










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.27 no.2 Bogotá Apr./June 2012
Histological characteristics of chronic gastritis reported in gastric biopsies from children aged 1 to 16 years at the Hospital Infantil de San Josè from september 2008 to september 2010
Pilar Archila, MD (1), Leonardo Tovar, MD (2), Mónica Ruiz, MD (3)
(1) Oncological Pathologist at the Hospital de San José and at the Hospital Infantil de San José.
(2) Third year medical resident in Pathology at the Fundación Universitaria de Ciencias de la Salud, Bogotá, D.C., Colombia.
(3) Third year medical resident in Pathology at the Fundación Universitaria de Ciencias de la Salud, Bogotá, D.C., Colombia.
Received: 05-12-11 Accepted: 15-05-12
Abstract
Gastritis is an inflammation of the lining of the gastric mucosa which occurs in response to an injury. It can be acute, chronic or mixed, and it can be associated with intestinal metaplasia and atrophy. There are multiple etiologic factors including irritation, chemical, immunological, genetic and infectious factors. Among the latter, Helicobacter pylori is the most common causative agent.
Objective: The objective of this study was to characterize histologic findings of chronic gastritis in children aged 1-16 years at the Hospital Infantil de San José from September 2008 to September 2010.
Materials and methods: This was an observational and descriptive cross sectional study. Information was obtained from gastric biopsy reports from children between 1 and 16 years of age who had been evaluated at the Hospital Infantil de San José from September 2008 to September 2010.
Results: We reviewed 826 reports of gastric biopsies from children with chronic gastritis. 59.2% of the sample was female, and the mean age was 9 years. Helicobacter pylori was present in 58.96% of this population, gastric atrophy was present in 0.7% and intestinal metaplasia in 1%. It was found that the presence of Helicobacter pylori was related to the degree of chronic inflammation and polymorphonuclear neutrophil activity levels.
Conclusions: Helicobacter pylori infection is common in chronic gastritis in children and its presence is related to the degree of chronic inflammation and polymorphonuclear neutrophil activity.
Key words
Gastritis, Helicobacter Pylori, infant, Sydney System. (Sources: DeCS and MeSH).
INTRODUCTION
Gastritis is an inflammation of the lining of the gastric mucosa in response to an injury. It may be acute with neutrophil infiltration or chronic with lymphocyte or plasma cell infiltration, or both. Many underlying causes are possible including intestinal metaplasia and atrophy (1).
Multiple etiological factors and can be grouped into chemical, immunological, genetic and infectious irritants. Among the latter is the gram negative bacillus Helicobacter pylori which was first observed in the human stomach in 1983 by Warren and Marshall (2-4). Since then it has become recognized as the most common causal agent of gastritis, especially of antral gastritis. It is also the most common cause of gastric and duodenal ulcers (3-5). In addition, it is an essential factor in the pathogenesis of lymphoid tissue tumors associated with the mucosa (MALT lymphomas) and gastric adenocarcinoma. (6-8) Transmission of these bacteria occurs through the oral-oral and fecal-oral route. It has been proposed that half the population is affected by this infection at some point in their lives. Its highest incidence is in the Third world (9, 10).
The prevalence of Helicobacter pylori infections among children has been observed to be between 60% and 90% and is closely related to socioeconomic status and health measures (11-13).
The gold standard for diagnosing gastritis is histopathological testing. Numerous classifications have been developed evolved over time as knowledge of the natural history of disease has advanced. For this study we have used the Sydney Classification System which was originally published in 1990. The Sydney System combines topographical, morphological and etiological diagnoses into a clinically useful diagnosis. Four years after its introduction the Sydney System was updated by an international group of pathologists who established the consensual terminology for gastritis, improved guidelines for histological classification and rationalized the diagnostic process (1, 14).
Since studies of chronic gastritis among children in Colombia are scarce, and since of Helicobacter pylori's incidence is high throughout the world, and since it is related to chronic inflammatory processes associated with subsequent increased incidence of neoplasms, we were motivated to carry out this study and contribute to the understanding of chronic gastritis in children caused by Helicobacter pylori. Equally important for us is learning about the pathology from the epidemiological point of view. This study of these bacteria among pediatric patients studied at the Hospital Infantil de San José also internally validated our procedures and allowed us to compare our results with national and international studies.
MATERIALS AND METHODS
An observational descriptive cross sectional study was performed using all the reports from gastric biopsies taken from children between 1-16 years old which had been evaluated at the Hospital Infantil de San José between September 2008 and September 2010. The Sydney System was used for these evaluations (14). No cardial biopsies or cases reported as chemical gastritis or gastric biopsies reported as normal were included.
