











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Globally, cervical uterine (CU) cancer constitutes a public health problem, given that it causes 528 000 new cases and 270,000 deaths per year, with 85% of these occurring in developing countries.1 In the last 30 years, incidence and mortality rates due to this type of cancer has diminished because social and economic indicators have improved. This change is due in great part to the implementation of secondary prevention efforts regarding early diagnosis and treatment of cancer precursor lesions during early stages.2 According to the Pan-American Health Organization in 2012, over 83 000 women were diagnosed with the disease and almost 36,000 died due to this cause in the Americas; adding that if current trends are manifested, the number of deaths will increase by 45% by 2030. According to the same source, mortality rates are three times higher in Latin America and the Caribbean than in North America, revealing huge inequalities in health.3
In 2009, Mexico reported a mortality rate due to CU cancer of 9.1 cases per 100 000 women and the state of San Luis Potosí reported 10.1 cases per 100 000 women.4 In this country, although screening is generally done by using the Papanicolaou test (cervical cytology or PAP), it is recognized that the effectiveness of the program on Timely Detection of Cervical Uterine Cancer has been poor. (5 A critical element that explains the low impact of the program on mortality due to CU cancer in most Latin American countries is the dissociation between the screening and treatment activities,6) with one of the critical factors being the quality of the samples for screening due, among others, to lack of compliance with the guidelines established in the cytology and pathology manual regarding the revision of the cyto-colpo-histopathological congruence, forms of training, and quality control, as well as personnel deficiencies in sample collection.7) A recent Mexican study8 showed that an important difficulty in the person collecting the sample is ignorance of the anatomy of the female lower genital tract, specifically the localization of the endocervix, the transformation zone, and lack of knowledge on which cells make up the transformation zone. Other faults were observed on the type of recommendations given to the user, the registry - particularly in identifying risk factors, and the gynecological evaluation before and during the test, as well as in applying the central technique (collecting the sample, spreading, and fixation).
The aforementioned justifies the need to conduct studies on educational interventions to improve the quality of sample collection from the cervical cytology. Students and interns (nursing staff engaged in social service) from the Nursing Degree Program in Mexico undertake their practices in public institutions. These practices include taking cervical cytology tests; hence, it is fundamental to improve capacities in this regard since their attendance to the university, which will increase their knowledge and skills as health service providers. Thus, the aim of this study was to evaluate the impact of applying a learning strategy to improve sample quality in cervical screening by the nursing staff in social service.
Methods
The study design was quasi-experimental, longitudinal and prospective, conducted in a university health center at a public university from February to June 2015. Convenience sampling was carried out of the institution where the study took place, with participation from 23 individuals who were about to complete their social service and required training in taking cervical cytology tests prior to concluding that stage. An educational intervention was designed based on the Andromache model for teaching innovation in taking these cytology tests, registered in the National Copyright Institute, dependent on the Mexican Secretary of Public Education (INDAUTOR, registry number: 03-2014-020412513001-01), and which was designed by researchers in the Faculty of Nursing at Universidad Autónoma de San Luis Potosí, Mexico. The intervention lasted two weeks with a total of 48 h, 24 h per week and was divided into three phases: 1- basal measurement, 2- training, and 3 -final measurement.
The first phase that conducted the basal measurement lasted 8 h, considered for the study as the pre-intervention and it assessed knowledge on taking cervical cytology tests and the skill in its execution. To apply the intervention, personnel participated from Pathology, Nursing, Gynecology, specialists in public health and information technology, all trained and certified in their given area. Three instruments were used: a test to measure knowledge and two verification lists, one to evaluate skills in taking cytology tests and another to emit the report of the quality of the cervical cytology samples. Knowledge was measured by applying a structured survey with 57 items (scale from 0 - 57 points, starting from the Mexican official norm), which has four sections: personal data (6 items), Mexican Official Norm (NOM-014-SSA2-1994. Secretary of Health, Mexico) (four items); anatomy of the female lower genital tract (six items); and steps of the procedure to take cervical cytology tests (47 items).
To obtain the score in practical skills, a verification list was designed with a measurement scale from 0 to 126 points, with three codes to evaluate in the procedure to take the cervical cytology tests: 0 (not taken), 1 (partially taken), and 2 (taken). It has five sections: reception of the user (3 items), registries (23 items), preparation of material (2 items), preparation of the user (8 items), and screening technique (27 items). The highest score is 126 for the person who throughout the procedure obtained two points for each item. Quality of the cytology tests was obtained through the report from the pathologist who was considered the gold standard. This study catalogued as suitable those samples with endocervical cells. The results were reported in a verification list based on the Bethesda System 2001, which classifies the sample as suitable or unsuitable (Table 1).9)

Instrument reliability was measured through Cronbach’s alpha (0.74 for the survey and 0.80 for the verification lists); experts on the topic provided validity.
