










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Cuidarte
Print version ISSN 2216-0973
Rev Cuid vol.8 no.3 Bucaramanga Sep./Dec. 2017
https://doi.org/10.15649/cuidarte.v8i3.464
Editorial
Exploring the relationship of threshold concepts and Hodges’ model of care from the individual to populations and global health

1Master of Research. Lancashire Care NHS Foundation Trust, Ormskirk, Lancashire, United Kingdom
Through academia, professional disciplines seek – whenever possible – to base their actions on theory rather than fact and historical practices. This serves to improve certainty and place curricula, research, and practice on the best footing in terms of knowledge and quality. This emphasis extends to the workplaces in which professionalised disciplines are learned and practised. In healthcare, great importance is placed upon evidence-based findings to support clinical practice1. Although subject to ongoing debate, the quality of research is assessed against a yardstick that culminates in a ‘gold-standard’ of clinical trials and systematic reviews. What healthcare professionals do, should, whenever possible, be based upon evidence, not ritualised practices and missives, such as “I was trained this way” and “This is how we do things here”.
Nursing boasts a rich and ongoing literature devoted to existing and new theories and models of nursing and health care2. The common sense fact behind this is of course that there is no single mental model; contexts, perspectives and frames of reference often change rapidly band in-situ (what we often refer to as ‘real-time’). There is a requirement that theories and models of nursing and health care are tested and can ultimately contribute to evidence-based practice and inform health policy; this need is even greater today, given the everincreasing costs of healthcare, demographic change, and various pressures on the healthcare workforce and global economies. From the above, it becomes clear that a description with reference to a diagram to explain Hodges' model3 is insufficient if theory in nursing and nurse education is to be progressed and practice assured in terms of patient/public safety and high quality of care. This editorial seeks to explore the following questions:
What are threshold concepts (TCs)?
How do TCs relate to Hodges' model?
How can Hodges' model and the concept of thresholds inform our theorizing about healthcare?
What are the prospects for research for Hodges' model with TCs?
Hodges' model was created in the early-mid 1980s by Brian Hodges, a Senior Lecturer at Manchester Polytechnic (now Manchester Metropolitan University)3. Hodges saw that a model of nursing was needed for several purposes: curriculum development, reflective practice, person-centred care and acts as a bridge to narrow the theory-practice gap. The result was Hodges' Health Career – Care Domains - Model which Hodges taught up to retirement in the early 1990s. Hodges' model is best explained with reference to a diagram as per Figure 1. This figure combines the model's axes and knowledge domains and shows that Hodges' model is simplistic in its basic form. The model is also potentially complex as a form of ‘rich picture’. As can be seen in Figure 1, the model's two axes intersect. The horizontal axis is the HUMANISTIC-MECHANISTIC; the vertical represents the INDIVIDUAL-GROUP. The axes give rise to four quadrants and these provide four spaces, or domains within which concepts can be placed. The domains, as indicated in the figure are not placed arbitrarily, but are derived through a series of questions concerning both the subjects (persons) and agents (formal and informal) of healthcare and the types of activities and events that might occur to deliver care. Hodges' model provides a space that can be described as deliberative, argumentative, or reflective.
