











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The mother-child bond is of fundamental importance compared with other bonds that humans develop during life.1 It is a single and long emotional relationship that begins early, during gestation, and is established slowly and gradually in a mutual adaptation process between mother and baby. 2,3) The bond is understood as the ability of the mother to provide love, caring, and enough protection to fulfill the physical and emotional needs of the child. The formation of this bond is influenced not only by maternal behavior but also by the child’s behavior. 1,4) Human infants, unlike those from other species, cannot survive without the care from and bond with parents and caregivers; their interactions determine the quality of care that is offered after the delivery of the baby. Time immediately after delivery is considered critical for establishing the bond because the relationship is facilitated by adequate maternal hormonal system and is stimulated by presence of the baby.1
First cares gives to the baby, the manner in which the mother holds and handles the baby and the way she establishes the routines, timing, and presentation of the world are characteristic factors of the first bonding relationship in humans, influence definitive psychic functioning, help form the basis of the baby's personality, and helps determine how future affective bonds will be established. 5) Therefore, quality of the bond between mother and child will determine the child's future mental health conditions; that is, it is the basis for the creation of their first emotional bonds that would interfere in subsequent social relantionships. 6,7) Care delivery during gestation, labor and puerperium, mainly given by the nurse, must favor the creation of the mother-child bond by identification of factors that might interfere in this process. However, currently, there are several obstacles, mainly for centralized care in biomedical model, necessitating guidance for care practice that seeks life maintenance and quality of life; these depend on a significant and strong relationship with the family, both for the child and the mother.8,9
This study aimed to characterize the demographic profile of puerperae and variables regarding delivery and to analyze the degree of the bond between puerpera and child, both in isolation and associated with experiences during and after delivery. This study was based on the importance of recognizing that the quality of the maternal bond will determine the success of the mother-child relationship and constitutes the basis for the child's mental health.
Methods
This cross-sectional study was performed in a teaching hospital in the city of São José do Rio Preto - SP, Brazil, an institution that represent the main filed of practical teaching of gynecology, obstetrics and pediatrics at Public State Faculty of Medicine and Nursing. The institution provides care for more than 2 million inhabitants from the 102 municipalities that are part of the 15 Regional Divisions of Health in the city of São José do Rio Preto. This large hospital in the São Paulo countryside currently has 180 beds; of these, 46 beds are designated for maternity. During the study, the hospital had 205 beds, 34 of which were maternity.
Data were collected in February 2014 among puerpera by using interviews with two instruments, one of which was structured, concerning the sociodemographic profile with some variables on delivery and significant experiences during and after delivery. We used the Mother-to-Infant Bonding Scale (MIBS), an instrument validated in 2005, which specifically evaluates the mental investment that the baby has in the parents' representative universe.10 This scale comprises 12 items of self-report, supported by three subscales: 1) positive bonding, evaluated by three items (affective, protective, and happy); negative bonding, evaluated by six items (angry, aggressive, sad, resentful, disappointed, uninterested); and unclear bonding, which highlights the presence of emotions not clearly related to bonding (afraid, possessive, neutral or without feeling). Each item has answer categories and one Likert-type scale ranging from 0 to 3: a score of 0 indicates the emotion is not present (elsewhere), and increasing scores indicate increasingly positive responses, up to it’s the maximal level of 3 (very). The responses reflect the feelings of parents in relation to child at the specific time in which the instrument is completed. The higher the score, the greater the degree of bonding seen.3,10 Initially, results of MIBS were analyzed in isolation, and posteriorly they were associated with some significant experiences that interfere in the development of the bond between mothers with their babies. We chose three significant experiences that have been extensively studied and that could interfere in the maternal bond: type of delivery, pain during delivery, and skin-to-skin contact.3,10
To select the sample, we included puerpera who had delivered at Hospital da Criança and Maternidade de São José do Rio Preto - SP in February 2014 and who were at the first and tenth day after labor, were literate, did not have physical or cognitive limitations that would prevent them from completing the instrument, and agreed to participate in the study after signing the consent form. Therefore, sample calculation led to consideration of the mean number of monthly deliveries; the sample consisted of 200 puerperae. We excluded illiterate puerperae who had any medical reason that made it impossible for them to write, as well as those who did not agree to participate after they were adequately informed about the objective of the study.
