











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Renal angiomyolipomas (AMLs) are common benign renal masses composed of a varying ratio of fat, blood vessels, and smooth muscles. They are often detected incidentally and, although largely asymptomatic, a small number of cases may present with or progress to develop symptoms like pain or complications such as spontaneous bleeding. Multiple treatment options are available, but no consensus or guidelines have been agreed to manage these lesions and, more importantly, there are no established surveillance or discharge protocols. The convention is to consider treatment for AMLs larger than 4cm, which was first proposed by Oesterling et al.1 This has since been debated and reviewed over the years with varying size parameters proposed and additional risk factors described based on the natural history of AMLs, which will discuss through the subsequent sections of the present paper.
The current untailored varied approach among individual practitioners and institutions needs to be streamlined, backed by evidence, and protocols, established to avoid the trap of neglect, excessive surveillance, and unnecessary healthcare expenditures. We have searched the available literature on renal angiomyolipoma through PubMed and Google Scholar to review the evidence and suggest an optimal management pathway. In the present paper, we have focused on the typical AMLs, as they form the bulk of the cohort. Comparatively, the management of hereditary and atypical AMLs has been better defined, and is exemplified in the "UK guidelines for managing tuberous sclerosis complex"2 and "2012 International TSC [tuberous sclerosis complex] Clinical Consensus Conference Recommendations. 3
Methodology
A literature search on AMLs was conducted on PubMed, and it included but was not limited to the terms AML, Renal AML, Angiomyolipoma, and Sporadic AMLs. Only papers published in English that involved sporadic renal AMLs were reviewed, in a total of 46 papers. Information on classification, appearance, diagnosis, presentation, risk factors and management were analyzed to propose a pathway for surveillance of sporadic AMLs including indications for treatment.
Classification
The classification of AMLs is based on radiological features, clinical behavior, and histological characteristics.
Radiological Classification
A new imaging classification of renal AML was proposed and reported by Song et al. 4 in 2016, based on the quantitative assessment of the AMLs on computed tomography (CT) and magnetic resonance imaging (MRI). Prior to this time, renal AMLs were generally classified as either lipid-rich or minimal fat lesions based on imaging and histopathological features. Song et al. 4 classified AMLs into three subtypes according to the amount of fat within such lesions quantified by CTor MRI: fat-rich, fat-poor, and fat-invisible.
On unenhanced CT (UECT), fat-rich AMLs are characterized by the presence of low attenuation areas measuring -10 Hounsfield units (HUs) or less, whereas in both fat-poor and fat-invisible AMLs these areas measure more than -10 HUs on UECT. 4 Using the chemical-shift imaging (CSI) MRI technique, which consists of opposed-phase and in-phase gradient echo sequences with signal intensity (SI) measurements, fat-poor AMLs, which contain a small amount of fat, would present a tumor-to-spleen SI ratio lower than 0.71, and an SI index greater than 16.5%. On the contrary, fat-invisible AMLs would present a tumor-to-spleen SI ratio of 0.71 or greater, and a SI index of 16.5% or lower. Hence, fat-poor AMLs may be differentiated from fat-invisible AMLs using CSI MRI. 5-7
Therefore, care and attention are required to control the size and placement of the regions-of-interest (ROIs) during quantitative assessment of the lesions on both CT and MRI to avoid inaccurate registration of the size of the low attenuation areas on UECT and the SI on MRI, which can lead to miscalculation and consequently misclassification of the subtypes of AML. 4 Table 1 demonstrates the radiological features of AMLs. 4
Table 1 Radiological classification of renal AMLs adapted from Song et al. 4

Abbreviations: AML, angiomyolipoma; CSI, chemical-shift imaging; MRI, magnetic resonance imaging; ROI, region of interest; SII, signal intensity index; TSR, tumor-to-spleen ratio; UECT, unenhanced computed tomography.
