











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
With the creation of the Brazilian Unified Health System (Sistema Único de Saúde Brasileiro - SUS), the National Policy for Comprehensive Women’s Healthcare 1 was established in 2004, followed by the Stork Network (Rede Cegonha) in 2021, which gradually promotes best obstetric practices and maternal and child health. Among the various concepts that comprise the expression “best obstetric practices” is the singular reception of the pregnant woman in the healthcare service, in addition to emotional support, well-being, and pain relief, which are based on non-pharmacological methods 2.
Maternal and child health has been a recurrent subject both nationally and internationally. The World Health Organization has taken an important initiative, which aims, among others, to reduce maternal and newborn mortality through strategies that promote timely access to healthcare services for pregnant women. In this line, countries, in general, have made investigative and assistance efforts to identify the best scientific evidence in maternal and child health 3.
Following Brazil’s example, Cuba and the Dominican Republic, along with other countries, have invested in new management and intervention approaches to promote the comprehensive health of women and children. The objective is, under this scope, to prospect strategies that ensure family planning, qualified prenatal care in primary healthcare, vaccination coverage, and universal access for pregnant women and children 4,5.
Based on these developments, the best maternal and child health practices transcend mechanized interventions and enable comprehensive and integrative care. Based on this initiative, best practices are open to more than just a professional subject or a single sector. They are configured as a healthcare network that expands and converges with diverse social sectors 6.
Studies confirm the importance of access and qualified information in prenatal care to empower pregnant women concerning their rights, thereby contributing to their greater autonomy and leading role during labor and delivery. The sustainable development goals, especially those related to reducing maternal, newborn, and infant mortality, can be achieved through collective and collegiate efforts among the various actors involved 7,8.
It is noted that maternal and child health in Brazil has undergone growing developments in its conception and (re)structuring to expand and improve the best multi-professional practices. Still, there are gaps in prenatal care regarding healthcare, infrastructure, health education, and a deficit of qualified professionals 9.
However, the question concerning healthcare professionals’ perspective of best practices in maternal and child health remains. In this sense, this study aimed to understand the perspective of healthcare professionals regarding best practices in maternal and child health.
Materials and methods
This research is a qualitative, exploratory, and descriptive study. The data collection was carried out online between December 2020 and March 2021. The study corpus consisted of 23 healthcare professionals out of the 33 appointed by the 4th Regional Health Department in Rio Grande do Sul for their strategic role in the 33 cities covered by the 4th Department. The objective of the regional health departments is to integrate the organization, planning, and execution of healthcare activities and services.
Notably, among the professionals appointed by the 4th Regional Health Department, 40 % had just a college education. The others had specializations and master’s degrees in maternal and child health. However, they all work in management activities and maternal and child healthcare. Based on the nominated individuals, we considered as an inclusion criterion being willing and available to participate voluntarily in the study and, as an exclusion criterion, to be healthcare professionals on leave of absence for a justified reason.
The data collection instrument was a semi-structured Google Forms questionnaire sent by e-mail along with the informed consent form to the professionals who had previously volunteered to participate in the study. The questionnaire contained questions regarding best practices in maternal and child health and aspects of the maternal and child healthcare network, such as what they know about best practices in maternal and child health and how they encourage such practices; which aspects should be considered in the management of the maternal and child healthcare network, and how to qualify the access to the maternal and child healthcare network.
Minayo’s thematic content analysis technique was used for data analysis, which was systematized in three stages. The first stage, named “pre-analysis,” consisted of resuming the initial hypotheses and objectives to direct data deepening. The second stage consisted of exploring the material. The texts were analyzed systematically, generating the initial thematic categories. The third stage comprised the treatment of results, i.e., the inference, interpretation, and final delimitation of thematic categories 10.
Throughout the research process, the recommendations of Resolution 466/2012 by the National Health Council (Conselho Nacional de Saúde) 11 and the Circular Letter (Ofício Circular) 2/2021 regarding research in the online modality 12 were followed. The Research Ethics Committee of the Universidade Franciscana approved the research project under Legal Opinion 4.253.922. To ensure anonymity, the participants’ statements were identified throughout the text with the letters “HP,” standing for healthcare professionals, followed by a number corresponding to the order of the statements: HP1… HP23. This study decided not to differentiate nurses from medical doctors, as it was understood that the Stork Network focuses on multi-professional practices.
Results
Of the 23 study participants, 19 are nurses, and four are medical doctors working in Basic Health Units (Unidades Básicas de Saúde - UBS) and residents of the central region of Rio Grande do Sul, southern Brazil. The analyzed data allowed the delimitation of two thematic categories: “best practices in maternal and child health: strategies in providing care” and “strategies to qualify the maternal and child healthcare network.”
