











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Thumb hypoplasia is a congenital abnormality that, according to the Blauth classification, can present with the complete absence of the thumb or different degrees of affectation ranging from type I to type V. This classification is useful as it not only describes the degree of hypoplasia but also guides treatment and prognosis.1
Thumb hypoplasia has an incidence ranging from 3.4 to 16 cases per 10 000 births and is often bilateral (2060% of cases) and accompanied by abnormalities in the limbs, spine, and other organs. This condition can occur within the VACTERL association, a group of birth defects that tend to co-occur and mainly affect parts of the body such as vertebrae, anal atresia, heart, trachea, esophagus, kidney, and limbs.2,3
The opposing movement of the thumb, which is particularly important for the correct functioning of the hand as it supports pincer grasp movements, is often affected in thumb hypoplasia due to atrophy or absence of the thenar muscles.
Abductor digiti minimi (ADM) transfer is a technique proposed by Eugen Huber in 1921 and used to restore the opposing movement of the thumb in patients with median nerve palsy.4 In theory, this method has advantages over other types of opposing transfers, since it replaces the intrinsic muscle of the deficient thumb with a muscle from the hypothenar region, which also helps to increase the volume and improve the appearance of the atrophied thenar eminence.5 This technique is often used in hypoplasia types II and type III.
Consequently, the aim of the present work was to describe the functional results obtained with the ADM transfer, also known as Huber transfer, in patients with thumb hypoplasia.
Materials and methods
This is a descriptive and retrospective observational study conducted in patients with thumb hypoplasia who underwent Huber opposition transfer to improve the function of their thumbs. Some of these patients had undergone pollicization because of the type of hypoplasia they presented.
The initial sample was composed of 14 patients with the same number of thumbs operated. However, patients that had undergone more surgeries to improve thumb opposition or other congenital malformations of the hand that altered its functionality and who could not be followed for at least 6 months or contacted for reassessment were excluded. The final sample consisted of 11 individuals.
The variables evaluated were age, sex, laterality, classification (according to Blauth), abnormalities of the contralateral thumb, additional surgeries, follow-up time, assessment of thumb opposition, and instability of the metacarpophalangeal (MCP) joint of the thumb.
Opposition of the thumb was evaluated based on a modification of the Kapandji index,6 a widely used instrument that assesses thumb opposition based on where on their hand the patient is able to touch with the tip of their thumb and that is very practical to implement in children; it should be noted that the original version of the instrument has a score from 1 to 10. In the modified version used for the present work, the values ranged from 0 to 4, and the equivalencies were very similar depending on the location reached by the tip of the thumb: 1 radial side of the middle phalanx of the index finger; 2 radial side of the distal phalanx of the index finger; 3 tip of the index finger; 4 tip of the little finger (only this value changed and is equivalent to Kapandji's score 6).
This is a retrospective study that did not require performing any new procedure on the participants. Participants' anonymity was kept at all times. The patients' data were obtained after their legal guardian signed an informed consent. This work was approved by the Ethics Committee of the Faculty of Medicine of the Universidad Nacional de Colombia through Minutes 010-159-18 of June 15, 2018, and followed the ethical principles for research on human beings established in the Declaration of Helsinki7 and Resolution 8430 of 1993 of the Ministry of Health of Colombia.8
Procedure
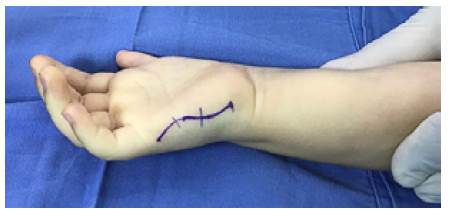
Figures 1, 2, and 3 show the details of the technique. A slightly curved incision was made over the ulnar edge of the hand, going from the base of the little finger to the pisiform bone. ADM was located and released from its insertion; the muscle was lifted, and its origin was left intact in the proximal side. On some occasions, it was possible to visualize the nerve branch of the ulnar nerve that enters deep into the base of the muscle.
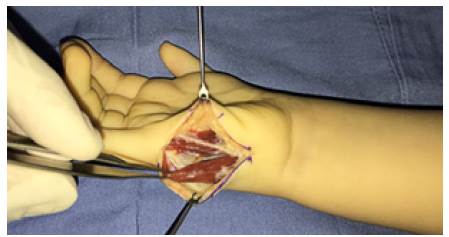
Source: Document obtained during the study.
Figure 2 Dissection of the abductor digiti minimi muscle

