











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkSnakebite envenoming is a public health problem of high impact on a global basis, having its heaviest burden in sub-Saharan Africa, Asia and Latin America 1 and mostly affecting rural impoverished populations in the rural tropics 2. In 2017, the World Health Organization (WHO) included snakebite envenoming as a category A disease in its list of neglected tropical diseases. Moreover, a resolution on snakebite envenomings was adopted by the World Health Assembly in 2018, and the WHO launched its global strategy for prevention and control of this disease in 2019 3. These initiatives aim at reducing the number of deaths and disabilities due to snakebite envenomings by 50% by the year 2030 3. A key issue in the fulfillment of this global strategy is the acquisition of robust epidemiological information on snakebites in countries with high incidence.
It has been estimated that the total annual number of snakebite envenomings in the world ranges from 1.8 to 2.7 million cases, resulting in 81,000 to 138,000 deaths and in more than 400,000 people left with permanent disabilities 1. In the Americas, an overall incidence and mortality rate of 6.2 and 0.04 per 100,000 population per year, respectively, were described, with a case fatality rate of 0.64% 4. Snake species of the families Viperidae and Elapidae are responsible for the most severe cases of envenoming in the world, with fewer cases inflicted by species of the family Lamprophiidae and the non-front fanged co-lubroid families 1. In Colombia, the report of snakebite envenoming as a single entity started in the year 2008. Previous reports in this country indicate incidences of 6 to 8.5 cases per 100,000 population per year, with a case fatality rate ranging from 1 to 3% 5. More recently, and based on various sources of epidemiological information, Chippaux 4 reported for Colombia, in the period 2009 to 2014, incidence and mortality rate of 8.69 and 0.073 per 100,000 population per year, respectively, with a case fatality rate of 0.84%. The Instituto Nacional de Salud (INS) of Colombia reported 4978 cases of snakebites in the year 2017 6. Other epidemiological studies have described a relationship between snakebite incidence and precipitation in almost 50% of the municipalities in this country 7. Previous reports have focused on particular regions in Colombia, such as Antioquia and Chocó 8, Nariño 9, and the Coffee Triangle Region 10.
Colombia has an abundant herpetofauna of venomous snakes, the most important of which are classified in the families Viperidae and Elapidae. The species of maximum medical impact are the viperids Bothrops asper, B. atrox, B. bilineatus and Crotalus durissus5. In addition, other Bothrops species, and species classified in the genera Bothriechis, Bothrocophias, Lachesis, and Porthidium (family Viperidae), and coral snakes of the genus Micrurus (family Elapidae) also cause human envenomings 5.
It is necessary to have national-wide information on the main epidemiological features of snakebites in Colombia in order to have an integrated view of the characteristics of this disease in the country. The present investigation was undertaken to analyze the epidemiology and some clinical features of this neglected tropical disease in Colombia for the period 2008-2016. This information provides a base of knowledge for the design and implementation of public health policies in this country aimed at developing cost-effective interventions to confront this disease.
METHODOLOGY
A transversal, retrospective descriptive study was done. The data bases used were the official data of Public Health Surveillance in the Integral Information System of the Social Protection (SISPRO) and the Surveillance System in Public Health (Sivigila) of Colombia, for the period 2008-2016. For the estimation of indicators based on population, the municipal area projection 1985-2020, from the National Department of Statistics (DANE), was used. Annual snakebite incidences and mortality rates were calculated by using the DANE data on population of each year, and the incidences per department were also estimated. The identification of the types of snakes responsible for the accidents, as well as the types of localities where bites occurred, the type of health affiliation system through which accidents were treated, and the main clinical manifestations of envenomings, were also collected from these data bases. The estimation of descriptive information, the trend curves and the correlation between various parameters were carried out with the program Excel. Parametric (Student's t test, correlation of Pearson, and Chi squared) and non-parametric (Mann-Whitney) tests were used in the analyses depending on the type of variable, case and groups analyzed. Some results were expressed with the 95% confidence intervals (95% CI). Values of p<0.05 were considered significant.