For data analysis we used descriptive statistical techniques. For the association between significant experiences and items from MIBS, we used Mann-Whitney non-parametric tests to compare two sample groups, and Kruskal-Wallis to compare more than two sample groups; the significance level was 5%. The study followed guidelines of resolution 466/2 of the National Health Council. The study was approved by ethical and research committee with humans of the Faculdade de Medicina de São José do Rio Preto (n.168.636/2012).
Results
The mean age of puerpera included in the study was 26.4 years (standard deviation, 6.9 years; median, 26 years). We observed the presence of a discrepant age value (outlier) - 46 years- that influenced the mean of the age distribution. The minimum age was 14 years, and the maximum age was 46 years. Data on patient age did not follow normal distribution. Most interviewed puerperae declared themselves as white (60.0%), as married (87.5%), and as having completed high school (51.5%). Most women had cesarean deliveries (80.0%), and 68.0% of women did not have pain during labor; only 54.0% had a chance for skin-to-skin contact with the baby immediately after delivery.

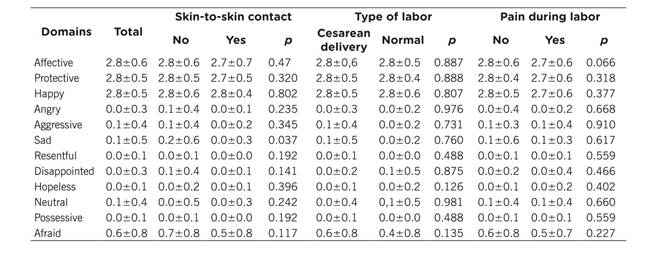
Table 2 shows the following scores on MIBS: total, type of delivery, occurrence of skin-to-skin contact just after delivery, and pain during labor. When evaluated in isolation, the MIBS was score was elevated for positive bonding and low for negative bonding and neutral bonding, which shows that puerperal respondents are highly involved with their children. Responses to the MIBS component on current labor showed that the type of delivery did not affect the bonding degree. Pain during labor did not significantly influence domains on child and mother bonding. All p values were higher than the level of significant applied.
Results showed the influence of skin-to-skin contact (mother-baby) in the domain related to sadness (p=0.037): Puerperal who did not have contact with their newborns showed significantly more sadness than puerperae who had such contact with their child. Variables such as type of labor and pain during labor, when compared with results of the bonding subscale, were not statistically significant (p>0.05).
Discussion
In this study, the participants’ mean age was 26.6 years, which is proportional to the reproductive age of Brazilian woman. This represents a young population because around 50% of them are younger than 30 years. In 2006, a national demographic study on the health of children and women was carried out; the following sociodemographic data were found in relation to race/ethnicity: 35.8% of Brazilian women living in the southeast region of Brazil declared themselves as white, while in other regions, especially the south region, there was a predominance of women who declared themselves to be black (65.7%). Therefore, these data show the divergence of findings in the study that showed a predominance of white women. When formal education level was evaluated, 50% of Brazilian women had completed more than 8 years of education, indicating that they had complete elementary school.11 In our study, 64.3% of women living in São José do Rio Preto concluded the second cycle of elementary education or more years of study. An adequate formal education level in a population is an essential requirement for development of a country to assure the exercise of citizenship and promote equality of social opportunities-among these opportunities, the right to healthcare.12
The marital status of participants in our study corroborate findings from a study in Portugal that also showed a higher percentage of married women (68.3% to 72.2%).10,13 The Winnicott study shows the importance of family support for puerperae who are vulnerable mainly within the first weeks after delivery. 5) Of deliveries in Brazil, 48.3% were cesarean according to the census of 2006, and the southeast region had a higher number of cesarean deliveries (51.7%). 11) In the city of São José do Rio Preto, the number of cesarean deliveries is even greater (86.4%).14 In studies done in the city of São José do Rio Preto, we observed a high incidence of unnecessary cesarean deliveries and a number of women reported cesarean delivery as a commodity.15 In this study, unlike what the researchers expected, the type of current labor did not significantly influence any MIBS domain; however, these findings corroborate other studies that showed no changes in emotional involvement of mothers with their newborns after different types of delivery.16