Best practices in maternal and child health: strategies in providing care
It was evident that the interviewees recognized that best practices in maternal and child health consist of measures identified as the best practices to be adopted in the mother-baby binomial. The participants’ reports demonstrate that best practices are understood as strategies that provide safety, quality, protection, and humanization throughout the pregnancy-puerperal process. They also highlight that such methods are based on scientific evidence and aim to reduce maternal and neonatal mortality, as described:
Humanization in the care provided aiming to follow evidence-based practices and providing knowledge, safety, and comprehensive care. (HP1)
Dissemination of knowledge and improvement strategies for the clinical/therapeutic care provided to the mother-baby binomial. (HP2)
These are practices based on scientific evidence to reduce maternal and infant mortality. (HP16)
It was noted in the participants’ statements that the best practices in maternal and child health are introduced from family planning so that women can become familiar with and choose contraceptive methods based on their health and that of their families. The participants recognize that this previous programming enables the qualification of comprehensive healthcare.
Best practices include family planning, orientation on contraceptive methods use, and access to quality prenatal care. (HP9)
Family planning can qualify for healthcare. (HP12)
Welcoming them with active listening and providing access to contraceptive methods and pregnancy testing. (HP21)
It was found in the participants’ statements that the best practices used in the daily routine of healthcare services are related to non-pharmacological methods for pain relief during labor, such as warm baths, the Swiss ball, music therapy, and penumbra. Some also mentioned the “golden hour,” which is considered the first hour of the newborn’s life and, in this sense, stressed the importance of breastfeeding, skin-to-skin contact, and timely clamping of the umbilical cord.
I consider warm baths, walking, Swiss ball, squatting, and skin-to-skin contact paramount. (HP3)
Non-pharmacological pain relief methods are essential, such as warm baths, Swiss ball, ambulation, company, timely cord clamping, skin-to-skin contact, and breastfeeding within one hour of life. (HP5)
I emphasize non-pharmacological methods of labor pain relief, reducing the number of episiotomies. (HP6)
Patient care provided by a multi-professional team, company, non-invasive practices for pain relief, and the golden hour. (HP17)
Free demand breastfeeding, encouraging breastfeeding and a good latch, and humanization. (HP18)
In the participants’ understanding, healthcare professionals responsible for maternal and child healthcare should consider women’s empowerment, rights, and duties. They address the importance of the companion of choice throughout the pregnancy- puerperal journey to allow the singularity and multidimensionality of care throughout the process.
I understand that respecting women’s decisions is necessary to empower them regarding their delivery and puerperium. (HP1)
Access to quality and humanized prenatal care with the support of a companion throughout the process must be considered. (HP14)
The right to a companion during childbirth. (HP23)
The professionals must be receptive to clarifying women’s doubts, enabling decision-making, and empowering them as protagonists of their care. (HP22)
The participants’ understanding of the best maternal and child health practices is summarized in humanized, integrative, and resolutive practices throughout the healthcare network. This qualification process, however, is gradual and must be carried out by each healthcare professional.
Strategies to qualify the maternal and child healthcare network
Strategies to qualify the maternal and child healthcare network have been increasingly promoted in Brazil. In this line, the participants highlighted the promotion of continuing education as lifelong training. It is from spaces of integration and (re)signification of knowledge and practices among co-workers that the needs and demands of each service are discussed, as described by a participant:
Through continuing education in network services, dialogue, and knowledge sharing, we can identify the demands and (re)signify our practice. (HP22)
The participants’ reports indicate that the qualification of the healthcare network is achieved through dialogical and constructivist processes mediated by continuing education. From this perspective, some participants highlighted the horizontality of interprofessional relationships and the permanent dialogue between the various actors of the healthcare network.
We need to keep qualifying the interprofessional dialogue... the professionals’ continued training in an integrated set; it is something that would certainly lead to better quality care provided to pregnant and postpartum women. (HP13)
Meetings with the network professionals for dialogue and agreement on the initiatives to be developed. (HP19)
The participants emphasize early admission of pregnant women to healthcare services to identify their needs and expand the support network. They underline, from this perspective, the relevance of prenatal care to promote early bonding and ensure a safe and continued pregnancy throughout the pregnancy-puerperal period, as noted in the following statements:
I focus on prenatal care. Active search, hospitality, and the follow-up of postpartum and puerperium. (HP7)
To welcome women in the UBS with suspected pregnancy, providing all the care for the beginning of prenatal care, such as exams and orientations related to care and assistance. (HP9)
Performing a comparative survey of the number of puerperal women discharged from the hospital with the number of first puerperal and Child Health appointments. (HP10)
Qualifying the care provided to pregnant women, puerperal women, and children should be considered a priority to prevent maternal and infant morbidity and mortality. (HP11)
For the participants, the bond between professionals and pregnant women is established through active and dialogical participation. This bond is, however, hindered by the high turnover of professionals in healthcare units. Besides the bond, hospitality with active listening, ambiance, and expanded and resolutive care were mentioned.
