of the questionnaires were administered. The students took approximately 15-20 minutes to complete the questionnaires.
Ethical considerations
The study protocol was approved by Institute Ethics committee. Permission was sought from the administrators of the colleges where the study was conducted. The participants were explained that participation in to the study is purely voluntary and their responses would have no influence on their semester exams. Data collection tools contained no identifying information and therefore kept the individual responses confidential.
Data Analysis
The data were analyzed using appropriate statistics and results were presented in narratives and tables. Descriptive (frequency, percentage, mean and standard deviation) and inferential statistics (Chi-square test, t- test) was used to interpret the data. The results considered statistically significance if the p value is less than 0.05.
Results
The present study comprised of 454 individuals of whom majority (n=357, 78.6%) were females. The mean age for the men was 20 yrs (SD=2.04) and for the women was 19 yrs (SD=1.32). Men (M±SD, 23.06±4.34) had a significantly higher BMI than women (M±SD, 23.06±4.34,t=5.403, p<0.001). Table 1 shows that, women in relation to men were younger (71.7% vs. 58.8%), nursing students (58.3% vs. 5.2%), with rural back ground (30.5% vs. 15.5%) and have less Weight status according to BMI of overweight (20.7% vs. 47.4%); these differences were statistically significant. The self-perception of overweight was very similar in both genders (28.9% in men and 23.2% in women) as well as the non-satisfaction with the weight (33% in men and 39.8% in women).
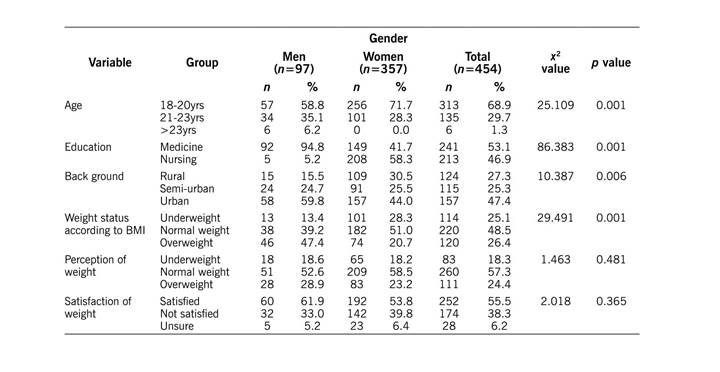
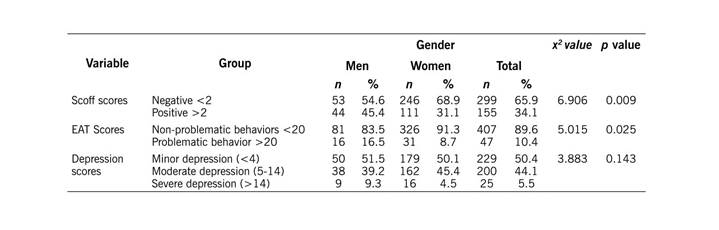
Table 2 shows association between gender and SCOFF, EAT scores. More men than women scored positively for disordered eating behaviors on SCOFF scale (45.4% vs. 31.1%) and for problematic behavior on EAT scale (16.5% vs. 8.7%). Severe depression in men was the double than in women (9.3% vs. 4.5%), but this difference was no significant.
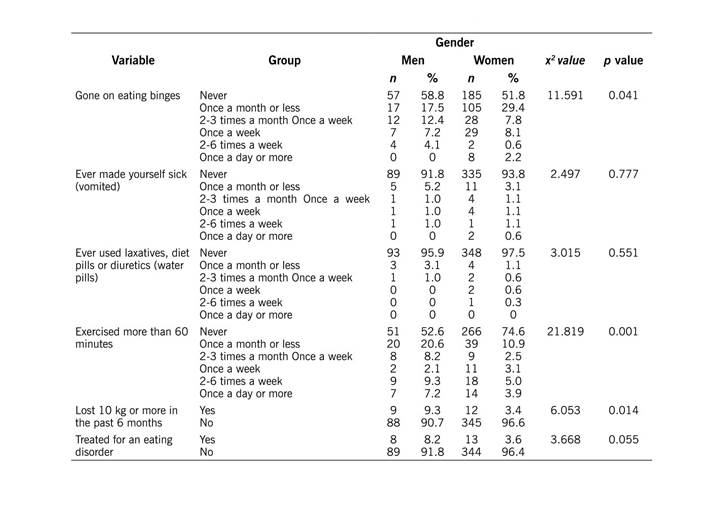
With regard to weight control behaviors, more number of women (48.2%) than men (41.2%) practice binge eating and this difference was statistically significant. Most of the men and women disagreed that they made themselves sick by vomiting (91.8% and 93.8% respectively) and used laxatives, diet pills or diuretics to control their weight (95.9% and 97.5% respectively). However, 47.4% of men compared to 25.4% of women endorsed that they have exercised more than sixty minutes (p<0.001). More men (9.3%) than women (3.4%) lost their weight more than 10 kgs in the past six months and 8.2% of men and 3.6% of women agreed that they were treated for eating disorders. These differences were statistically significant. (Table 3).