Studies show that pain in labor is considered a main builder of social representativeness of female attitudes about parturition, and it contributed to high index of cesarean deliveries in the country. 17) In this study, pain during delivery did not significantly influence the mother-and-child bond; however, studies have shown that if labor is difficult and involves more pain, the mother-child relationship will change significantly. 18) Promotion of skin-to-skin contact is an indicator of quality in humanized delivery care.19 According to ordinance no. 371 May 7, 2014, the Brazilian Ministry of Health instituted new guidelines for integral and humanized care to newborn, establishing that skin-to-skin contact must be assured immediately after labor in a continuous way; neonates are to be placed over the abdomen or thorax of the puerpera and are to be covered with a dry and warm cover in order to assure temperature maintenance.20
A study in Paraná showed that only 5.3% of babies born from vaginal deliveries and 1.8% babies born from cesarean deliveries remained with the mother for at least 30 minutes; not allowing the mother and infant to have this sustained contact after delivery can harm both the maternal bond and the promotion of maternal breastfeeding. 21) In Bahia, a study carried out in a public maternity unit showed that nursing professionals involved in promotion of skin-to-skin contact failed to encourage skin-to-skin contact between mothers and neonates. They did not worry about measures that could support mothers and would facilitate this first contact effectively; in addition, they did not inform women about the importance of this contact and not request consent for it. In general, the contact established is brief, and puerperae continue with doubts and anxieties because a short period does not enable adequate recognition between mother and child.20 Another study done in Santa Catarina aimed to identify and analyze feelings expressed by mothers in the first contact with their child. It revealed that first moments after birth constitute a sensitive phase, and it constituted a precious opportunity for mothers to be touched by their babies.22 In skin-to-skin contact there is huge change between mother and child, and it gives the opportunity to begin bonding. Some puerperae are apprehensive about the characteristics of neonates soon after birth. However, having a team available to clarify any apprehension can transform the motivation factors of bonding.23
In our study, we observed that lack of early skin-to-skin contact with the baby negatively influenced bonding: Puerperae who did not establish contact with the neonate were significantly sadder than puerperae who did have early skin-to-skin contact. Although the literature is clear regarding evidence on the importance of skin-to-skin contact, we observed that for more varied reasons the health team can still delay or limit this experience.22,24,25 Data obtained in this study, on a topic so little explored in our area, reveal the variability in the process by which puerperae bond to their babies.
Further studies are needed to clearly establish other significant experiences to before, during and after labor in order to improve the health team's understanding of how to act in this scenario. In addition, it is necessary to understand the need to respect pathways that lead a mother to establish a bond with her child. Some women might have difficulty establishing a emotional bond with newborn. The tasks for health professionals are to identify and act in such situations in order to offer help women establish a solid basis for interaction with and adequate care for their child, thereby facilitating interactions that strengthen the bond.
Limitations of this study include the extensive time needed to conduct the interview. In addition, some puerperae declined to answer the questions, which contributed to an oscillation in the number of responses. Moreover, some data were not evaluated because they were irrelevant; there was great turnover of puerperae because of the many deliveries done and small number of beds in the maternity; and it was difficult to interview puerperae who had health insurance.
Conclusion
Pueperae participants had a high degree of bonding with their babies that is mainly related to history of skin-to-skin contact. Nurses must promote strategies that encourage skin-to-skin contact between mother and newborn in the delivery room. Administration of MIBS by nurses immediately after labor is essential to identify and prevent future fragility in the formation of bonding between mothers and babies and may enable the implementation of new strategies to strengthen this bonding. In addition, seeking direct and humanized care for puerperae will support them in providing adequate care to their child.