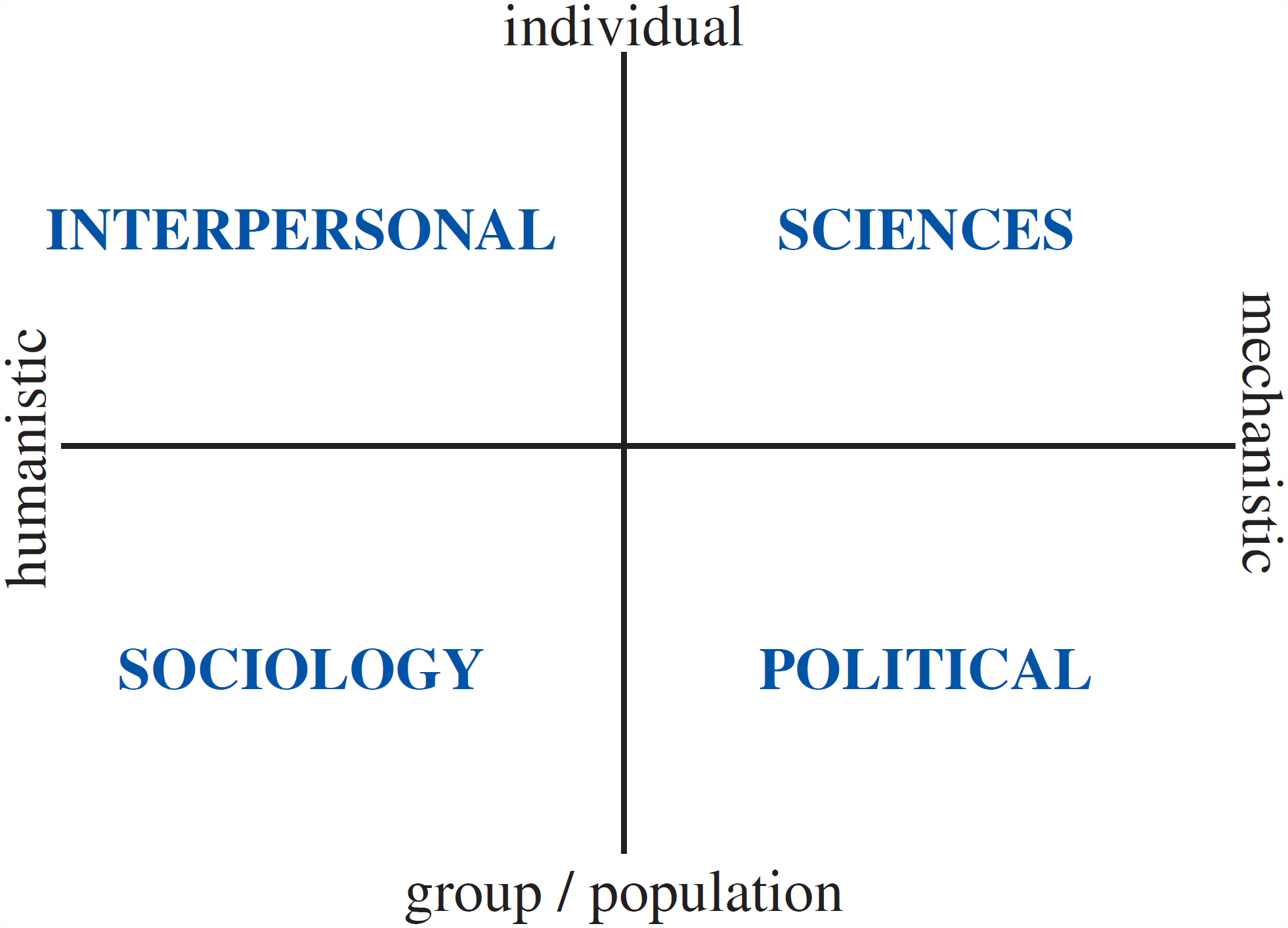
From the simplified nature of the model, it is an easy step to see the model as idealised; a function of many models and frameworks. Figure 1 can still prompt many questions. How are we intended to navigate the axes? Are they equivalent in breadth of the continua represented? What is the ‘unit’ of measurement? Taking the individual-group axis first, we can see where the idealisation of person-centred care is located. This is not just by virtue of labelling (individual), but is associated with the knowledge that it invites around it. The top two domains of interpersonal and sciences instantiate the two forms of nursing care upon which all nursing is based and around which a parity of esteem debate still rages4. These are mental healthcare (interpersonal) and physical care (the sciences). Within these domains, we can conceptualise the various activities that make up being human and doing nursing. Communication is a key concept in which all healthcare professionals must achieve and maintain competency5. In addition, the model – as a whole – can also be considered, according to need, as being found within a spiritual domain.
If the individual, whether as patient, or carer, is the preserve of the upper half of the model and the clinical encounter we must extend the individual beyond this. In public health we see the potentially life or death connection between the individual and others in ‘contact tracing’ or ‘partner notification’ that is prioritised in communicable disease. The sociological and political domains require consideration of the relational: reflection, reflexive, human relationships and power relations6. The inclusion of a POLITICAL domain increases the model's conceptual scope of the model and its relevance.