I always advocate hospitality with active listening, health education, screening pregnant women and their families, and establishing a professional-user bond. (HP7)
Try to keep professionals in primary care and encourage people to stay because turnover is high. (HP8)
Measures that encourage personnel to reduce turnover. (HP15)
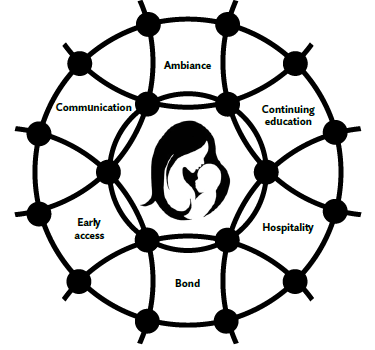
The qualifying strategies of the maternal and child healthcare network are configured in the participants’ conception of soft technologies, which are expanded and consolidated from the interprofessional relationships. In this sense, continuing education, hospitality, ambiance, active listening, early access, and the professional-user bond are strategies that, summarized in Figure 1, prospectively contribute to the qualification of the maternal and child healthcare network.
Discussion
The study participants consider themselves responsible for developing the best maternal and child health practices and for resolute and quality care. Studies corroborate these findings by mentioning that the staff is committed to implementing the best maternal and child health practices, which are guaranteed, especially by continuing education in health and lifelong training 13,14.
In this context, continuing education in health is understood as learning on the job, where learning and teaching are brought together in professional practices. Thus, this learning process appreciates the professionals’ pre-existing knowledge coordinated with daily challenges to improve their knowledge 15.
Adopting best practices focused on the maternal and child healthcare network entails a daily and permanent process through the stimulation of reflective and self-evaluative processes that promote prospective self-criticism. The reflective process, defined by knowledge associated with actions, demanding actions that transcend the linearity of the daily routine, must be stimulated in the development of theoretical-practical knowledge. In addition, alternative therapies should be discussed and encouraged, among which ambiance, music therapy, and aromatherapy stand out 16,17.
The ambiance is a physical space of interpersonal relationships that provides hospitality and humane care. The National Humanization Policy considers ambiance as a welcoming, integrating, and aggregating environment for best practices that aim to improve the work process 18.
For healthcare professionals, best maternal and child health practices are translated daily into relational-interprofessional and humanizing actions. In this sense, dialogic action-reflection-action is essential for redefinition practices and interprofessional conduct to ensure special and multidimensional care. Studies 19,20 emphasize, under this approach, the relevance of the co-responsible engagement of the various actors within the network to overcome hegemonic standards and enable horizontal and dialogical intervention processes.
According to the study participants, the best practices in maternal and child health, especially those related to soft technologies, enable greater dynamism and interprofessionalism. In this relationship, soft technologies emerge as enhancers of professional interactions and associations, strengthened by bonding and hospitality 21. According to the participants, these technologies must be expanded to enable greater interactivity in the maternal and child healthcare network. A study 22) corroborates this idea by mentioning that interactive and associative processes favor an ambiance that aggregates and enhances the autonomy of the various actors involved. In this dialogic path, it is also necessary to consider the active participation of companions as an empowering and bonding strategy 23,24.
Therefore, the need to strengthen interpersonal and interprofessional relationships from new theoretical and practical references emerges. A study indicates that professional qualification, from an interprofessional perspective, enables dialogical and associative breakthroughs between professionals, and pregnant and postpartum women, encouraging the development of best maternal and child health practices starting from prenatal care 25.
The participants stressed the relevance of strategies associated with active listening, dialogue, and the professional-user bond, which can be expanded and strengthened by the mediation of continuing education in health. Studies indicate that innovative approaches, that is, those that are dialogical and horizontalized, enable qualified and resolutive interventions in maternal and child health 26. In this context, continuing health education is enabled by developing spaces for critical-reflective approaches that induce the (re)significance of the professional daily existence and performance 27-30.
This study’s participants mentioned other strategies related to hospitality and supportive ambiance. They emphasize, in this sense, the importance of the parturient’s companion of choice, so that she feels welcomed and supported in her needs, is autonomous, and becomes the protagonist of the decision-making process. A study in this line has shown that hospitality, birth companion, and ambiance are vital for the quality of care provided to the parturient 31,32.
The qualifying strategies of the maternal and child healthcare network mentioned by the participants are within reach of healthcare professionals. They can be promoted, for the most part, without substantial structural investments. A study, however, opposes this argument by mentioning that structural and interpersonal assets must be considered in the management processes to enable qualified healthcare 33. Therefore, the importance of continuing education in health is emphasized, as it promotes the professionals’ qualification, contributing to improved care through hospitality, ambiance, and active listening.
Conclusions
Healthcare professionals acknowledge the relevance of best practices in maternal and child health, although this process needs to be expanded and consolidated. Continuing education, hospitality, ambiance, communication, early access, and the professional- user bond stand out among the qualifying strategies.
It is concluded, in summary, that the promotion of best practices in maternal and child health is related to more significant and better investments in human resources and a welcoming and aggregating ambiance. Therefore, the questions remain regarding how to qualify professional relationships and interactions to reassure the singularities of each user and what new theoretical-methodological approaches should be promoted to meet the unique health demands.
Study limitations
This study’s limitation is related to the low adherence of medical professionals, considering the 14 medical doctors previously referred by the 4th Regional Health Department. Another restraint may be associated with the exhaustion experienced by healthcare professionals due to the multiple and growing activities stemming from the pandemic.