Rarely, renal cell carcinoma (RCC) may have a fat component, which is strongly suggestive of AML but is not pathognomonic. Approximately 5% of AMLs are fat-poor and may mimic RCCs. 8 Here, the lack of calcification on CT may favor diagnosis of AML. 5,6 A rare variant of AML is the eosinophilic AML (eAML); first described by Eble et al., 9 it is characterized by predominant perivascular epithelioid cells and, radiologically, it presents distinct differences from AML but close resemblance to RCC. 10 Fat-poor AMLs with high cellular content, eAMLs show variable enhancement on CT and, on MRI, high cellular content with absence of fat. Pathological bleeding, necrosis, and hyalinization contribute to the heterogeneity, making them difficult to distinguish from RCCs on imaging. 10-12
Clinical Classification
While 80% of AMLs are sporadic, 20% are hereditary, associated with tuberous sclerosis (TS) or pulmonary lymphangioleiomyomatosis (LAM). 13,14 The genetically predisposed presentations are likely to be multiple, progressive, more aggressive, and affect patients at a younger age. Hence, this potential aggressive nature must be reflected in their surveillance/management. Identification of the clinical features is helpful in differentiating hereditary cases from sporadic cases, which form the vast majority of presentations.
A total of 80% of TS patients have AMLs; TS is a multisystem, autosomal dominant condition characterized by hamartomas, mainly in the brain, lung, skin, and kidney. This occurs due to mutation of either one or both inhibitory genes, called tuberous sclerosis complex 1 (TSC1), on chromosome 9q34, which codes for protein hamartin, and tuberous sclerosis complex 2 (TSC2), on chromosome 16p 13.3, which codes for protein tuberin. 15,16 As a consequence, hamartin and tuberin fail to form an inhibitory complex against mammalian target of rapamycin (mTOR). This leads to unopposed activation of mTOR, resulting in increased angiogenesis, protein synthesis, cell growth, and development of characteristic hamartomas. Tuberous sclerosis is characterized by mental retardation, neurological symptoms, epilepsy, adenoma sebaceum, and other hamartomas.
A rare disease that most commonly affects women, LAM is characterized by lung cysts and lymphatic abnormalities, chylous pleural effusion, recurrent pneumothoraces, and cystic lungdisease. 13,17-21 The pathophysiology of its association with AML is similar to that of the association of AML and TS.
Histological Classification
Histologically, AMLs are classified as typical (triphasic) or atypical (monophasic, epithelioid). Typical AMLs are triphasic, as they are composed of varying proportions of blood vessels (angio), smooth muscles (myo), and adipocytes (lipo). Some AMLs may be composed largely of one element and hence are described as monophasic (atypical). A variant of this is epithelioid AML (eAMLS), an AML with predominant epithelioid cells, abundant eosinophilic and granular cytoplasm, and minimal or no adipocytes. These may be aggressive with potential for malignant transformation; hence, they must be differentiated from typical AMLs to streamline management. Histologically, eAMLS may resemble RCCs, and the immunohistochemical difference is the presence of markers such as melan-A, HMB - 45 (immunohistochemical test), caldesmon, and smooth-muscle actin. Generally, if more than 5% of the specimen contains an epithelioid component, then it is described as an epAML, which has a poor clinical outcome compared with typical AMLs. 12 However, it is difficult to identify malignancy in eAMLS, as not all cases with cellular atypia are malignant. 10 The adverse histological features associated with malignancy have been described by two large multicenter retrospective studies22,23 as: a large epithelioid cell component, severe nuclear atypia, extent of nuclear atypia, mitotic count, presence of atypical mitotic figures, necrosis, presence of lymphovascular invasion, tumor size larger than 7 cm, and renal vein invasion.