Even in the horizontal axis we see how nursing and this model is predicated on the person as the primary focus. The various things we need to describe, be they objects, ideas, concepts, behaviours, outcomes, tests, data, phenomena all fall into one of two broad categories. They are either humanistic, or mechanistic. Acknowledging idealisation once again, of course context is critical, there can be overlap. The model is situated, a concept that spans nursing and education. For nursing, this means practice is to the fore7, Nursing might and must be directed by evidence and best-practice, but as Mitchell argues it is the entirety of the person-person encounter that is nursing7.
Thresholds abound in day-to-day life, the sciences, myth, culture, history and in the literature. Being a guest in someone's home is something we negotiate from a young age beginning with family. Crossing the physical threshold of a patient's home as a professional was encountered as a student nurse in 1979. Gravity is a threshold we take for granted until we fall. If instability occurs then consequences follow: heart muscle becomes arrhythmic, a building might collapse, as with an economy, lava erupt, tributaries flow and a population explode. Individually and socially, we quickly recognise the threshold of pain – physically and psychically. The two primary thresholds are of course death and taxes. Thresholds in economics and finance define and drive markets and levels of taxation. Variation in queuing and operational research is accommodated using fixed and adaptable algorithms that can alter a threshold according to the size of a queue8. In the field of toxicology, Crump9 lists types of threshold: statistical, practical, apparent, operational, “threshold”, acceptable, pragmatic, regulatory and biological.
Before progressing to more details of TC, we should define threshold and threshold concept. ‘Threshold’ can, therefore be defined as the magnitude or intensity that must be exceeded for a certain reaction, phenomenon, result, or condition to occur or be manifested: nothing happens until the signal passes the threshold [as modifier]: a threshold level.
Taylor10 goes to the source for a definition: “Meyer et al.11 discuss the definition of a threshold concept as a transformative gateway, possessing certain properties (for example, being integrative and possibly ‘troublesome’) that leads to the understanding of new and conceptually more difficult ideas”. There is insufficient space to critique threshold concepts in detail, but details follow of a comprehensive literature resource on TCs.
The research interest in TC is also evident through textbooks, papers, a conference series, and a comprehensive online bibliographical resource hosted by University College London. Entries range from ‘academic professional development’ to ‘widening participation’ to more recognisable disciplines, such as physics, engineering, and mathematics. A keyword directory covers education across the topics of early childhood education, lifelong learning, mentoring, primary and secondary school education, technology-enhanced learning, and many more. Healthcare is also well represented. Table 1, from the bibliography, outlines the features of TCs and provides the references retained within the table.
Table 1 Feature of a threshold concept
| Transformative | Once understood, a threshold concept changes the way in which the student views the discipline. |
| Troublesome | Threshold concepts are likely to be troublesome for the student … knowledge can be troublesome e.g., when it is counter - intuitive, alien or seemingly incoherent. |
| Irreversible | Given their transformative potential, threshold concepts are also likely to be irreversible, i.e., they are difficult to unlearn. |
| Integrative | Threshold concepts, once learned, are likely to bring together different aspects of the subject that previously did not appear, to the student, to be related. |
| Bounded | A threshold concept will probably delineate a particular conceptual space, serving a specific and limited purpose. |
| Discursive | Meyer et al.,11 suggest that the crossing of a threshold will incorporate an enhanced and extended use of language. |
| Reconstitutive | “Understanding a threshold concept may entail a shift in learner subjectivity, noted. Such reconstitution is, perhaps, more likely to be recognised initially by others, and also to take place over time”. |
| Liminality | Meyer et al.,11 have likened the crossing of the pedagogic threshold to a ‘rite of passage’ (drawing on the ethnographical studies in which a transitional or liminal space has to be traversed; “in short, there is no simple passage in learning from ‘easy’ to ‘difficult’; mastery of a threshold concept often involves messy journeys back, forth, and across conceptual terrain”. |
Thresholds of an often-critical nature come to the fore in respect of health, care and nursing. When things are stable, we take no heed. If a threshold denotes anything, it indicates a potential, a new signal – new information that might follow that may or may not denote change of some kind. Particles and fluids have their dynamic also acting as an analogy for the journey that we call life: from the micro (sub-atomic) level of cells pumping protons with a death threshold associated with cell functioning and apoptosis12, to the macro level of geomorphological phenomena13. Colman14 defines the absolute threshold found in neuroscience and psychophysics, the level of stimulus that can be detected by the human senses. Ecological and environmental thresholds often feature in the news when they are breached and public safety might be affected. Industrial hygiene and safety investigators test and refine safety thresholds for chemicals in the work environment.
