











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Agenesis of the gallbladder is the least frequent malformation of the bile duct, with a variable incidence between 0.01 and 0.06%, according to the literature, although it may be lower, with a ratio women to men of 3:1 1. This condition was first described by Lemery in 1701, although other authors cite Bergman in 1702 as the first 2. The literature shows about 400 case series in total, which is why this case and literature review are relevant.
Agenesis of the gallbladder is not an isolated malformation, since studies show great association with other cardiovascular, genitourinary and central nervous system conditions in up to 15-33% of the cases, specifically pulmonary agenesis, tetralogy of Fallot, and anomalies in the limbs and in the genitourinary tract 1,3-6.
Most case series have been presented by Kumar, who classifies patients with agenesis of the gallbladder into three groups: a) asymptomatic patients (35%) diagnosed after performing studies to establish another cause; b) symptomatic patients (50%), of which 33% have a dilated primary bile duct and 33% lithiasis in the main bile duct, and c) children with more complex congenital anomalies (15%) such as lung agenesis, tetralogy of Fallot, and abnormalities of the limbs or the genitourinary system, which are often incompatible with life 7.
Moreover, if information relates only to symptomatic gastrointestinal cases, the statistics become more revealing, since 34% of them present with acid-peptic disease, and 50% are symptomatic with respect to pathology of the bile duct 7. Additionally, if only patients with biliary tract symptoms are considered, 33% present with dilation of the bile duct and 33% with choledocholithiasis, while the remaining cases report sphincter of Oddi dysfunction. With this in mind, it is possible to conclude that vesicular agenesis is a risk factor for such pathologies, as some authors have suggested 1,6-9.
CASE PRESENTATION
44-year-old woman from Bogotá D.C., mestizo, who was initially treated in the outpatient clinic for pain in the epigastrium and in the right hypochondrium, exacerbated by the intake of fatty foods, with approximately one year of evolution The symptoms led to conclude a clinical picture suggestive of vesicular lithiasic pathology, so an ambulatory ultrasound was performed, showing no gallbladder, an intrahepatic and extrahepatic bile duct of normal caliber, and a 6 mm common bile duct. A subsequent esophagogastroduodenoscopy discarded acid-peptic disease, so a magnetic resonance cholangiography (MRC) was requested.
Two weeks after the initial consultation, the patient was admitted to the emergency department due to a clinical picture of three days of evolution consisting of abdominal pain in the epigastrium, which radiated to the back, and subjective fever. No emesis nor irritating urinary symptoms were observed, but choluria without acholia.
The patient presented the following surgical history: tubal ligation and right hip osteotomy. Upon physical examination, mild jaundice and pain were observed in the right hypochondrium and the epigastrium, without a positive Murphy sign nor signs of peritoneal irritation.
Paraclinical tests yielded the following results: leukocytes: 13 395, N% 87; Hb: 14; platelets: 344 000; amylase 34 U/L; total bilirubin: 4.66 mg/dL; direct bilirubin: 4.09 mg/ dL; indirect bilirubin: 0.57 mg/dL; alkaline phosphatase: 1292 IU/L.
For its part, MRC showed generalized dilation of the intrahepatic and extrahepatic bile ducts, common bile duct with an average dilatation of 1 cm, with presence of hyperintense faceted images in T2. Gallbladder was not identified (Figure 1).
Source: Own elaboration based on the data obtained during the study.
Figure 1 MRC - 3D reconstruction of the coronal section in the bile duct. Note the absence of gallbladder.
Since several aspects indicated a high probability of choledocholithiasis, an endoscopic retrograde pancreatic cholangiopancreatography (ERCP) was performed, revealing a dilated, tortuous, and impacted intrahepatic bile duct, with no possibility of extraction, therefore, placing a stent was decided. Consequently, the case was taken to a surgical board to perform laparoscopic bile duct exploration.
During the procedure, the following findings were observed: absence of gallbladder, edematous biliary tract with duodenum adhesion, iatrogenic duodenum lesion of 5 mm (during the release of adhesions) and choledocholithiasis.
The procedure was performed by plastron adhesiolysis, primary duodenorrhaphy with absorbable suture by laparoscopy, and bile duct exploration by laparoscopy plus mechanical lithotripsy.
In the postoperative period, the patient presented a good evolution, with normalization of the liver profile and successful discharge after five days. Ambulatory follow-up showed an asymptomatic patient, without episodes of choluria, acholia or pain, so it was concluded that pain was completely resolved. Likewise, the patient showed tolerance to food; however, the patient did not attend subsequent follow-up sessions.
DISCUSSION
Agenesis of the gallbladder is a rare pathology that not many surgeons have the opportunity to treat. However, a surgeon must be prepared for any malformation and anatomical variant; actually, Skandalakis 10 points out vesicular triplication, which includes, agenesis of the gallbladder and how to act when it is suspected.
It should be noted that before 1950, ultrasound studies were not available, so cholelithiasis was diagnosed when oral cholecystography showed that the gallbladder was excluded (it was not observed in radiological images). When the patient underwent cholecystectomy, surgeons were surprised to notice the absence of the gallbladder.
Fortunately, today surgeons can plan procedures in an optimal manner, since ultrasound has a performance close to 80 or 90%, and is sufficient in most cases. However, in a case such as the one presented here, in which a scleroatrophic vesicle, chronic cholecystitis and acalculous cholecystitis were identified - the latter using tomographic studies-, agenesis of the gallbladder cannot be disregarded. In these cases, other specialized methods such as MRC (Figure 2), endoscopic ultrasonography, ERCP, among others, can be helpful. 9.