The Sydney system was established to measure degrees of chronic gastritis considering topographic, morphological and etiological information. It uses a visual analogue system which is clearly explained in the consensus. To assess the density of Helicobacter pylori it uses polymorphonuclear neutrophil activity, chronic inflammation, glandular atrophy and intestinal metaplasia (14).
The protocols of gastric biopsies were checked in order to clarify certain variables such as age, gender and the criteria included in the Sydney system.
For data analysis we used descriptive statistical techniques and non-parametric inferential statistics such as the chi-square test and the Spearman Rank Correlation method. These statistical procedures were based on Stata version 10.0 for Windows.
The protocol had the approval of the Research and Ethics Committee of the Faculty of Medicine of the University Foundation of Health Sciences and the research was classified as without risk.
RESULTS
During the period of the study we found a total of 849 gastric biopsy reports. 23 did not meet the inclusion criteria because 17 reported chemical gastritis, and 6 reported normal mucosa. The final sample thus was constituted of 826 reports.
59.2% of the population consisted of girls. The average age was 9.4 years old. 90.6% of the gastric biopsies studied were taken from the antral region.
According to the Sydney system criteria assessed in gastric biopsies the following results were found (Table 1).
Table 1. Population Characteristics (n=826)
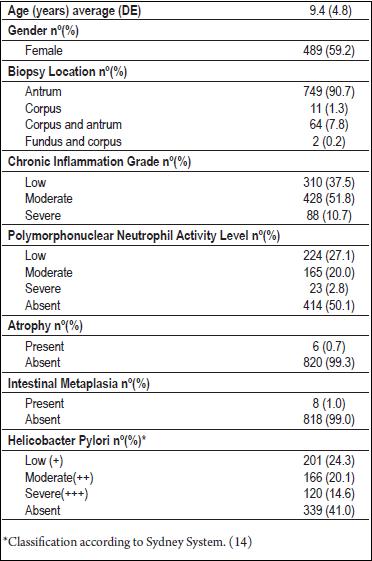
Polymorphonuclear neutrophil activity grade
27.1% of the biopsies examined had low polymorphonuclear neutrophil activity, 20% had moderate and 2.8% had severe activity (Figure 1).
Figure 1. Inflammatory polymorphonuclear neutrophil infiltrate in a gastric gland with epithelial permeation (Hematoxylin and Eosin stain; original magnification x 40).

Chronic inflammation grade
37.5% of biopsies evaluated showed low degrees of chronic inflammation, 51.8% had moderate degrees, and 10.7% had severe degrees (Figure 2).
Figure 2. Severe chronic inflammatory infiltrate consisting of lymphocytes (Hematoxylin and Eosin stain; original magnification x 20).

Atrophy and intestinal metaplasia
Gastric atrophy was found in 0.7% of the population and intestinal metaplasia was found in 1% (Figure 3).
Figure 3. Complete intestinal metaplasia (Hematoxylin and Eosin stain; original magnification x 20).

Helicobacter Pylori
H. pylori infections were found in 59% of the population. 24.3% had small numbers of bacteria, 20.1% had moderate numbers, and 14.6% had abundant bacterial populations (Figure 4).
Figure 4. Helicobacter Pylori in abundant quantities +++/+++ (Hematoxylin and Eosin stain; original magnification x 100).

Chi-squared tests showed the existence of a relation (p <0.0001) between Helicobacter pylori infections and the grade of chronic inflammation. It is important to note that of the 88 cases of severe chronic inflammation found in biopsies, only 3 did not present Helicobacter pylori (Table 2 and Figure 5).
Table 2. Relation between presence of Helicobacter Pylori and Chronic Inflammation Grade.
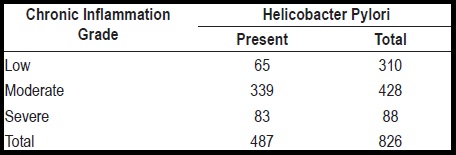
Figure 5. Relation between the presence of Helicobacter pylori and the grade of chronic gastritis.

In addition, we found that Helicobacter pylori infection is related to the grade of polymorphonuclear neutrophil activity (p <0.0001) (Table 3).