More generally, the existence and utility of thresholds (as noted above) soon make themselves evident in health and social care. Caring is fundamental to nursing and this is where we can begin. Clouder15 investigates caring as a threshold concept, stressing the ethical, moral and personal challenges that professional caring demands. Threshold concepts have been explored and proposed, thus: differentiating thresholds within panic disorder16; surgically in clinical transplantation17; within mental health to promote patient-centred care in interprofessional education18; the social model of disability as a TC19; while Stacey & Stickley20, explore recovery.
Many of the TCs above are so broad as to be problematic. The laudable aim of person-centred care is troublesome when so much of what we do is organised according to service-centred foundations. Patient-professional communication is central as per Clouder17, but the thresholds for accountability bring in collective actions with their own structure from revalidation through to decisions on mental capacity, safeguarding, clinical-managerial supervision and whistleblowing.
Figure 2 maps TCs from the literature (underlined) and additional candidates directly upon Hodges' model in the form of a 2x2 table. When we contemplate stress-vulnerability, this quickly becomes learning, reflection, health literacy and a movement towards self-efficacy.
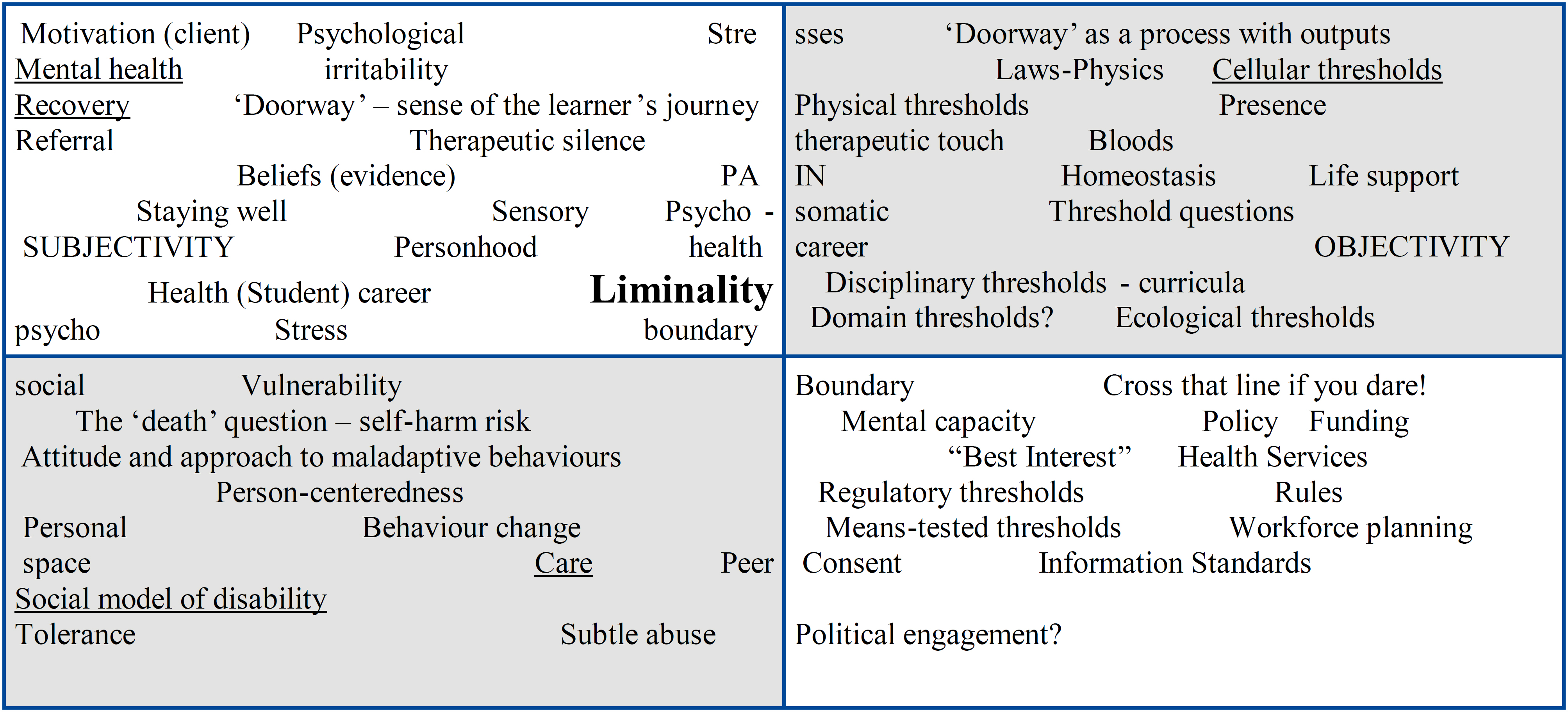
Although the axes of Hodges' model appear dichotomous, as polarities they differ not only in what they seek to represent, but also possibly in what they are? Are they continua, serving a need to differentiate through oppositions? In Hodges' model, we can discern a series of multidimensional and interrelated continua, which form a framework. While simply 2D to begin, the axes in Hodges' model can quickly take on multidimensional and interrelated form. We can project time through the model to create a series of frames, frames populated according to our purpose.