RESULTS
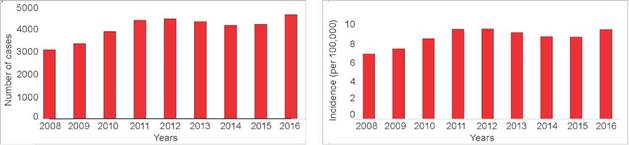
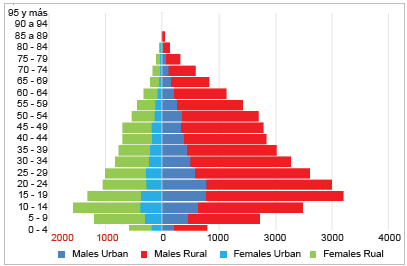
In the interval 2008 to 2016, a total of 37,066 cases of snakebites were reported in Colombia, with a range of 38 to 120 cases per epidemiological week. The total number of cases per year ranged from 3126 (year 2008) to 4704 (year 2016), and the number of fatalities ranged from 28 (year 2008) to 42 (year 2011). In turn, case fatality rates ranged from 0.6% (year 2013) to 1.0% (year 2010) (Table 1). Annual incidences ranged from 7.0 (2008) to 9.7 (2011 and 2012) cases per 100,000 population. Mortality rates ranged from 0.059 (2013) to 0.091 (2011) per 100,000 population (Table 1). There was a trend for increase in the number of bites along this period, with an R2 value of 0.82, with peaks of incidence for the years 2011, 2012 and 2016 (Figure 1).The highest incidences occurred in males, also with an incremental trend (R2 0.7), with male/ female ratios ranging from 2.4 to 2.7 along this period (Figure 2). The mean age of people suffering snakebites in Colombia in this period was 31.7 years (95% CI: 28.3 34.5), with a median age of 28.9 years. The majority of cases (70.3%) correspond to males, and 34.7% of the cases were males younger than 30 years old (Figure 2).
Table 1 Incidence and mortality due to snakebite envenomings in Colombia (2008-2016)
| Year | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 |
|---|---|---|---|---|---|---|---|---|---|
| Cases of snakebites | 3126 | 3405 | 3945 | 4455 | 4526 | 4400 | 4232 | 4273 | 4704 |
| Deaths | 28 | 31 | 38 | 42 | 38 | 28 | 34 | 31 | 34 |
| Incidence per 100,000 population | 7.0 | 7.6 | 8.7 | 9.7 | 9.7 | 9.3 | 8.9 | 8.8 | 9.6 |
| Mortality rate per 100,000 population | 0.063 | 0.069 | 0.083 | 0.091 | 0.082 | 0.059 | 0.071 | 0.064 | 0.070 |
| Case fatality rate (%) | 0.9 | 0.9 | 1.0 | 0.9 | 0.8 | 0.6 | 0.8 | 0.7 | 0.7 |
Source: Data from SISPRO and Sivigila, Colombia, 2008 -2016.
Source: Public Health Surveillance in the Integral Information System of the Social Protection (SISPRO) and the Surveillance System in Public Health (Sivigila) of Colombia.
Figure 1 Number of snakebite cases in Colombia (A) and incidences per year (B) for the period 2008-2016
Source: Public Health Surveillance in the Integral Information System of the Social Protection (SISPRO) and the Surveillance System in Public Health (Sivigila) of Colombia.
Figure 2 Distribution of snakebites occurring in Colombia during the period 2008-2016 according to age, for males and females and for urban and rural locations
The highest number of cases and incidences were in rural regions (Fig 2), with a peak of 31.9 per 100,000 population for the year 2016 and with an incremental trend over the period (R2 = 0.79), whereas the overall incidence in the period for urban areas was 2.8 per 100,000 population per year. Snakebites occurred throughout the country, with the exception of San Andrés, a Caribbean island. The geographical regions of Amazonia and Orinoquia presented the highest incidences, particularly the departments of Amazonas, Vaupés, Guaviare, Vichada and Arauca (Figure 3). Cases occurred throughout the year, without drastic differences in the number of snake-bites along the different months (not shown). When cases were classified according to the self-declared ethnic groups, Afro-Colombian and indigenous people showed the highest percentages among self-declared groups, corresponding to 9.9% and 9.7% of the cases, respectively, whereas most affected people (79.6%) were classified as 'others' in terms of ethnic group, and percentages of less than 1% corresponded to roma, raizel and palenquero groups.