Table 3. Relation between presence of Helicobacter Pylori and grade of polymorphonuclear neutrophil activity

DISCUSSION
The frequency of Helicobacter pylori infections in our hospital was similar to those found by other authors in Latin America and Asia. In a study conducted in Cuba, Gamez Escalona used a histological method and found a frequency of Helicobacter pylori infection of 67.7% in the pediatric population evaluated (15). Sarmiento Q, in a study of a pediatric population in Chile, found a 69% infection rate in the study population using histopathological studies for diagnosis (16). A study in Brazil which used a urease test found a 56% prevalence of Helicobacter pylori in a pediatric population while another study among children Bangladesh using the same diagnostic method found the organism in 61% of the children between 1 to 3 months and among 84% of the children between 6 and 9 years old (17, 13).
European countries have lower prevalences of Helicobacter pylori infections than do Latin American and Asian countries. A study conducted among children between 1 and 14 years old in a hospital in Tudela, Spain found prevalences of up to 15.8%. Enzyme immunoassays were used to detect Helicobacter pylori antigen in feces (18). A study done by the Thinder in Sweden showed a serological prevalence of this organism in 16% of pediatric population (19). This suggests that the prevalence of this infection is higher in underdeveloped countries where public health measures are weak than in more highly developed countries.
Our results relating the presence of Helicobacter pylori infection and the grade of chronic gastritis activity are similar to those described in reports by various researchers. The study by Gamez Escalona as well as those by Gallo and Zambon, found highly significant relations between the presence of Helicobacter pylori and active forms of chronic gastritis (15, 20).
We found that the greater the severity of chronic inflammation, the greater was the presence of microorganisms. This finding is the same as that of Gamez Escalona (15) and similar to those of the study by Uhlig in Leipzig, Germany (21).
A study done in Poland found that the grade of chronic inflammation in pediatric patients with Helicobacter pylori infection is correlated to the percentage of CD4 positive T lymphocytes in peripheral blood, while patients who showed no indications of infection with this microorganism had a grade of chronic inflammation related to the percentage of B lymphocytes in peripheral blood (22).
In our study we found gastric atrophy in 6 cases, one of which also had the presence of Helicobacter pylori. In a study conducted in hospitals in Korea and Colombia, gastric atrophy was found in 16% of the population and the organism was identified in all cases in Colombia (23).
In the Hospital de San José in Bogota a study conducted in 2002 (24) evaluated the histopathological findings of gastritis in individuals under 18 years of age over a period of 10 years. That study found 70 cases: 62% were female and 84.4% were located in the antrum. This is similar to what we found in our study, but the frequency of Helicobacter pylori infection found in that study was higher (78%), and the most seriously affected group of patients were older (from 14 to 18 years old). In our case the average age was 9.4 years old. Gastric atrophy occurred in 1.3% of biopsies and metaplasias in 2.6%, both slightly higher than the results in our study.
CONCLUSSIONS
Helicobacter pylori infection is common in chronic gastritis in pediatric patients at Hospital Infantil de San José. The grade of chronic inflammation and levels of polymorphonuclear neutrophil activity are significantly associated with infection by this microorganism. There were very few cases of gastric atrophy or intestinal metaplasia.
Conflicts of interest
None.
REFERENCES
1. Owen DA. Gastritis and carditis. Mod Pathol 2003;16(4): 325-41.
2. Hessey SJ, Spencer J, Wyatt JI, Sobala G, Rathbone BJ, Axon AT, et al. Bacterial adhesion and disease activity in Helicobacter associated chronic gastritis. Gut 1990;31(2): 134-8.
3. Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1984; 1(8390): 1311-5.
4. Pajares JM, Gisbert JP. Helicobacter pylori: its discovery and relevance for medicine. Rev Esp Enferm Dig 2006; 98(10): 770-85.
5. Zhang C, Yamada N, Wu YL, Wen M, Matsuhisa T, Matsukura N. Comparison of Helicobacter pylori infection and gastric mucosal histological features of gastric ulcer patients with chronic gastritis patients. World J Gastroenterol 2005; 11(7): 976-81.
6. Macarthur M, Hold GL, El-Omar EM. Inflammation and Cancer II. Role of chronic inflammation and cytokine gene polymorphisms in the pathogenesis of gastrointestinal malignancy. Am J Physiol Gastrointest Liver Physiol 2004; 286(4): G515-20.
7. Parsonnet J, Isaacson PG. Bacterial infection and MALT lymphoma. N Engl J Med 2004; 350(3): 213-5.
8. Guindi M. Role of Helicobacter pylori in the pathogenesis of gastric carcinoma and progression of lymphoid nodules to lymphoma. Can J Gastroenterol 1999; 13(3): 224-7.
9. Pounder RE, Ng D. The prevalence of Helicobacter pylori infection in different countries. Aliment Pharmacol Ther 1995; 9(Suppl 2): 33-9.