Figures 4 and 5 show the second incision made in the dorsal and radial side of the MCP joint of the thumb, which was used to create a subcutaneous tunnel, first with scissors and then with Kelly clamps. This tunnel ran from the origin of the ADM in the pisiform bone to the second incision in the MCP joint of the thumb; it had to be wide enough to allow adequate movement of the ADM over the superficial palmar fascia. The muscle was transferred through the tunnel to the second incision, and the insertion of the abductor pollicis brevis on the dorsum of the proximal phalanx of the thumb and the dorsal capsule of the MPC joint was sutured with 4/0 polypropylene. On several occasions, it was necessary to open the first web space and reconstruct the ulnar collateral ligament of the MPC joint because it was unstable.

Source: Document obtained during the study.
Figure 4 Transfer of the abductor digiti minimi muscle through a subcutaneous tunnel to the thumb.

Source: Document obtained during the study.
Figure 5 Suture of the abductor digiti minimi muscle at the insertion of the abductor pollicis brevis on the dorsum of the proximal phalanx of the thumb and the dorsal capsule of the metacarpophalangeal joint.
The average age of the patients analyzed at the time of surgery was 35 months (range 28-60 months), with a median of 30 months, and average follow-up time of 15.4 months (range 6-60 months); 54% of the patients were male. There were 3 cases of hypoplasia type II and 2 cases of hypoplasia type III; the other 6 cases had undergone pollicization. Moreover, 5 patients had undergone reconstruction of the MPC joint of the thumb, of which 2 presented with hypoplasia type IIIA and 3 with hypoplasia type II. Regarding laterality, 6 patients presented difficulty in the right hand and 5 in the left hand.
According to the modified Kapandji index, the average of the opposing function of the thumb before surgery was 1.63 (interval of 1-2), increasing to 3.72 (interval 2-4) after surgery. Figures 6 and 7 show the results for 2 patients.

Source: Document obtained during the study.
Figure 6 Pre-operative assessment (type I) and satisfactory post-operative outcome (type IV).

Source: Document obtained during the study.
Figure 7 Abductor digiti minimi transfer at 18 months with type IV result on modified Kapandji index. → Abductor digiti minimi in the thenar region.
In none of the cases there were any immediate postoperative complications or the need to perform additional surgical procedures.
Discussion
Thumb hypoplasia is a pathology that alters thumb function and, consequently, of the hand, as it hinders opposition and affects dexterity. Thumb hypoplasia type I, and sometimes type II, does not require any specific management, but hypoplasia type IIIA, and some type II cases, require surgical treatment to reconstruct the finger; some of these procedures are transfers to improve thumb opposition as the technique described by Huber. In type IIIB, IV, and V, pollicization is usually performed.9,10
The literature reports some studies that assess the Huber transfer method,11,12 but they do not have an adequate and objective evaluation of the results obtained in the procedures. Given the inherent difficulty of carrying out studies with young children, especially under the age of 3, assessment with the Kapandji index may not be possible, altering the evaluation. In these cases, making drawings or marking points so that the child can reach them with the thumb is recommended, and the help of the parents is necessary for achieving this.
The rotation of the ADM, which arises from the pisiform bone, can produce compression of the ulnar nerve, since the transferred muscle is located on the Guyon's canal. This finding, reported by Cawrse & Sammut,13 is known as a rare complication that forces the reversal of muscle transfer. For this reason, and in order to give greater length to the transferred muscle, some authors remove the proximal ADM muscle from the pisiform bone, the flexor retinaculum and the flexor carpi ulnaris.12-14 In the present series, this complication was not observed and neither was the transfer of the ADM as a myocutaneous flap,15,16 which is more useful in children with greater atrophy of the tissues in the thenar region.
The participants in the present study had good functional results with the Huber technique after their thumb-opposition function improved: in 9 patients, it increased to type IV and in another it went from I to III; only in 1 case it did not improve significantly (type I to II) because the patient had a stiffness of the fingers associated with a VAC-TERL. Finally, good stability of the MPC joint was achieved.
The small size of the sample was one of the limitations of the present study due to the type of pathology analyzed.
Conclusions
The findings prove that the Huber technique is an effective therapeutic option that has the advantage of using an intrinsic hand muscle with a similar function. It also guarantees a better aesthetic appearance by filling the thenar region and allows good functional opposition results for the hypoplastic thumb, which are very similar to those described with other techniques such as the flexor digitorum superficialis lasso tendon transfer.17