Discussion
The present study was aimed to examine the gender differences in magnitude of eating disorders, body dissatisfaction and depression among Indian nursing and medical undergraduates. The findings indicate that more number of women than men were dissatisfied with their body weight, perceived themselves as overweight. But more number of men than women shown to be high risk for development of eating disorders on EAT and SCOFF scales. It is particularly noteworthy that 48.2% of women and 41.2% of men practiced binge eating to control their weight.
In the present study sample, mean BMI was significantly higher in men than in women. This is in consistent with earlier studies.20 In line with previous research,21 more number of women in this study was underweight. However, the number of women those were overweight was higher than men. These findings differ from a study that examined gender differences in body mass index (BMI), body weight perception, eating attitudes and weight loss strategies among undergraduate students in Malaysia.21 Earlier research indicates that female adolescents tend to perceive their body weight inaccurately when compared to BMI.22 Similarly, in our study, approximately equal percentage (13.1%) of men and women perceived themselves as under weight or over weight. While men underestimate their weight, women felt that they were obese. These findings also were supported by a recent study among Korean high school students.23 These findings indicate an urgent concern as these individuals may engage in undue weight loss practices and may put themselves at risk of nutritional deficiencies.24
Body weight dissatisfaction is common in many modern societies and it appears to have grown over time.7 Widely published literature21 indicates that females were more dissatisfied with their body weight than males. In a study among adult Americans found that women were around twice as likely as men to be dissatisfied with their body size.25 Our study findings also were in concordance with these studies as 81.6% of the women were dissatisfied with their weight compared to 18.4% of the men. However, more empirical evidence is needed in this regard to identify the gender differences in relation with body weight satisfaction.
Early published literature26 report females are at high-risk of eating disorders as compared to males. However, our study revealed more men than women scored positively for disordered eating behaviors on SCOFF (45.4% vs. 31.1%) and EAT scale (16.5% vs. 8.7%). These findings were also comparable to a recent study among undergraduate and post graduate students found that men with overweight had greater eating disorder risk (males OR=3.5; females OR=2.0), binge eating (males OR=2.1; females OR=1.9), and use of compensatory behaviors (males OR=1.5; females OR=1.3).27 Surprisingly, in this study 9.3% of men reported severe depression compared to 5.5% in women. However, this difference was no significant. These findings indicate the need of conducting further studies to screen for depression for earlier intervention to prevent disordered eating behaviors in women.
Earlier studies report that females were generally more concerned about body weight, body shape and eating than males. They diet more frequently, had self-induced vomiting, and used laxatives and exercise as their weight-loss strategies21 In line with previous research,28 our findings also observed that nearly half of the women practice binge eating to control their weight. These findings differed from previous studies that showed no gender differences in the prevalence of binge eating.20 On the contrary, nearly half of the men exercised more than sixty minutes and lost weight more than 10kgs in the past six months. Previous studies also found similar findings.29 Furthermore, 8.2% of men stated that they had undergone treatment for eating disorders. These findings could be due to the stigma attached to eating disorders30 or women don’t want to disclose about their experiences about eating disorders.
The limitations of the present study include cross sectional design, convenient sampling and data were collected using self reported questionnaires including BMI was calculated by height and weight measures reported by the participants. Hence, the findings cannot be generalized to all health science students in India. Future studies with random sampling and qualitative designs could be conducted in different regions in India. Despite these limitations, the present study sample was from two universities from South India and larger sample provided interesting findings that could be helpful in planning interventional programs to prevent eating disorders in this population.
Conclusion
The findings indicate that gender differences exist in body weight perception, satisfaction, eating attitudes and weight control behaviors in Medical and nursing undergraduates. Women were more dissatisfied, perceived themselves as overweight and practiced binge eating than men. Though there were small differences between the genders, cannot be ignored as men agreed that they have undergone treatment for eating disorders. Further, more in depth studies are required to explore the reasons for these gender differences and to develop gender based intervention programs to prevent eating disorders in these populations.

