











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Glomerulopathy associated with Graves' disease is a rare phenomenon. Its pathogenic mechanisms include damage mediated by antithyroid antibodies (direct or by immune complex deposition), cross antigenic interaction by non-thyroid autoantibodies (e.g., ANCA), damage caused by antithyroid drugs, and radioiodine therapy. Concurrence of other autoimmune diseases with renal involvement is also possible (1). Nephrotic syndrome and membranous glomerulonephritis are usual types of nephritis associated with Graves' disease. Minimal change disease (MCD) is an atypical manifestation of kidney injury in Graves' disease (2, 3). Likewise, propylthiouracil is the thioamide most commonly associated with nephritis, being the association of methimazole as a potential causative agent, much less common (4). In this report, we present the case of a woman with Graves' disease who was undergoing methimazole therapy and developed nephrotic syndrome characterized histologically as MCD.
Case presentation
A 36-year-old woman, from Caracas,Venezuela living in Bogotá, Colombia, visited the Emergency Department due to having experienced, for seven days, facial and lower limb edema associated with foamy urine and decreased urine output. She reported having a history of hyperthyroidism secondary to Graves' disease, diagnosed three months before the consultation. The following findings were reported in her thyroid panel at the time of diagnosis: thyroid stimulating hormone (TSH) <0.005 mU/L (normal range: 0.27-4.2 mU/L); free T4: 5.06 ng/dl (normal range: 0.93-1. 7 ng/dl), total T3: 263 ng/dl (normal range: 80 ng/dl-200 ng/dl); elevated TRAb (Thyrotropin Receptor Antibodies) levels (18 IU/L; normal value <1.75 IU/L); anti-peroxidase antibodies: 10.36 IU/ml (normal range: 0-34 IU/ml), and thyroglobulin thyroid antibodies: 10 IU/ml (normal range: 0-115 IU/ml).
The patient presented with Grave’s ophthalmopathy without activity at the time of the consultation. Also, she reported having experienced a 12 kg weight-loss in the last eight months, as well as an abrupt weight-gain during the last days. The patient denied any exposure to toxic agents and stated she had been using methimazole (50 mg every day, split into three doses), propranolol (40 mg every 12 hours), prednisolone (5 mg every day) for three months as part of the treatment she was prescribed with. Regarding birth control and family planning, she reported the use of oral contraceptives (levonorgestrel 150 𝜇g plus ethinylestradiol 30 𝜇g).
The patient was admitted with a heart rate of 56 beats per minute, a respiratory rate of 18 breaths per minute, blood pressure of 136/85 mmHg, body temperature of 36.8°C and an oxygen saturation value of 95%. She was 1.58 meters tall and weighed 68.2 kg (the usual weight referred by the patient was 58 kg). The following findings were reported on physical examination: exophthalmos, palpebral edema, palpable goiter predominantly in the right lobe, and pitting edema in the ankles. No jugular vein distention, abnormal cardiopulmonary findings or tremors affecting the extremities were evidenced.
On admission tests, creatinine level was 1.9 mg/dl, and urea nitrogen level was 75.9 mg/dl (see Table 1, day zero); besides, a spot sample urinalysis showed substantial proteinuria according to the urine test strip (see Table 2). The protein to creatinine ratio in the admission spot sample was 19398 mg/g and 24-Hour Urine Protein Test of 16.3 g, with a serum albumin level of 2.51 g/dl; hypercholesterolemia and hypertriglyceridemia were documented (see Table 2). Chest radiograph and electrocardiogram were unremarkable. Thyroid function tests on admission showed marked TSH suppression, with low free T4 levels (see Table 1, day 4). Furthermore, a renal ultrasound showed normal echogenicity and size without alterations in the urinary tract (see Table 2). Thus, the patient was diagnosed with a de novo nephrotic syndrome associated with a stage 3 acute kidney injury according to the KDIGO criteria (5).
Table 1 TSH, free T4, serum creatinine, serum urea nitrogen and weight timeline

*Acronyms: BUN (Blood Urea Nitrogen), TSH (Thyroid Stimulating Hormone).