As already noted, taken at face value (Figure 1), Hodges' model `speaks' of continua and conceptual domains, but how does Hodges' model relate to thresholds and threshold concepts? The full title of Hodges' model bears the health career. This refers to an individual's life, the life chances that their birth, upbringing, health, education and circumstances affect upon them. Health career can be linked to the TC feature of liminality.
If thresholds are defined by their being tested, crossed, sustained and broken then Hodges' model can work to test, cross, sustain and break what are often silos of knowledge and practice. This acknowledges the role of Hodges' model in facilitating holistic, integrated and multidisciplinary care at least in its conceptual foundations. Hodges' model could be instrumental in defining holistic care, the model as acting as a dashboard that signifies various thresholds. Emergency care in Hodges' model will be centred upon the SCIENCES domain. True holistic care will touch all the domains, plus the spiritual, which encompasses all.
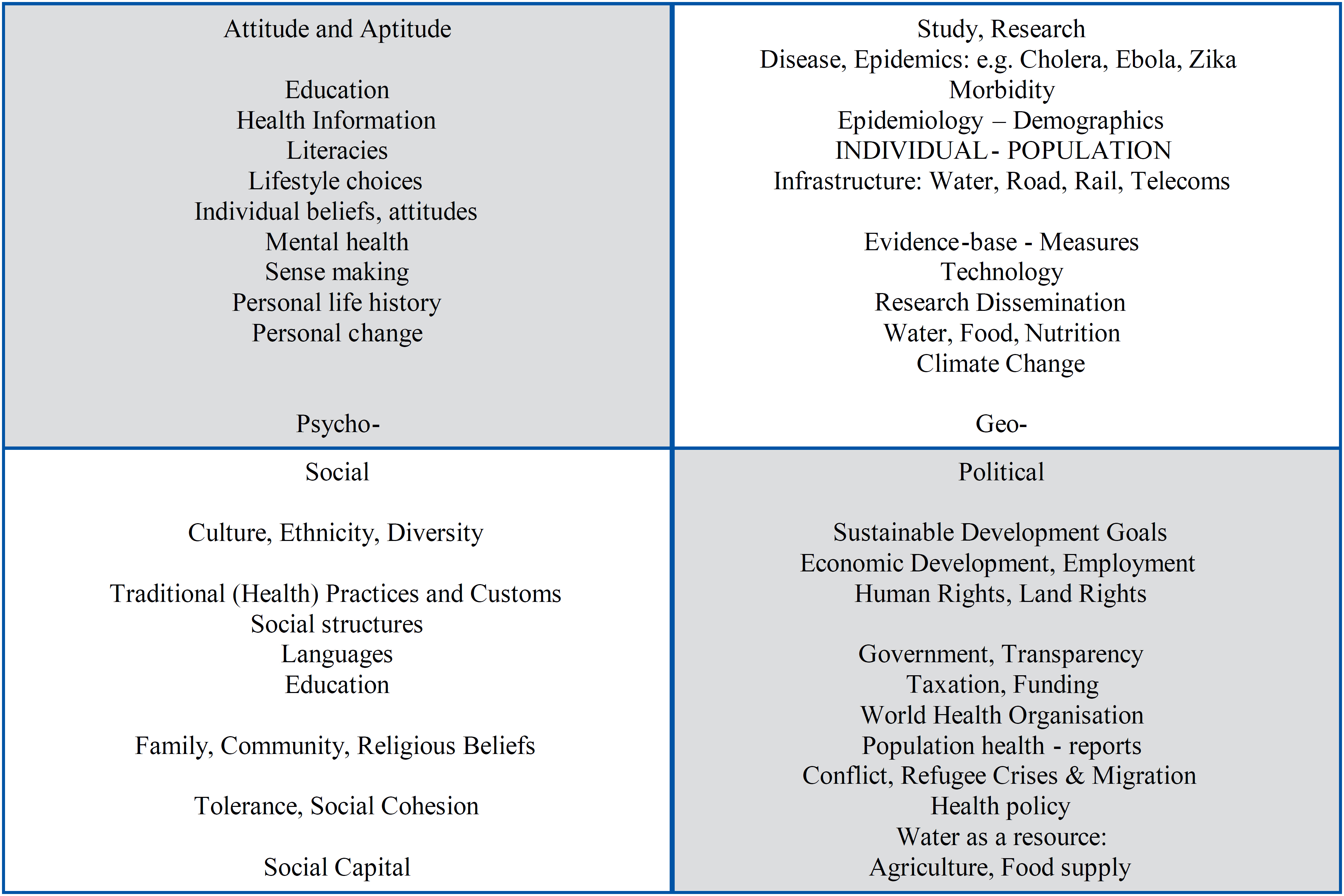
An example is needed and will be provided next. The intention is to demonstrate the potential utility of Hodges' model to conjoin ipseity, that is, the self, individual identity and personhood with the group and population. Further studies will seek to establish how Hodges' model can be used in case formulation not just at an individual level – were social factors inform assessments and evaluations – but in community and global health development. Hodges' model is further suited to this task as the model supports precontextualisation by helping us to anticipate the future and recontextualization in seeking to make sense of the past. Overarching this temporal dimension is the fact of Hodges' model being so general and independent of any particular discipline to be transtheoretical. There is no single theory that can explain, predict or account for the validity of Hodges' model. The example that follows is necessarily broad touching on several themes of global health and development as outlined in Figure 3. The same 2x2 table is adopted to reflect the model's care domains and basic structure.