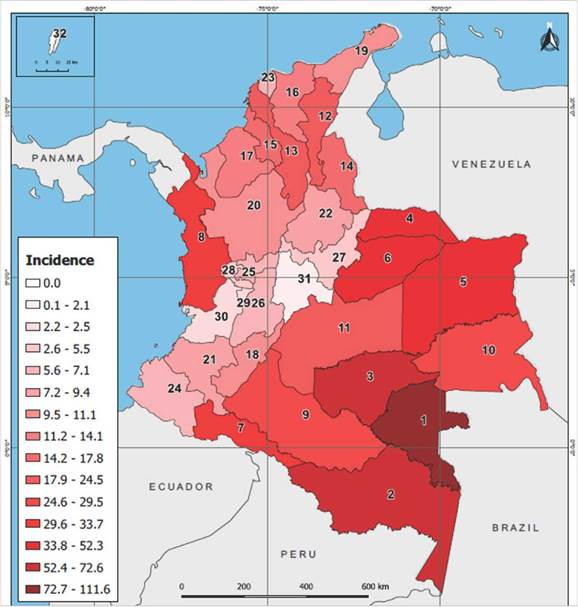
The departments correspond to: (1) Vaupés; (2) Amazonas; (3) Guaviare; (4) Arauca; (5) Vichada; (6) Casanare; (7) Putumayo; (8) Chocó; (9) Caqueta; (10) Guainia; (11) Meta; (12) César; (13) Bolívar; (14) Norte de Santander; (15) Sucre; (16) Magdalena; (17) Córdoba; (18) Huila; (19) La Guajira; (20) Antioquia; (21) Cauca; (22) Santander; (23) Atlántico; (24) Nariño; (25) Caldas; (26) Tolima; (27) Boyacá; (28) Risaralda; (29) Quindío; (30) Valle del Cauca; (31) Cundinamarca; (32) San Andrés. Elaboration of map: Dany Villalobos.
Figure 3 Mean annual incidence of snakebites in Colombia per 100,000 population per departments for the period 2008-2016
In Colombia, health services are provided according to the Social Security General System in Health (Sistema General de Seguridad Social en Salud, SGSSS). People are ascribed to various affiliation systems. Those who pay to receive health services belong to a contributive system, whereas those who are unable to cover the costs of the health service are subsidized by the public health system. In addition, groups classified as 'special' and 'exception' mainly belong to the armed forces and the education sector. According to this classification, the majority of people affected by snakebites in this period belong to the subsidized regime (70.4%), followed by non-insurance (15.5), contributive (11.0%), special (2.2%), exception (0.7%), and undetermined (0.2%).
Regarding the identity of the offending snake, according to the data collected in the information systems analyzed, snakes of the genus Bothrops inflicted 64.5% of the cases (Figure 4). In terms of the activity people were doing at the time of the bite, the majority of the cases occurred while carrying out agricultural work, followed by domestic work (in rural settings), and walking in rural trails (Figure 5). The early management of snakebite cases included, in 30.8 % of the cases, a variety of interventions outside health facilities, such as praying, oral ad-ministration or topic application of plant extracts, suction with the mouth at the site of the bite, and attendance by local healers. In 73.5% of the cases antivenom was administered at health centers.
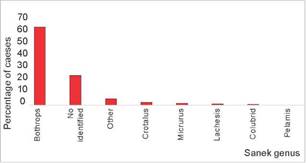
NI: Offending snake was not identified. Others: Snakes of other genera, such as Bothriechis and Porthidium. Source: Public Health Surveillance in the Integral Information System of the Social Protection (SISPRO) and the Surveillance System in Public Health (Sivigila) of Colombia.
Figure 4 Percentage distribution of cases of snakebites in Colombia, on the basis of the genus of the snake causing the accident, for the period 2008-2016
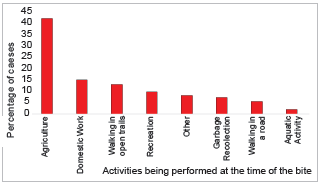
Source: Public Health Surveillance in the Integral Information System of the Social Protection (SISPRO) and the Surveillance System in Public Health (SIVIGILA) of Colombia.
Figure 5 Percentage distribution of cases of snakebites in Colombia, on the basis of the activity being carried out at the time of the bite, for the period 2008-2016
In Colombia, the severity of snakebite envenomings is classified as no envenoming, mild, moderate and severe envenoming, according to the local and systemic clinical manifestations of envenoming and the alterations in clinical laboratory parameters, depending on the genus of the offending snake 11. On this basis, 61.5% of the cases were classified as mild envenomings; among them, 67.6% received antivenom. On the other hand, 32.2 % of cases were classified as moderate, and 6.3% as severe. Of these, 85.3% and 87.7%, respectively, received antivenom as part of the treatment. The local and systemic clinical manifestations of envenomings are depicted in Figures 6 and 7.
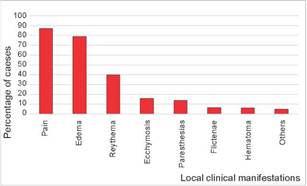
Source: Public Health Surveillance in the Integral Information System of the Social Protection (SISPRO) and the Surveillance System in Public Health (SIVIGILA) of Colombia.