The second phase corresponds to the training carried out during 32 h, 8 h per day. In this phase, theoretical classes (10 h) were dictated along with the practices (22 h). The theory was taught by professors, physicians, and researchers who were experts on the topic, using reading material, videos on the correct taking of cervical cytology tests, systematization of experiences to obtain facilitators and hindrances from the opinions of the participants and based on their experience, didactic techniques, like plenary talks, expositions and demonstrations, such as the technique to carry out the staining train and the importance of correct sample taking. The core of this educational strategy is the practice phase, which applied innovative methodological strategies to propitiate a more significant learning environment. Among these is the in vivo reading of the cervical cytology samples, which means that once the participants collected the samples, the staining was done in the place where the course was being offered. Thereafter, during a special session, by using a microscope, the pathologist reads and interprets the samples in front of the participants. The pathologist interprets each sample and communicates to individuals the quality with which it was collected, indicating if the sample contains endocervical cells and emitting the diagnosis. To perform said activity, four real-situation practices were carried out with patients. The first is cataloged as the basal measurement or pre-intervention and the last as post-intervention, which were taken to make the final comparisons of this study. Additionally, two other intermediate practices were conducted, denominated 360-degree practices and pre-final evaluation. The first makes a paired assessment (two participants, one conducts the technique and the other evaluates it), this is done to reinforce learning. In addition, an evaluator or certified monitor is present and is always in the consultation rooms to assess the procedure.
The pre-final evaluation practice is considered the last opportunity to carry out the technique of taking the guided cervical cytology tests and with help from experts before the final evaluation. All the samples were collected with cyto-brush for endocervix and Ayre spatula for exocervix. The registry used a format denominated “Request and Results of Cervical Cytology” from the Secretary of Health in San Luis Potosí, Mexico. Other practices exist, like simulation and modelling. The first simulates taking cervical cytology tests by using lower mammal anatomical pieces (cow uterus) with simulator cytological models of flexible material with which students can improve their skills. Modelling is a workshop in which the participants use special soap to model their anatomical pieces (uterus and cervix) with which they perform the three central steps of this procedure: cell collection, spreading the cells on the sample holder, and fixation. Expert professors guide the practices at all times.
The final measurement (8 h) constitutes the last phase and, for this study, it is called post-intervention, which again and for the last time evaluated knowledge and practical skills. To analyze results related to knowledge and practical skills, Student’s t and the analysis of variance with repeated measures were applied. Analysis of the results of sample quality was done by using the binomial test.
This study kept in mind the ethical principles contained in the Helsinki declaration. All the participants and patients provided written informed consent. The Ethics Committee of the Faculty of Nursing and Nutrition at Universidad Autónoma de San Luis Potosí approved the project and assigned registry number CEIFE-2015-118. The diagnosis of the samples and their quality were validated through the Department of Pathology at Hospital Central Dr. Ignacio Morones Prieto located in the city of San Luis Potosí. All the results were delivered to the patients one month after performing the cytology study.
Results
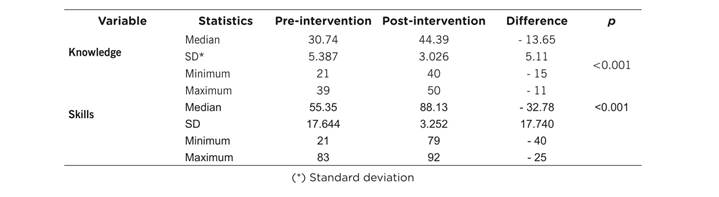
This study showed in the participants a significant increase from the basal measurement to the final measurement in the average scores of theoretical knowledge (30.74 to 44.3 points) and in practical skills in taking cervical cytology tests (55.3 to 88.13 points) (Table 2).