Being an expert is in a sense a claim to liminality. Liminality is not an end-point, as the increased need for lifelong learning reveals. As an adjunct to reflective practice, Hodges' model can surely claim something in common with TCs? If a lay definition of an expert is someone who knows when, how and which corners to cut for reasons of efficiency, efficacy, effectiveness; then perhaps the utility of TCs may lie in the disciplinary routing they facilitate – as discussed in the literature. This also applies to beginners. There is a possible synergy in two respects that involve the mapping metaphor so often ascribed to utilising concepts fully. There are clearly ‘disciplinary TCs’ even while this relies on the presence of a knowledge-silo mentality. Such bounded TCs are defining characteristics of expertise, professional differentiation and professional boundaries, delineating scope of practice.
This editorial informs a practice related project to instantiate Hodges' model within a web-based reflective workbench. Users will be able to input, select, organise and map a case using Hodges' model as a structure. It is envisaged that users will be presented with an interface according to their platform registration. Learners would be able to tag the content of their case in a variety of ways, including what they consider to be `troublesome' concepts. The reflective workbench would then serve as a repository for a dedicated dataset to help validate Hodges' model (Do users apply Hodges' model in a consistent way?). In addition, an idealised objective would be for the model to facilitate the user's sense, awareness, learning of values through Hodges' model (discursive) and how their beliefs and attitudes develop (integrative, boundedness, reconstitutive) through their student career (transformative, liminality).
Hodges' model allied with TCs as explored here can help learners achieve a conceptual gestalt. The approach outlined here appears to be sympathetic to research and researchers. Hodges' model might provide a pathway to and a measure of holistic care, especially when care concepts are truly integrated. An online definition of ‘gestalt’ reads: “an organized whole that is perceived as more than the sum of its parts”. In so much of what we do in health and social care, such as person-centred and integrated care, this definition applies to not only the health of the individual, but global health and development too.