Diagnosis and Imaging Modality
Presentation and Symptoms
More than 50% of AMLs present as incidental findings on ultrasound (US) or CT scans, and most are asymptomatic at diagnosis. 18,24 Symptoms at diagnosis are present in less than 15% of cases, and they may be related to retroperitoneal hemorrhage. 18 Wunderlich syndrome is a rare condition resulting in spontaneous non-traumatic renal bleed, which may be caused by renal angiomyolipoma and RCC. 25 In up to 10% of cases of Wunderlich syndrome, massive and life-threatening retroperitoneal hemorrhage occurs, 24 which is the main clinical concern. Other symptoms may include flank pain, palpable mass or painless hematuria. Studies13,26,27 also suggest symptoms of urinary tract infection and renal failure. 13,26,27
Around 80% of AMLs are sporadic, and 20%, hereditary. The latter are linked commonly to TS and LAM with symptoms and presentation as aforementioned. Here, the associated AMLs have a more aggressive tendency, and the presence of symptoms and progression are more likely. About 80% of TS patients develop AMLs, which are frequently bilateral, multifocal, and have a propensity to grow and suddenly bleed. Patients diagnosed with LAM, however, have a high prevalence of symptomatic AMLs and should, therefore, be screened for renal AMLs at the time of diagnosis and undergo surveillance. 17
A rare variant of renal angiomyolipoma, epAMLs can occur in patients with or without TS, and it may be malignant. 11 In a series of 437 consecutive cases of AML, the authors28 identified epAMLs in 4.6% of the cases. In total, 22% of epAMLs present with invasion or metastasis with higher mitotic activity, indicating higher risk of metastasis. 29
Gross Appearance
Macroscopically AMLs appear as well-circumscribed fatty lumps. They may be single or multiple, unilateral or bilateral. The cut surface may display the vascular, smooth-muscle, and fatty components as red, grayish-white, and yellow respectively. The tumor may involve the intrarenal venous system, the renal vein, or the vena cava, depending on its location and size. Rarely, cystic components may also be displayed. 30
Radiological Features
Often observed as incidental imaging findings, AMLs can be identified on US, UECT, MRI scans, but US and CT are more commonly used.
On grayscale US scans, fat-rich AMLs are typically markedly hyperechoic comparable to the echogenicity of renal sinus fat, with posterior acoustic shadows. The hyperechoic appearance (characteristic bright echo pattern) is the US reflection from the fatty component, which varies with the amount of fat in the lesion. The acoustic shadowing is due to the tissue interfaces between the elements of the AML. 26 Fat-poor and fat-invisible AMLs, on the other hand, are generally less echogenic or may be isoechoic compared with the renal parenchyma. Due to overlapping sonographic features of different subtypes of AML and RCC, US scans alone cannot be used to confidently confirm the diagnosis of an AML. 31
When a solid renal lesion has been identified, one of the key roles of imaging is to attempt to differentiate a benign from a malignant lesion and, whenever possible, to provide a specific diagnosis. While classic fat-rich AMLs are usually easy to diagnose on both CT and MRI, differentiating fat-poor and fat-invisible AMLs from RCC subtypes remains challenging, since these lesions all share some common imaging features.
On UECT, fat-rich AMLs show hypoattenuating foci with -10 HUs or less. Contrast-enhanced CT (CECT) is usually not required for the diagnosis of a fat-rich AML, but may be necessary for treatment planning in cases of high risk of bleeding, and embolization is to be considered. On MRI, fat-rich AMLs show variable foci of hyperintensity on both T1-weighted (T1W) and T2-weighted (T2W) imaging that demonstrate signal loss when the fat-suppression technique is applied, thereby confi rming the presence of bulk fat and the diagnosis of a fat-rich AML. One should also bear in mind the rare incidence of RCCs containing bulk fat. However, such RCCs are reported to be associated with additional features such as calcifications and necrosis, and usually contain only a small amount of fat relative to tumor size. 32,33
Intra-AML aneurysms of 5 mm or more have been shown to be more strongly associated with the likelihood of hemorrhage than overall size. 34 In fact, sensitivity and specificity rates of 100% and 86% respectively to predict hemorrhage in the presence of intratumoral aneurysms of 5mm or more compared with a specificity of 38% for the 4-cm AML threshold. 34 Hence, in selective cases of vascular lesions with a prediction of riskof bleeding, CECT may be considered to assess intratumor aneurysm and plan for embolization.