Source: own creation

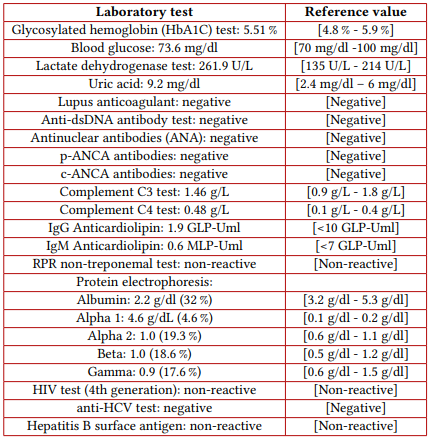
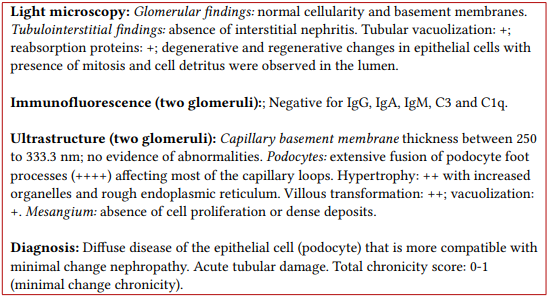
Treatment consisting of furosemide intravenous administration (initially at 10 mg every 4 hours, and then increased to 20 mg every 4 hours), as well as water and sodium intake restriction, was started; atorvastatin administration (20 mg q.d.,) and subcutaneous sodic heparin (5000 UI bid) were also started. Oral contraceptives were withdrawn. Etiological studies were requested and their results allowed ruling out infectious or autoimmune causes (see Table 3). Then, diffuse disease of the epithelial cell (podocytopathy) compatible with minimal change disease (MCD) was identified in an ultrasound-guided percutaneous renal biopsy (see Table 4). Considering the above, methimazole was judged as a potential causal agent and, therefore, its use was suspended; besides, given the impossibility of restarting the administration of antithyroid drugs, total thyroidectomy was proposed as definitive treatment, however, this procedure could not be performed due to renal complications. Weighing the potential response of MCD to systemic corticosteroid therapy, prednisolone oral administration (1 mg/kg daily) was started. Additionally, a Tuberculin Skin Test was negative.
The kidney injury worsened, with a marked increase in serum ureic nitrogen and creatinine levels, and poor response to diuretics due to oliguria (see Table 1, days 7, 8 and 9). Taking this into account, a high risk of uremia and the presence of resistant edema were considered, thus, renal replacement therapy through hemodialysis was started. As it was considered that kidney injury was enhanced by the functional hypothyroidism of the patient, and given the persistence of a marked decrease of free T4 levels, levothyroxine oral supplementation was started with a loading dose of 200 𝜇g and a daily dose of 150 𝜇g, which was later adjusted to 75 𝜇g every day.
Afterwards, the patient experienced a progressive improvement in creatinine and ureic nitrogen levels, as well as a marked weight-loss (see Table 1, days 9 to 15) and normal urine output. Provided that the patient’s kidney function was stable, hemodialysis was stopped six days after it was started. Likewise, due to the stability of both diuresis and kidney function, the normalization of the free T4 levels and the improvement of the edemas, she was discharged and ordered to use prednisolone (45 mg q.d., with a 5 mg reduction every week), levothyroxine 75 𝜇g q.d., and atorvastatin 20 mg every night.
In the outpatient follow-up visits held during the first and second week after she was discharged, the patient reported experiencing insomnia and heart palpitations. Hands tremor was observed on physical examination; a marked increase in free T4 levels (in the range of thyrotoxicosis), as well as adequate kidney function (see Table 1 on days 30 and 36), although with persistent proteinuria and hematuria were evidenced, according to the urine test strip. Levothyroxine was suspended, beta-blocker (propranolol 40 mg q.d.,) administration was restarted and low doses of methimazole (10 mg q.d.,) were restarted, which resulted in the reduction of free T4 levels (see Table 1, day 61) without affecting kidney function. Besides, prednisolone dose was gradually reduced until it was completely suspended.
Finally, after radioiodine therapy was started (two months after the hospital discharge) with a total dose of 30 mCi, the patient showed symptom improvement and a gradual decrease of free T4 levels progressing to secondary hypothyroidism that required levothyroxine supplementation. Kidney function was preserved since hospital discharge (creatinine level between 0.5 mg/dl and 0.61 mg/dl); furthermore, complete remission of the nephrotic syndrome was achieved at day 125 after hospital admission, with normal proteinuria ranges (110 mg in 24 hours) and normalization of serum albumin levels (4.1 g/dl).
Discussion
Graves' disease has been associated with glomerular injury by mechanisms that are not entirely clear, including deposition of immune complexes, cross-reactivity of antithyroid antibodies against renal antigens, and/or the presence of other antibodies with renal effect. Cellular immunity could also have an important role in the pathogenesis, specially by Autoreactive T lymphocytes. In some cases of Grave’s disease, antithyroid drugs or radioiodine therapy have been proposed as the cause of glomerular injury (1,6).
A frequent histopathologic type of glomerulopathy associated with Graves' disease is membranous glomerulonephritis, (7,8) which can lead to the occurrence of nephrotic syndrome, as it has been described in several case reports. However, there are several reports of nephropathy cases in patients with Graves' disease due to MCD in both adults (6,9,10,11,12) and children (13). Among these case reports, there is one of a patient who experienced a nephropathy associated with chronic use of low-dose methimazole, (6) a case of MCD that preceded the clinical manifestations of Graves' disease for several years (11), a case of MCD in a patient who was being treated with propylthiouracil (12), and, one case in which the simultaneous onset of MCD and Graves' disease was reported (10). Other types of kidney injury associated with Graves' disease described in the literature include membranoproliferative glomerulonephritis (14), as reported in a case where it was mediated by immune complexes (15).