REFERÊNCIAS
1. The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions. Higgins JPT, Green S. editors. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. 2011. Available from: http://handbook.cochrane.org [ Links ]
2. Alligood MR. Nursing Theorists and Their Work. 8th ed. St Louis, MO: Mosby Inc. 2014. [ Links ]
3. Hodges BE. The Health Career Model. In: Hinchcliffe SM, (Ed.) Nursing Practice and Health Care. 1st Edition only, London, Edward Arnold. 1989. [ Links ]
4. Millard C, Wessely S. Parity of esteem between mental and physical health. BMJ, 2014; 349: g6821. https://doi.org/10.1136/bmj.g6821 [ Links ]
5. National Institute for Health and Care Excellence (NICE). Patient experience in adult NHS services (NICE clinical guidance 138) recommendation 1.5.10. London: NICE. 2012. Available at: https://www.nice.org.uk/guidance/cg138 [Accessed: 17/07/2017]. [ Links ]
6. Beta G, Lidaka A. The Aspect of Proficiency in the Theoretical Overview of Pedagogical Practice of Nurses. Procedia - Social and Behavioral Sciences. 2015; 174: 1957-65. https://doi.org/10.1016/j.sbspro.2015.01.861 [ Links ]
7. Mitchell G. Implications of Holding Ideas of Evidence-Based Practice in Nursing. Nursing Science Quarterly. 2013; 26(2): 143-51. https://doi.org/10.1177/0894318413477139 [ Links ]
8. Han LD, Ko SS, Gu Z, Jeong MK. Adaptive weigh-in-motion algorithms for truck weight enforcement. Transportation Research Part C: Emerging Technologies. 2012; 24: 256-69. https://doi.org/10.1016/j.trc.2012.01.010 [ Links ]
9. Crump KS. Use of threshold and mode of action in risk assessment. Critical Reviews in Toxicology. 2011; 41(8): 637-50. https://dx.doi.org/10.3109/10408444.2011.566258 [ Links ]
10. Taylor C. Threshold Concepts in Biology (Chap. 6) In: Overcoming barriers to student understanding: threshold concepts and troublesome knowledge. Meyer J, Land R. (Editors). Abingdon: Routledge. 2006. [ Links ]
11. Land R, Meyer J, Smith J. Threshold concepts within the disciplines (Educational futures; 16). Rotterdam: Sense. 2008. [ Links ]
12. Lane N. The Vital Question. Why is life the way it is? London: WW Norton; 2015. [ Links ]
13. Bledsoe BP, Watson CC. Logistic analysis of channel pattern thresholds: Meandering, braiding, and incising. Geomorphology. 2001; 38(3): 281-300. https://doi.org/10.1016/S0169-555X(00)00099-4 [ Links ]
14. Colman AM. A Dictionary of Psychology. Third edition. Oxford: OUP. 2009. p. 3. http://dx.doi:10.1093/acref/9780199534067.001.0001 [ Links ]
15. Clouder L. Caring as a ‘threshold concept’: transforming students in higher education into health (care) professionals. Teaching in Higher Education. 2005; 10(4): 505-17. http://dx.doi.org/10.1080/13562510500239141 [ Links ]
16. Batelaan N, Graaf R, Van AB, Vollebergh W, Beekman A. Thresholds for health and thresholds for illness: panic disorder versus subthreshold panic disorder. Psychological Medicine. 2007; 37(2): 247-56. http://dx.doi:10.1017/S0033291706009007 [ Links ]
17. Bridson JM, Prescott D, Guha A, Strivens J, Taylor D. Implementation of Critical Threshold Concept in Clinical Transplantation: A New Horizon in Distance Learning. World Journal of Educational Research. 2017; 4(2): 301-12. http://dx.doi.org/10.22158/wjer.v4n2p301 [ Links ]
18. Nambiar-Greenwood G. The role of mental health as a “threshold concept” for promoting patient-centred care for inter-professional health students. The Journal of Mental Health Training, Education and Practice. 2010; 5(4): 12-7. https://doi.org/10.5042/jmhtep.2010.0686 [ Links ]
19. Morgan H. The Social Model of Disability as a Threshold Concept: Troublesome Knowledge and Liminal Spaces in Social Work Education. Social Work Education. 2012; 31(2): 215-26. http://dx.doi.org/10.1080/02615479.2012.644964 [ Links ]
20. Stacey G, Stickley T. Recovery as a threshold concept in mental health nurse education. Nurse Education Today. 2012; 32(5): 534-39. http://dx.doi.org/10.1016/j.nedt.2012.01.013 [ Links ]
Received: August 07, 2017; Accepted: August 16, 2017
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