Figure 6 Local clinical manifestations in snakebite envenomings occurring in Colombia in the period 2008-2016
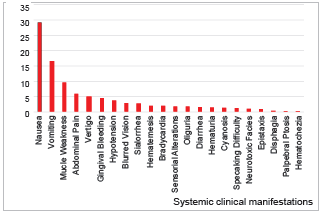
Source: Public Health Surveillance in the Integral Information System of the Social Protection (SISPRO) and the Surveillance System in Public Health (Sivigila) of Colombia.
Figure 7 Systemic clinical manifestations in snakebite envenomings occurring in Colombia in the period 2008-2016
The most common local complications of envenomings were associated with infection (19.5% of cases with cellulitis and 2.9% with abscesses). In terms of systemic com-plications, anemia was described in 1% of cases, and acute kidney injury in 0.8%. Surgical interventions were carried out in 1029 cases, including surgical cleansing procedures (39.75%) and drainage of abscesses (33.72%).
DISCUSSION
This study presents an overview of the main epidemiological features of snakebites in Colombia from 2008 to 2016. The data examined reveal a general trend of an increment in reported snakebites in Colombia over the period 2008-2016. This could reflect an actual increase in the number of bites in the country, but more likely is the consequence of the improvements in the notification of cases. The Instituto Nacional de Salud (INS) and other stakeholders developed a series of workshops in various regions of Colombia from 2015 to 2018, which is likely to have impacted in the report of the cases. Other possible explanations can be considered as well. For instance, changes in the incidence of snakebites may be related to climate parameters, as described in Costa Rica 12, demographic changes, in-country migrations, and changes in the use of the land. In several municipalities in Colombia, a relationship between snakebite incidence and precipitation has been demonstrated 7. It is necessary to carry out more detailed studies to discern which factors are involved behind this increment in the reported number of snakebite cases in Colombia. Despite the described improvement in the collection of data on snakebites, it is likely that under-registration still occurs, especially in regions where snakebites are not attended in health facilities, and this is a limitation of our study. There is a need to identify such regions in order to improve the official records of this neglected tropical disease.
Incidence of snakebites in the period of study in Colombia ranged from 7.0 and 9.3 per 100,000 population per year. These values agree with the value of 8.69 per 100,000 population described by Chippaux 4 for the period 2009-2014. A similar incidence has been described in other countries of Latin America, although some countries in the region show higher incidences, such as Panama, Guyana and French Guyana 4. In terms of mortality rate in the period studied, Colombia had rates that ranged between 0.059 (2013) and 0.091 (2011) deaths per 100,000 population per year. Chippaux 4 described a mean mortality rate for the period 20092014 of 0.073 deaths per 100,000 population per year. Mortality rates in Latin America ranged from 0.012 (Argentina) to 0.631 (French Guyana) per 100,000 population per year 4. When case fatality rates are analyzed, our study showed a range of 0.7% to 1.0%, in agreement with the value of 0.84% described for the period 20092014 4. In Latin America, for this period, case fatality rates ranged from 0.42% (Brazil) to 4.44% (Bolivia) 4. In the Brazilian Amazonia, higher mortality has been described among older people and people from indigenous communities with difficulties for having access to health services and antivenoms 13. It is relevant to investigate whether these factors are also associated with higher mortality in Colombia.
The regions with highest incidences of snakebites in Colombia are the Amazonia and Orinoquia, with highest incidences in the departments of Vaupés, Amazonas, Guaviare, Arauca, Casanare and Vichada. In agreement, the Amazon region in Brazil presents a high incidence of snakebites 14. These departments in Colombia have eco-epidemiological characteristics associated with high incidences of snakebites, i.e. climatic conditions that favor a rich snake fauna, and human activities characterized by agricultural work. A relationship has been found in Colombia between incidence of snakebites and precipitation in about 50% of the municipalities, but not in others 7. Likewise, in the Brazilian Amazonia, snakebites are more frequent in regions of high precipitation and humidity 15. This combination of ecological features and human activities increases the likelihood of encounters be-tween venomous snakes, especially of the genus Bothrops, and humans, as described for the rest of Latin America 16. The identification of the departments and regions of highest incidence of snakebites in Colombia, and the analysis of the access to health posts in these settings (see for example 17, is relevant for the design of public health interventions tailored to the characteristics and needs of those regions, hence making interventions more effective. This has been stressed in the WHO strategy for prevention and control of snakebite envenomings 3.