Methimazole is a thioamide that inhibits thyroid hormone synthesis. Cases of kidney injury secondary to its use have been documented in the literature, being nephritis a rare adverse effect (16). Some case reports, have proposed methimazole as a causative agent of nephrotic syndrome (17,18,19), taking into account the close temporal association between the onset of renal disease and the time its administration was started, as well as the occurrence of clinical improvement after suspending its use. In at least two cases, an association between methimazole and MCD has been found (6,9). Other types of clinical presentation of kidney injury associated with methimazole use, include hematuria/proteinuria (20) and isolated acute kidney injury (21). Histopathologically, methimazole use has also been associated with the presence of crescentic glomerulonephritis and membranous glomerulopathy (20). The induction of glomerulopathy associated with ANCA (Anti-Neutrophil Cytoplasmic Antibody), especially by anti-myeloperoxidase antibodies (MPO-ANCA)(22), has been proposed as one of the possible pathogenic mechanisms of kidney injury due to methimazole use (23). Furthermore, there is a case of a patient who developed lupus nephritis due to systemic lupus erythematosus presumably induced by methimazole use (24). The exact mechanism that mediates the injury of methimazole in MCD are unknown; one possibility is a direct damage in the podocyte and in the base membrane (21).
In the case reported here, causality assessment systems for adverse drug reactions were used for methimazole. In this regard, a score of 4 points, according to the probability scale by Naranjo (25) was obtained, which makes the adverse reaction to methimazole in our patient "possible", and where aspects such as previous reports of this effect, the use of methimazole preceding the occurrence of the adverse event, and the fact that glomerular injury improved after suspending its administration increased the probability of adverse drug reaction, and, aspects such as the presence of another possible cause of the adverse event (Graves' disease, through other mechanisms) reduced it. Likewise, when the WHO-UMC causality assessment system was used, (26) a “possible” adverse reaction to methimazole was concluded, considering a reasonable temporal relation, although with another potential causal explanation. In our patient, methimazole was reintroduced at low doses and concomitant whit prednisolone without new episodes of proteinuria; this reduced the probability of causal association.
In the case described here, treatment consisted of suspending methimazole use and starting the administration of prednisolone at 1 mg/kg. The use of corticosteroids was based on the extrapolation of the substantial response to this treatment described in pediatric population with MCD, the recommendation made by scientific associations such as the KDIGO initiative (5) and, the biological plausibility of corticosteroids by inhibiting processes mediated by T and B lymphocytes, which have been proposed as mediating mechanisms of MCD (27). Moreover, some case reports of MCD associated with Graves' disease have reported that remission was achieved by using systemic corticosteroid therapy (11,12).
In this case, the patient developed a severe stage 3 acute kidney injury, according to the Kidney Disease: Improving Global Outcomes (KDIGO) initiative classification (5), and needed provisional renal replacement therapy due to oliguria, hypervolemia and azotemia with poor response to diuretics. Acute kidney injury is not unusual in adults with minimal change disease who develop nephrotic syndrome (28). Likewise, renal effects of thyrotoxicosis include increased glomerular filtration rates, and treatment of hyperthyroidism leads to a considerable decrease of said rate (29,30,31). In the present case, the substantial decrease of free T4 levels (in the range of evident hypothyroidism) could have contributed to the marked impairment of renal clearance function. This, added to the renal vasoconstriction effect of the de novo nephrotic syndrome (28). All of these factors, could have contributed to glomerular function deterioration; there was no evidence to consider the presence of rhabdomyolysis triggered by the patient’s iatrogenic hypothyroidism.
Based on the above, it is not possible to say, with a high degree of certainty, that MCD in our patient was caused by either Graves' disease (through different mechanisms) or methimazole use, as they are both potential causes of it and shared causality is even feasible. Similarly, it is possible that another unknown causal element was the cause of MCD in our case. Currently, the way how MCD is caused by Grave’s disease is unknown, as there is not information about the pathogenic mechanisms involved, and the epidemiology and natural course of MCD secondary to Grave’s disease. Besides, there are no diagnostic criteria that allow differentiating between Grave’s disease and its pharmacological management as the cause of MCD.
Conclusions
Graves' disease and its pathogenic processes, as well as its treatment with methimazole, are potential causes of kidney injury in a wide syndromic range, with nephrotic syndrome being a well-known type with multiple histopathological forms, including MCD. Thus, renal biopsy is fundamental in the diagnostic and therapeutic approach in such clinical setting. Severe acute kidney injury is a complication to be considered in patients with nephrotic syndrome due to MCD; likewise, the transition from thyrotoxicosis to induced hypothyroidism may enhance renal function decline. Finally, systemic corticosteroid therapy may have a favorable role in the treatment of MCD associated with Graves' disease.