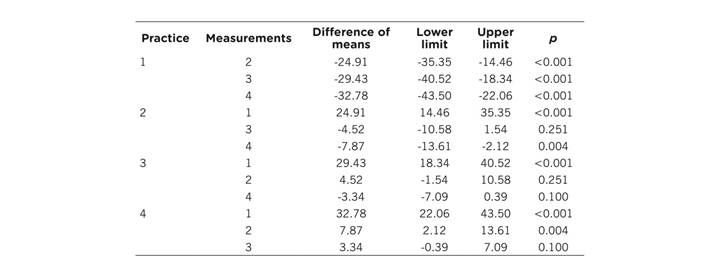
A sustained increase was noted in the average score of practical skills measured during four sessions of the intervention (1st = 55.34, 2nd = 80.26, 3rd = 84.78, and 4th = 88.13), showing in the ANOVA that differences were statistically significant only between the first and the remaining three (Table 3).
Table 3 Results of the ANOVA of repeated measurements of the comparison of skills among practice sessions (n = 23)
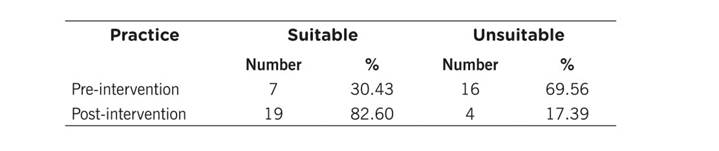
The pre-intervention reported 30.43% suitable samples versus 82.6% in the post-intervention; this difference was statistically significant (p = <0.001) (Table 4).
Discussion
This study revealed that in the basal measurement participants obtained a low score with respect to the expected score. This result agrees with that reported by Songthap et al.,10Arias et al.,11 and Makwe et al.,12 who found that students demonstrated medium knowledge on CU cancer, given that they lacked sufficient clarity on the theme. Weaknesses found in this study regarding the low knowledge of the participants is related to the results of the samples in function of the quality reported through pathology because the first measurement only obtained 30.43% of samples with optimal quality and with the presence of endocervical cells. This result is similar to that reported by Yoshino et al.,13 whose work with nurses from a university in Japan indicates that only 4.7% knew that CU cancer is detected through tests, like the Papanicolaou test, and concludes that deficient knowledge in this staff was associated with the failure to undergo cancer detection. Likewise, the study by Ali et al.,14 2010, with interns in social service and nursing staff from a tier III hospital in Karachi, Pakistan, also indicates that only 23.3% were aware that CU cancer is the most common cause among gynecological cancers and 41% ignored the new detection methods; concluding that most service providers do not have sufficient knowledge on this ailment.
During post-intervention, the participants improved notably in knowledge acquisition and improved their practical skills, gained greater confidence, and the guidance provided to users was better. In this evaluation, the mean score in practical skills improved compared to the first measurement in the five sections assessed (from 55.35 to 88.13 points). This result was reflected in the pathology report during the post-intervention, given that it reported 80% suitable samples, with useful material for its interpretation, which was the main objective in this study. This agrees with the results by Gómez et al.,15 where after an educational intervention to improve the taking of cervical cytology tests, it reported a greater amount of cervical material useful to emit results that are more accurate and diminish false negatives.
Training with this innovative methodology is effective to increase the capacities of participants, as well as to improve the quality of the samples from cervical cytology tests, given that this training has implemented strategies different from the habitual strategies. Nevertheless, it is fundamental to continue improving the teaching methodologies in students and health professionals. It is important to reinforce general learning in taking cervical cytology tests in the following aspects: awareness of the anatomical characteristics of a cervix, the way of conducting the gynecological assessment, different instruments used to collect samples, and the correct fixation technique.
One of the limitations in this study was the availability of educational and health institutions to allow their interns in social service to attend the training. We recommend increasing the number of participants in applying this methodology, as well as measuring the variables one or six months after the training concludes. We also recommend using this model in other intervention scenarios and testing new “be learning”-type tools to implement the advanced technology in health education.
In conclusion, interns in social service have among their functions that of providing care in public health services, and to a large extent, performing cervical screening, which is why it is fundamental for them to have solid theoretical and practical training that integrates the capacities and skills requested by the labor setting. Thus, upon increasing their technical skills and knowledge on cervical cancer, they will enhance their practice along with the quality of public services. This study identified the importance of continuous training of the health staff in formation, given that during their attendance in the university, they acquire the necessary theoretical knowledge, but often practice is minimal in relation to the opportunities of direct care to patients. The results from this study evidence the need to implement continuous training and updating of the health staff, as indicated in the NOM-014-SSA2-1994 standard, for prevention, detection, diagnosis, treatment, control, and epidemiological surveillance of cervical-uterine cancer, as well as by the Action Program on Cervical Cancer in Mexico 2007-2012.