Digital subtraction angiography (DSA) can identify AMLs as hypervascular lesions characterized by well-defined hypervascular masses with dense arterial networks ob-served in the arterial phase. The tortuous vessels have a "sunburst" appearance. In the venous phase, the peripheral vessels have an "onion peel" appearance. Micro- or macro-aneurysms may also be observed with absent arteriovenous shunting.
The CSI MRI technique is used to differentiate fat-poor from fat-invisible AMLs when a renal AML has presents more than -10Hus on UECT. As clear-cell RCCs, which contain an abundance of intracytoplasmic fat, also show similar CSI MRI characteristics as those of fat-poor AMLs, that is, a tumor-to-spleen SI ratio lower than 0.71 and an SI index greater than 16.5%, this imaging technique alone cannot reliably be used to differentiate fat-poor AMLs from clear-cell RCCs. The qualitative assessment of the lesion may be helpful in this situation, in which fat-poor AMLs are typically mildly hypointense compared with the renal cortex on T2W imaging as opposed to clear-cell RCCs, which are usually hyperintense. 35,36 The presence of tumor necrosis almost virtually rules out the diagnosis of an AML. 35
Prior reports36,37 on the use of dynamic contrast-enhanced (DCE) imaging to differentiate minimal-fat AMLs from RCCs have been inconsistent, since it is likely that both fat-poor and fat-invisible AMLs, which could have different DCE imaging characteristics and present histological variations, were considered as a single subtype. Earlier studies have reported minimal-fat AMLs and clear-cell RCCs showing strong early enhancement on DCE CT, 36 and homogenous and prolonged enhancement as valuable predic-tors of minimal-fat AML. 37
Fat-invisible AMLs share common imaging features with papillary RCCs, and these two lesions cannot be reliably differentiated from each other based on imaging alone. Both lesions are typically homogeneously hyperattenuating on UECT and hypointense on T2W imaging. Neither show signal loss on CSI MRI due to the paucity of fat. Fat-invisible AMLs may demonstrate homogenous and prolonged enhancement similar to that of papillary RCCs. As such, when a renal lesion demonstrates all of these imaging features, biopsy may need to be considered to differentiate among a fat-invisible AML, an eAML, and a papillary RCC.
The radiological features of AMLs are summarized in Table 2. 4,13,18,26,31,32,38
Table 2 Radiological features of AML adapted from Vos and Oyen13

Abbreviations: CSI, chemical-shift imaging; MRI, magnetic resonance imaging; UECT, unenhanced computed tomography; US, ultrasound.
Biopsy
Radiological identification of AMLs is sufficient for the diagnosis in most cases. Biopsy of the mass lesion may be indicated in cases ofdiagnostic dilemma, such as fat-invisible AML, suspicion of eAML, or RCC and inconclusive imaging results. However, if the lesion has more than 3 cm or there is evidence of massive hemorrhage, then, proceeding with treatment may be more appropriate to avoid further bleed-ing, and because eAMLs and RCCs are more presumable. 13,31
Concerns and Complications: When and Why Is Treatment Indicated?
Many clinicians have asked the question: if sporadic AML is a benign lesion, why and when does it need treatment, and what are the guidelines for management? On the other hand, there are established guidelines2,3 for AMLs with hereditary predisposition, which, therefore, are not the focus of our discussion. We will continue to focus on the sporadic cases and their management, reviewing the natural history and management proposed in the literature.
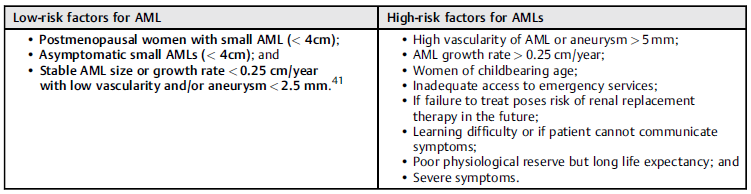
The traditional convention is to consider treatment for AMLs larger than 4 cm. This was first proposed by Oesterling et al.,1 and has since been debated and reviewed over the years, with one paper18 suggesting that 70% of AMLs larger than 4 cm are asymptomatic. Several studies emphasize the importance of the size of the vascular component over the size of the fatty mass in predicting the risk of bleeding and need for intervention, 26,39 with no difference in the growth rate of AMLs shorter or greater than 4cm. 40 Overall, more than 90% of AMLs grow very slowly or not at all, regardless of the initial size, while only 9% grow more rapidly, at rates of 0.25 cm per year or more, which may pose a slightly higher risk of rupture and bleeding. 40 When they measure less than 4 cm, AMLs are rarely symptomatic, but those larger than 4 cm are more likely to be symptomatic (6.6% versus 31.9% respectively). 31 Thus, the symptoms can provide an indication of tumor growth and, in asymptomatic cases, the degree of vascularity and the presence of intratumor aneurysms measuring 5 mm or more are risk factors for rupture. Other factors indicating the need for treatment are bleeding or increased risk of bleeding, presence of symptoms such as pain or hematuria, eAML variant, and suspicion of malignancy.
The literature suggests that it is reasonable to consider prophylactic treatment in cases considered high-risk AMLs and those associated with high-risk factors.
AML factors:
Patient Factors:
Women of or prior to childbearing age (along with patient and lesion-specific risk factors); 41
Patients whose AML rupture or subsequent emergency treatment risks precipitating renal replacement therapy (such as underlying kidney disease, solitary kidney); 41
Patients with intellectual or communication difficulties, in whom symptom evaluation may be challenging; and
Patients with poor physiological reserve but long life expectancy conferring high lifetime risk of rupture.
Social Factors:
Active Surveillance
After confirmation of the diagnosis, if the indications for treatment have not been met, then active surveillance is by and large the most appropriate treatment. There are no current guidelines for the frequency and modality of imaging. It is in fact suggested in the literature7 that surveillance imaging of all sporadic AMLs is unlikely to impact management decisions, but preference for a follow-up strategy may help build the evidence gap.
Selective Arterial Embolization
This is minimally invasive and, as such, should be the first-line treatment option (in which diagnosis is certain and treatment is indicated), provided this is technically feasible and the patient is hemodynamically stable. Sometimes preoperative embolization is considered to reduce the difficulty and complications of surgery. 7,18
The complications of embolization include pyrexia, pain, nausea, vomiting, and leucocytosis, which usually occur within the first couple of days of the procedure and are typically self-limiting with supportive management. Embolization of non-target normal renal tissue, renal infarction, and abscess formation are rare but recognized complications. The effects of embolization may vary due to the varying composition of AMLs, with recurrence and repeat bleeding remaining a concern. The literature42-44 suggesta a varying need for reembolization, ranging from 17% to 37%.
Following treatment, if symptoms persist or recur, repeat imaging (preferably CT angiography) should be performed to assess residual or recurrent tumor volume, residual vascularity, and the presence and size of intratumor aneurysms. As these factors are associated with a risk of hemorrhage, they should be assessed and reported. A tumor which remains unchanged in size but has reduced vascularity and no aneurysms may represent satisfactory treatment response. However, if symptoms persist, then repeat or alternate treatment may be offered. In cases in which the residual AML is poorly vascular, further embolization is probably of limited benefit, and alternate treatments such as ablation or resection may be preferable.
Surgical Management
It includes offering a partial or radical nephrectomy. Ideally, out of the two options, nephron-sparing surgery should be considered, as this will limit nephron loss in the future due to recurrence, multifocal disease or other comorbidities.
Surgery should be considered when an AML is too large for embolization, in the event of failure of the embolization, presence of vascular malformation, or if there is suspicion of malignancy. In uncontrolled hemorrhage and hemodynamically-compromised patients, nephrectomy may be lifesaving. 42,45
Ablation
Cryoablation, microwave ablation, and radiofrequency ablation are alternatives to the aforementioned invasive procedures. They have been used in selective cases, such as those of solitary kidney or hereditary cases, with an investigation of the safety and efficacy of the procedure and aiming to preserve renal function. 43,44 They are more commonly used for RCCs or suspected RCCs, but safety and efficacy have also been reported for AMLs in a small number of patients. The reported average sizes of AMLs treated with these techniques are of ~ 5cm. Ablation can be applied with percutaneous or laparoscopic techniques, and they work by inducing cell death. These procedures can also be combined with simultaneous biopsies if required. 7 Little evidence is available on its use on larger or symptomatic AMLs; and a complication rate of 13.3% has been reported in the literature. 46
Drugs
Drug treatment is not currently an option for the treatment of sporadic AMLs, but it can be offered for the management of hereditary AMLs. Therefore, it will be discussed only briefly. Sirolimus and Everolimus are mTOR inhibitors that interrupt tumor progression and promote regression of the lesion(s). They are offered for asymptomatic AMLs measuring more than 3 cm and associated with LAM and TSC. 13
Follow-up Imaging
The role of follow-up imaging is uncertain in treated patients who remain asymptomatic, but practitioners and patients are likely to want at least one radiological assessment of posttreatment change. The report should include the residual or recurrent tumor volume, residual vascularity, and presence and size of intratumor aneurysms, as these will help assess the outcome of treatment and if further treatment will be needed, especially if there are persistent or recurrent symptoms.
Conclusion and Recommended Management Pathway for Sporadic AMLs
Renal AMLs are common benign renal masses with varying amounts of fat, blood vessels, and smooth muscle. The fatty component is the characteristic feature that enables diagnosis based on imaging, and the lack of this element presents a diagnostic challenge. Needless to say, establishing the diagnosisis the first step, followed by decision regarding the treatment and surveillance or discharge.
The natural history of AML is poorly understood, with no strong evidence for the exact cut-off size for treatment. The traditional convention, as proposed by Oesterling et al., 1 is to consider treatment for AMLs larger than 4 cm, which is a widely accepted size guide used in decision making. However, size alone is not a strong indicator of the risk of bleeding, with various cut-offs, generally larger sizes, suggested over the years. Most sporadic AMLs grow slowly, at an average rate of less than 0.02 cm per year, while 9% show faster growth, of 0.25cm per year. 40 The stronger indications for treatment are symptomatic AMLs and high-risk factors for hemorrhage, which justify the prophylactic treatment.
While the choice of treatment is a relatively easier decision to make, there is a lack of surveillance and discharge protocol. Following the present literature review and given the aforementioned characteristics, the benign nature of the lesion and the lack of guidelines, we propose the algorithm shown in Fig. 1 for the management of sporadic AMLs.

Although an US scan may suffice for diagnosis, we also suggest a CT scan at diagnosis and at follow-up in 12 or 24 months to assess the size of the vascular component, as this is the most significant predictor of hemorrhage. The growth and changes noted at this stage can determine the subsequent imaging modality. If the growth rate or vascular component of the AML is significant, symptoms or any of the aforementioned risk factors develop, then CT is likely to be more helpful, whereas in low-risk cases an US scan may be sufficient.
Following a uniform pathway will help clinicians' decision in management planning and will allow patients to benefit from uniformity of care provision across the region or nation, maintaining a uniform cost-benefit profile. It will also form the basis for a future consistent database to further stream-line management and to incorporate into guidelines using the evidence base. Following a standardized surveillance protocol will also allow future prospective studies to evaluate and improve said protocol.