Snakebites are more frequent in rural areas than in urban settings. The activity associated with the highest number of snakebite cases was agricultural work, as previously described in Colombia 5 and in many regions of the world 1. In this context males are more affected than females, particularly young males in their productive age. Therefore, the study of changes in the use of land in rural areas is relevant for identifying changing patter-ns in snakebite incidence. Examples of such changes are deforestation for expanding agricultural land or creating new urban settings, as well as for development of mining activities. Similar findings of high incidence of snakebites in agricultural settings have been described for Ecuador 18, Costa Rica 19, Bolivia 20, and Brazil 21, among other countries in the region. Despite this trend, it is relevant to identify other circumstances in which snakebites occur. Our work found domestic activities or walking through rural trails as common scenarios of snakebites. Bothrops asper and B. atrox, two species responsible for the highest number of cases in Colombia (5,11,this work), are ecologically-versatile species 22 which can be found nearby human dwellings, hence explaining the occurrence of bites near or inside houses.
There are various ways of affiliation to the Health Social Security System in Colombia. The highest numbers of snakebite cases correspond to people of the low income of the most vulnerable sectors of the population, and these are mostly attended through the subsidized system of public health. It is relevant to identify human groups which are particularly prone to suffer snakebites. Such is the case of indigenous communities in Latin America, which have a high incidence of snakebites and often lack appropriate health services 23,24. The relationship between health issues and ethnicity has been highlighted by the Pan American Health Organization 25. Interventions tailored to the cultural contexts of these groups should be designed and implemented in Colombia and in other countries in the region.
The majority of cases in which the offending snake was identified corresponded to Bothrops sp bites, most likely B. asper or B. atrox. This agrees with the general trend described in Colombia 5. Fewer cases were inflicted by rattlesnakes (Crotalus durissus) and the bushmaster (Lachesis muta and L. acrochorda), and by coral snakes of the genus Micrurus. Envenomings by C. durissus differ from those of other viperids for being predominantly neurotoxic and myotoxic 5. However, it is more difficult to differentiate between cases inflicted by Bothrops sp and Lachesis sp, since they have similar clinical manifestations. Nevertheless, bites by Lachesis are less frequent owing to its pre-dominant distribution in primary forest, whereas B. asper and B. atrox adapt well to agricultural settings and other altered settings 22.
The data collected in the information systems used in this study allow for the analysis of the main clinical features of envenomings. In terms of the severity of the clinical manifestations, cases were classified as mild, moderate or severe in 61.5%, 32.2% and 6.3%, respectively. A more detailed characterization of the severity of the cases has been proposed by Otero-Patiño 11 who graded severity in terms of local and systemic manifestations. According to the clinical manifestations described, the main local effects were pain and edema, in agreement with previous studies describing clinical features in envenomings by Bothrops sp 5,11,19,26,27. In terms of systemic effects, nausea and vomiting were often described, and constitute typical manifestations of viperid envenomings 27. In general, the percentage of patients with systemic manifestations in this study was lower than in previous reports 5,11. This discrepancy reveals limitations in the report of clinical manifestations in the notification systems used in our study and underscores the relevance of using hospital files and prospective clinical studies for detailed analyses of clinical features of envenomings. The most common complications described were associated with local infections, i.e. cellulitis and abscess formation, and necrosis, in agreement with previous works 11,28. Local necrosis of soft tissues may end up in permanent sequelae, with a high impact in the quality of life of people affected 28. A low percentage of cases were associated with respiratory failure, probably caused by bites of coral snakes (Micrurus sp) or rattlesnakes (Crotalus durissus).
In terms of antivenom treatment, among patients who-se envenomings were graded as mild, moderate or severe, the percentages that received antivenom therapy were 68%, 85% and 88%, respectively. The fact that more than 10% of patients having moderate or severe envenomings did not receive antivenom urges attention, as to identify the causes of this observation. Antivenoms from various public and private laboratories are distributed in Colombia, and the recommended dosage varies depending on the neutralizing potency of each antivenom 5. The issue of antivenom availability and accessibility in the various regions of Colombia deserves more detailed investigations.
In conclusion, our study summarizes the main epidemiological features of snakebite envenoming in Colombia for the period 2008-2016. Snakebites constitute the main type of accident caused by venomous animals in this country 29. The information presented in our work allows for the identification of trends in the occurrence of snakebites and for highlighting the regions and human groups at highest risk of suffering snakebites. This, in turn, provides a valuable base of knowledge for the design and implementation of public health interventions, including prevention, early management of cases and appropriate attention in health facilities. More detailed studies are required to further identify regions and groups at high risk, and ways to improve the provision of health services in these and other settings ♣

