











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkAn 82-year-old male who attended the rheumatology out-patient clinic in March 2020 due to the appearance of a necrotic eschar on the pad of the right index finger, as well as loss of strength in said hand. As history of interest, he presented arterial hypertension and dyslipidemia and had undergone a quadruple coronary bypass surgery in January 2020. The patient reported that since the intervention he had paresthesias, hypoesthesia, and loss of strength in the first three fingers of his right hand. A few weeks later he began to develop a necrotic lesion, for which he consulted.
On anamnesis, he denied Raynaud's phenomenon or previous episodes of arthritis, he did not present sensation of dysthermia or other cutaneous or mucosal lesions, nor did he have infectious symptoms at the time he attended the visit. He had not objectified macroscopic alterations in the stools, his digestive rhythm had not changed, he denied loss of weight or appetite and he did not have macroscopic alterations in the urine.
The laboratory tests revealed elevated acute phase reactants (C-reactive protein 132.5 mg/dL, erythrocyte sedimentation rate 60mm/h) and normochromic normocytic anemia (hemoglobin 9.9 g/dL). Autoimmunity was negative, the proteinogram was normal and the urinary sediment was anodyne. With the suspicion of mononeuritis of the median nerve associated with an established digital necrosis, the patient was admitted to rheumatology for study.
Physical exploration
The patient was conscious and oriented in all three spheres, with preserved higher functions.
Complementary explorations
Ultrasound of the right elbow
Anechoic mass with thickened and hypoechoic walls, measuring 60 mm x 107 mm, dependent on the wall of the proximal ulnar artery, shortly after the bifurcation of the brachial artery, with intralesional power-Doppler signal, compatible with pseudoaneurysm vs. parietal aneurysm of the latter. In a position medial to the vascular lesion, the thickened median nerve is observed, with a diameter greater than 58 mm (Fig. 1).

Electromyography/electroneurophysiology
Signs of denervation in the explored muscles, both proximal and distal, dependent on the right median nerve (located at the level of the insertion of the pronator teres muscle), with absence of voluntary activity. The rest of the explored muscles correspond to a different nerve and the same root within normality.
Conclusion
Acute lesion of the proximal right median nerve at the level of the elbow, of severe degree. Angio-CT
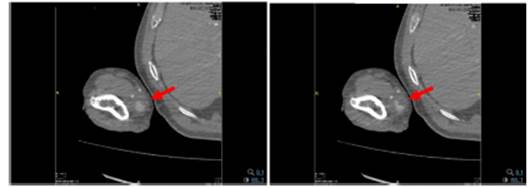
A pseudoaneurysm of the right ulnar artery measuring 22 x 21 mm in diameter, with a neck of 2 mm is observed (Fig. 2).
Evolution
After confirming the diagnosis of pseudoaneurysm of the ulnar artery by angio-CT, we requested evaluation by vascular surgery, which opted for interventional treatment through ultrasound-guided thrombin injection. Ultrasound control was performed 48 h after the procedure, in which total thrombosis of the lesion was observed. At discharge, they prescribed clopidogrel 75 mg/day for five days and clinical monitoring in their consultations.
The control at two and four months evidenced the complete resolution of the lesion, confirmed the recovery of the amplitude of the ulnar pulse and the absence of new necrotic lesions. Regarding strength, the patient attended several rehabilitation sessions in the months following hospital discharge, with complete recovery of weakness (strength 5/5).
Discussion
A pseudoaneurysm is a vascular dilatation due to rupture of the arterial wall, which does not involve the three layers that make it up and communicates with the vascular lumen.1 In general terms, pseudoaneurysms of peripheral arteries are rare and, specifically, the pseudoaneurysms that affect the upper limbs have a prevalence of 2%.1,2 Their etiology is usually traumatic after manipulation of displaced fractures or iatrogenic in the context of invasive vascular procedures.3,4 It is postulated that defective vascular manipulation or a coagulation disorder could participate in their development.(3 Despite their low prevalence, the frequency is currently increasing as a consequence of the greater use of invasive intravascular techniques. In addition, it is also higher in parenteral drug addicts and in hemodialyzed patients.1,5
There are reported cases of compressive neuropathy of the median nerve at the level of the carpal tunnel or the elbow flexure, due to lesion of the brachial or the ulnar artery.2,5 The carpal tunnel syndrome is the most frequent nerve entrapment, with a prevalence of around 2.1% of the general population.6 The ulnar artery coincides anatomically with the median nerve at the level of the elbow, shortly after its bifurcation from the brachial artery. Ulnar artery aneurysms have been known since the 18th century, the first case was described by Guattani, being one of the causes that arise in the differential diagnosis of digital ischemia of the upper limbs.7) However, in the literature there is only one published case of compression of the median nerve by the ulnar artery, since it is most frequently compressed by the brachial artery,1-3 as inferred after the bibliographic review. In our case, the location of the pseudoaneurysm is unusual, since it is located in the most proximal portion of the ulnar artery, just after its bifurcation from the brachial artery.
In the presence of a patient with symptoms of compressive neuropathy, ultrasound could confirm the diagnosis and offer information about the morphology of the affected nerve and the state of nearby structures.6 In addition, it is useful in the differential diagnosis of elbow or forearm flexure injuries and facilitates follow-up.4 In the case of a pseudoaneurysm, hyperechoic flow or material corresponding to an intralesional thrombus will be observed. Finally, it is worth mentioning that it is an advantageous technique in terms of its low cost and wide availability. In relation to other imaging techniques, arteriography continues to be the gold standard, but angio-CT or MRI angiography are also useful and widely used tests. (1
Finally, the treatment of any pseudoaneurysm depends fundamentally on the size, location, and pathogenesis.5 Due to the possibility of embolization or thrombosis, treatment should not be delayed.1 The therapeutic options currently available are endovascular techniques (embolization, stent placement) or traditional surgery, which offers very good out-comes.5 Intralesional thrombin injection was first described by Cope and Zeit in 1986. This technique, which has been shown to be highly effective, requires an ultrasound control at 24 h to confirm that it has been successful.4,5 Surgical treatment is preferred in cases where the lesion progresses rapidly, when there is already established ischemia, and when there is a high risk of distal embolization or small arterial caliber, which makes complex the placement of an endoprosthesis.4,5