10. Brown LM. Helicobacter pylori: epidemiology and routes of transmission. Epidemiol Rev 2000; 22(2): 283-97.
11. Malaty HM, Graham DY. Importance of childhood socioeconomic status on the current prevalence of Helicobacter pylori infection. Gut 1994; 35(6): 742-5.
12. Patel P, Mendall MA, Khulusi S, Northfield TC, Strachan DP. Helicobacter pylori infection in childhood: risk factors and effect on growth. BMJ 1994; 309(6962): 1119-23.
13. Mahalanabis D, Rahman MM, Sarker SA, Bardhan PK, Hildebrand P, Beglinger C, et al. Helicobacter pylori infection in the young in Bangladesh: prevalence, socioeconomic and nutritional aspects. Int J Epidemiol 1996; 25(4): 894-8.
14. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996; 20(10): 1161-81.
15. Gámez Escalona MM, Mulet Pérez AnM, Miranda Moles Z, Mulet Gámez AnM. Gastritis crónica antral por Helicobacter pylori en la infancia. Rev Cubana Pediatr 2008; 80(1).
16. Sarmiento Q, Chávez C, Pizarro M, Kakarieka W, Vial P, Gotteland R. Infección por Helicobacter pylori y daño gástrico en niños de nivel socioeconómico bajo. Rev Chil Pediatr 1997; 68(6): 251-5.
17. Rodrigues MN, Queiroz DM, Bezerra Filho JG, Pontes LK, Rodrigues RT, Braga LL. Prevalence of Helicobacter pylori infection in children from an urban community in north-east Brazil and risk factors for infection. Eur J Gastroenterol Hepatol 2004;16(2): 201-5.
18. Leandro Liberato SV, Hernandez GM, Torroba AL, Sanchez MF, Leandro Ciriza SE, Gomez AA, et al. Helicobacter pylori infection in the child population in Spain: prevalence, related factors and influence on growth. An Pediatr (Barc.) 2005; 63(6): 489-94.
19. Tindberg Y, Bengtsson C, Granath F, Blennow M, Nyren O, Granstrom M. Helicobacter pylori infection in Swedish school children: lack of evidence of child-to-child transmission outside the family. Gastroenterology 2001; 121(2): 310-6.
20. Gallo N, Zambon CF, Navaglia F, Basso D, Guariso G, Grazia PM, et al. Helicobacter pylori infection in children and adults: a single pathogen but a different pathology. Helicobacter 2003; 8(1): 21-8.
21. Uhlig HH, Tannapfel A, Mossner J, Jedwilayties S, Deutscher J, Muller DM, et al. Histopathological parameters of Helicobacter pylori-associated gastritis in children and adolescents: comparison with findings in adults. Scand J Gastroenterol 2003; 38(7): 701-6.
22. Helmin-Basa A, Michalkiewicz J, Gackowska L, Kubiszewska I, Eljaszewicz A, Mierzwa G, et al. Pediatric Helicobacter pylori infection and circulating T-lymphocyte activation and differentiation. Helicobacter 2011; 16(1): 27-35.
23. Ricuarte O, Gutierrez O, Cardona H, Kim JG, Graham DY, El-Zimaity HM. Atrophic gastritis in young children and adolescents. J Clin Pathol 2005; 58(11): 1189-93.
24. Cadena D, Bastidas RG. Hallazgos histopatológicos de la gastritis en los individuos menores de 18 años, en el Hospital de San José en el periodo 1990 al 2001. (Tesis doctoral). Bogotá: Fundación Universitaria de Ciencias de la Salud; 2002.
1. Owen DA. Gastritis and carditis. Mod Pathol 2003;16(4): 325-41. [ Links ]
2. Hessey SJ, Spencer J, Wyatt JI, Sobala G, Rathbone BJ, Axon AT, et al. Bacterial adhesion and disease activity in Helicobacter associated chronic gastritis. Gut 1990;31(2): 134-8. [ Links ]
3. Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1984; 1(8390): 1311-5. [ Links ]
4. Pajares JM, Gisbert JP. Helicobacter pylori: its discovery and relevance for medicine. Rev Esp Enferm Dig 2006; 98(10): 770-85. [ Links ]
5. Zhang C, Yamada N, Wu YL, Wen M, Matsuhisa T, Matsukura N. Comparison of Helicobacter pylori infection and gastric mucosal histological features of gastric ulcer patients with chronic gastritis patients. World J Gastroenterol 2005; 11(7): 976-81. [ Links ]
6. Macarthur M, Hold GL, El-Omar EM. Inflammation and Cancer II. Role of chronic inflammation and cytokine gene polymorphisms in the pathogenesis of gastrointestinal malignancy. Am J Physiol Gastrointest Liver Physiol 2004; 286(4): G515-20. [ Links ]
7. Parsonnet J, Isaacson PG. Bacterial infection and MALT lymphoma. N Engl J Med 2004; 350(3): 213-5. [ Links ]
8. Guindi M. Role of Helicobacter pylori in the pathogenesis of gastric carcinoma and progression of lymphoid nodules to lymphoma. Can J Gastroenterol 1999; 13(3): 224-7. [ Links ]
9. Pounder RE, Ng D. The prevalence of Helicobacter pylori infection in different countries. Aliment Pharmacol Ther 1995; 9(Suppl 2): 33-9. [ Links ]
10. Brown LM. Helicobacter pylori: epidemiology and routes of transmission. Epidemiol Rev 2000; 22(2): 283-97. [ Links ]
11. Malaty HM, Graham DY. Importance of childhood socioeconomic status on the current prevalence of Helicobacter pylori infection. Gut 1994; 35(6): 742-5. [ Links ]
12. Patel P, Mendall MA, Khulusi S, Northfield TC, Strachan DP. Helicobacter pylori infection in childhood: risk factors and effect on growth. BMJ 1994; 309(6962): 1119-23. [ Links ]
13. Mahalanabis D, Rahman MM, Sarker SA, Bardhan PK, Hildebrand P, Beglinger C, et al. Helicobacter pylori infection in the young in Bangladesh: prevalence, socioeconomic and nutritional aspects. Int J Epidemiol 1996; 25(4): 894-8. [ Links ]
14. Dixon MF, Genta RM, Yardley JH, Correa P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996; 20(10): 1161-81. [ Links ]
15. Gámez Escalona MM, Mulet Pérez AnM, Miranda Moles Z, Mulet Gámez AnM. Gastritis crónica antral por Helicobacter pylori en la infancia. Rev Cubana Pediatr 2008; 80(1). [ Links ]
16. Sarmiento Q, Chávez C, Pizarro M, Kakarieka W, Vial P, Gotteland R. Infección por Helicobacter pylori y daño gástrico en niños de nivel socioeconómico bajo. Rev Chil Pediatr 1997; 68(6): 251-5. [ Links ]
17. Rodrigues MN, Queiroz DM, Bezerra Filho JG, Pontes LK, Rodrigues RT, Braga LL. Prevalence of Helicobacter pylori infection in children from an urban community in north-east Brazil and risk factors for infection. Eur J Gastroenterol Hepatol 2004;16(2): 201-5. [ Links ]
18. Leandro Liberato SV, Hernandez GM, Torroba AL, Sanchez MF, Leandro Ciriza SE, Gomez AA, et al. Helicobacter pylori infection in the child population in Spain: prevalence, related factors and influence on growth. An Pediatr (Barc.) 2005; 63(6): 489-94. [ Links ]
19. Tindberg Y, Bengtsson C, Granath F, Blennow M, Nyren O, Granstrom M. Helicobacter pylori infection in Swedish school children: lack of evidence of child-to-child transmission outside the family. Gastroenterology 2001; 121(2): 310-6. [ Links ]
20. Gallo N, Zambon CF, Navaglia F, Basso D, Guariso G, Grazia PM, et al. Helicobacter pylori infection in children and adults: a single pathogen but a different pathology. Helicobacter 2003; 8(1): 21-8. [ Links ]
21. Uhlig HH, Tannapfel A, Mossner J, Jedwilayties S, Deutscher J, Muller DM, et al. Histopathological parameters of Helicobacter pylori-associated gastritis in children and adolescents: comparison with findings in adults. Scand J Gastroenterol 2003; 38(7): 701-6. [ Links ]
22. Helmin-Basa A, Michalkiewicz J, Gackowska L, Kubiszewska I, Eljaszewicz A, Mierzwa G, et al. Pediatric Helicobacter pylori infection and circulating T-lymphocyte activation and differentiation. Helicobacter 2011; 16(1): 27-35. [ Links ]
23. Ricuarte O, Gutierrez O, Cardona H, Kim JG, Graham DY, El-Zimaity HM. Atrophic gastritis in young children and adolescents. J Clin Pathol 2005; 58(11): 1189-93. [ Links ]
24. Cadena D, Bastidas RG. Hallazgos histopatológicos de la gastritis en los individuos menores de 18 años, en el Hospital de San José en el periodo 1990 al 2001. (Tesis doctoral). Bogotá: Fundación Universitaria de Ciencias de la Salud; 2002. [ Links ]