Source: Own elaboration based on the data obtained in the study.
Figure 2 MRC sequence in T2 of the bile duct. Note the absence of gallbladder.
Before ultrasounds, Frey performed the largest amount of surgeries involving vesicular agenesis, establishing a triad for its diagnosis under the following criteria: absence of inflammatory signs or fibrosis in the vesicular bed, complete dissection looking for an ectopic gallbladder (this dissection was extensive, including dissection of the left hypochondrium), and intraoperative cholangiography 6.
However, this procedure was done before the laparoscopic era and the arrival of MRC. Therefore, today it is considered that, during the surgical act, fibrous remnant or scar should be sought; the vesicular ectopic position should be discarded (intrahepatic, adhered to the left lobe, falciform ligament, retroperitoneal or in the anterior abdominal wall), and, according to the ability or criterion of the surgeon, intraoperative cholangiography should be performed, although it is not mandatory, as stated by Frey 11.
However, despite the fact that postoperative ERCP/MRC should inevitably be performed, in this case, MRC should always be considered, since agenesis is an exotic pathology and the infrequent vesicular positions mentioned above can be overlooked 3-5,7-14, thus avoiding, in the first instance, the risks of ERCP when there is no lithiasis in the primary bile duct (choledocholithiasis) (Figure 3). However, in the presence of agenesis, ERCP has been reported as not effective due, in part, to dysfunction of the sphincter of Oddi, so many patients need surgery and lithotripsy, as happened in this case 15.

Source: Own elaboration based on the data obtained in the study.
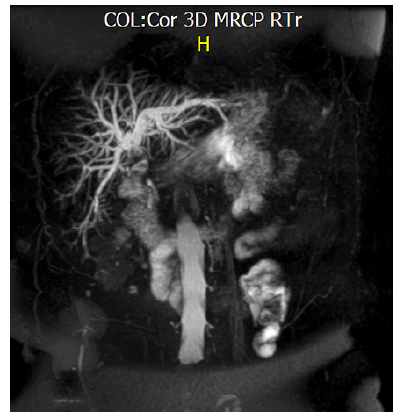
Figure 3 3D reconstruction of the bile duct. Note the multiple hyperintense images, the major ones (yellow arrow) correspond to lithiasis of the bile duct.
Finally, the safety vision of Strasberg 16 is recommended, since it is the most effective way to prevent bile duct injury as exposed in said reference.
Unfortunately, longterm follow-up was not possible, since the patient, as mentioned before, did not attend the subsequent controls, which is common in the Colombian context.
CONCLUSIONS
Although it is not possible to make generalizations based on the current evidence, other authors report two more cases in the region 17; therefore, the following steps are advisable when the intraoperative gallbladder cannot be identified:

