











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
Guided by the principles of the Toronto Call to Action for a Decade of Human Resources in Health in the Americas (2006-2015),1 the World Health Organization (WHO), the Pan-American Health Organization (PAHO), and the Colombian Ministry of Health and Social Protection consider human talent as the pillars of the health system, highlighting the importance of competent and committed human resources working in optimal conditions to meet the health needs of the population.
Anesthetists are a key component of human talent in health. According to statistics of the Colombian Society of Anaesthesiology and Resuscitation (S.C.A.R.E) for 2016, 3206 anesthetists were members of S.C.A.R.E. and, in Colombia, close to 116 specialists graduate from the 23 programs that offer the specialty. The year 2016 was declared "The Year of Human Talent in Health,"2 underscoring the importance of knowing the characteristics and other determinants of human talent supply and demand in Colombia.
One of the objectives of the S.C.A.R.E Quality of Life Programme is to characterize Colombian anesthetists in terms of their personal, social, academic and work factors, as well as to inquire about health-related conditions and wellness (quality of life, family functionality, professional burnout, depression, anxiety, suicide, use of psychoactive substances), which might be directly or indirectly related to their personal or work situation.
Occupational stress has been identified as a relevant factor in the practice of anesthesiology. It is related to a noxious emotional response that occurs when work demands surpass the capabilities, resources and needs of the practitioner.3 Although stress is common in the workplace, anesthetists are particularly prone to chronic stress due to pressure, length of the workday, financial instability, and issues with interpersonal relations.4 The syndrome arising from these conditions is known as professional burnout and may lead to substance and alcohol abuse, family problems and emotional changes, putting the professional performance of the anesthetist at stake, increasing the risk of lawsuits, and compromising patient safety.5,6
On the other hand, recognizing factors such as training, work prospects and academic productivity of the anesthetists is of critical importance because it helps identify the areas of training already covered and the areas with potential for development. Likewise, knowledge of the academic prospects of the professionals allows to identify ongoing training which is key for maintaining quality standards; and finally, knowledge creation contributes to the advancement of the discipline and, consequently, it needs to be evaluated and promoted at a local level.3
Acknowledgement of work, personal and academic conditions will serve as the basis for the formulation by S.C.A.R.E of a plan of action for developing customized interventions.
The objective of this work was to describe the socio-demographic, academic and work characteristics of Colombian anesthetists, as well as the levels of satisfaction at work as an initial component of a project entitled "Health and well-being conditions related to the practice of anesthesia in Colombia." Details about the assessment of these other factors will be presented in separate publications.
Materials and methods
Sampling and sample size
Following approval by the institutional Ethics Committee, a convenience non-probabilistic sampling was used, including all the anesthetists in the S.C.A.R.E. database. A snowball sampling was used for the professionals in the databases of the society and of the departmental association leaders, as well as of attendance at national academic events, where the instrument was completed on site (XXXI Colombian Congress of Anaesthesiology and Resuscitation and I International Congress of Paediatric Anaesthesia).
Data collection
The data collection tool was designed and reviewed based on indicators collected by the S.C.A.R.E work observatory, trying to identify those characteristics with a high potential of impact on the health (occupational and mental) and academic development of the professionals. The tool was administered through interactive electronic media, ensuring anonymity of the information and data confidentiality, and this was clearly explained to the participants. Data collection took place between June and November 2015. Completion of the electronic data was verified in the final database. Each of the questions or sections was adjusted according to the number of respondents. In the end, a total of 662 forms were completed.
Data regarding the professional profile and personal characteristics were analyzed using descriptive statistics, frequency measurements such as proportions and 2 x 2 tables for categorical variables and their intersections, and means and medians for continuous variables with their respective scatter measurement (standard deviation [SD] or interquartile range [IQR]). Bivariate statistics were used for the analysis, using x2 or Fisher exact test and the Mann-Whitney U test for median differences. Income values were taken in Colombian pesos and converted to US dollars based on the average exchange rate for 2015.7) All analyses were conducted using the STATA 13 software package (Statacorp, Colege Station, TX).
Results
Sociodemographic characteristics
A total of 702 anesthetists responded some section of the survey. The majority were males (70%; n = 494), and the mean age was 45 ± 11 years. Table 1 shows the distribution by age groups.

In terms of the department of origin, there was a significant participation from Bogotá DC, followed by Antioquia, Valle del Cauca and Atlántico; while there was a marginal representation from Vichada, Guaviare, Casanare and San Andrés & Providencia. The majority of the respondents reported that they practiced in capital cities (89%; n = 628). In terms of marital status, the majority (62%) of the anesthetists were married, 22% were single and 11% reported a de facto marital union; 4% were divorced and 1% were widowed; and 81% have 2 or more children.
Overall, 82% (n = 566) of the anesthetists were home owners, and almost half of them were in the process of paying for their homes (55%).
Academic characteristics
Of the anesthetists who participated in the study, 47% (n = 326) had graduated from a public university in Colombia, while 39% (n = 275) had graduated from a private university; the remaining 14% (n = 101) had done their graduate training abroad.
Regarding time since graduating from the graduate program, 31% (n = 216) had less than 5 years of specialized practice, while 27% (n = 190) had more than 20 years of experience. Out of a total of 698 anesthetists, 89% reported that they would specialize in anesthesia again (86% of the women and 90% of the men; x2, P > 0.05), while 11% (n = 78) would not choose that specialty again. The reasons stated by the latter group included work overload (41%), compensation below their expectations (36%), complex work schedule (14%), and dissatisfaction with the profession (9%).
In terms of additional academic training, 20% (n = 143) of the anesthetists reported having some training in a second clinical specialty (17% of the women and 21% of the men; Fisher, P >0.05), the most common being cardiovascular anesthesia, intensive care, and pain (Table 2). Reports of a subspecialty were more frequent from anesthetists with more than 11 years of practice since graduating (Fisher, P <0.05).

On the other hand, 23% (n = 161) of the anesthetists had other academic degrees (24% of the women and 22% of the men; P > 0.05), including the following: management (n = 61), higher education teaching (n = 38), epidemiology (n = 16), auditing (n=15), and ethics (n=9). Less frequent was training in software development and information technology, legal liability, project management, engineering, finance, family medicine, pharmaceutical chemistry, public health, alternative medicine, and occupational health, among others.
In terms of foreign language proficiency, anesthetists had a greater mastery of English, French, and Portuguese. One-hundred percent reported some degree of knowledge of the English language, although only 12% were in an advanced level (Table 3). Other languages reported less frequently were Italian (n = 6), German (n = 5), Catalonian (n = 2), Russian (n = 2), Rumanian (n = 1), Mandarin (n = 1), Swedish (n = 1), Yiddish-Hebrew (n = 1), Latin (n = 1), Arabic (n = 1), and even indigenous dialects such as Wayunaiki (n = 1), with different levels of proficiency.

Regarding the number of hours/year devoted to continuing medical training, 18% of the anesthetists devoted less than 20 hours to this activity per year; 24% between 21 and 40 hours; 22% between 41 and 60hours; 13% between 61 and 80hours; 9% between 81 and 100hours; and 14% devoted more than 100h/year. There were no differences between men and women regarding the time devoted to training (x2, P >0.05). Approximately 10% of the anesthetists reported that they belonged to a research group recognized by Colciencias, 11% men and 7% women; 17.5% acknowledged their participation in research work that resulted in academic output such as lectures during scientific events, scientific papers, poster presentations, books, and participation in Clinical Practice Guidelines (CPG).
Revista Colombiana de Anestesiología (the Colombian Journal of Anaesthesiology) was the academic publication with the highest recognition, followed in order of preference by Anaesthesiology, Anestesia, & Analgesia, Anaesthesiology Clinics ofNorth America, British Journal of Anaesthesia, Current Opinion in Anesthesiology, Revista Española de Anestesiología, Critical Care Medicine, Anaesthesia, ASA Newsletter, European Journal of Anaesthesiology, Paediatric Anaesthesia, Acta Anaesthesiologica Scandinavica, Canadian Journal of Anaesthesia.
Work characteristics
Close to 99% of the anesthetists (total = 696) work with a Healthcare Provider Institution (IPS in Spanish). Of them, 41% work in a Level III Healthcare Provider, 35% in a Level IV institution, and 24% in a Level II institution. These healthcare providers are mainly private institutions (59%) and, to a lesser extent public (22%) or mixed (19%) (total n = 696).
The predominant form of work relation was through a service agreement, reported by 47% of the anesthetists. Work relations through associations (unions, cooperatives, simplified stock partnerships) were reported by 33%, and employment by 20%. Regarding form of payment, hourly payment is the most prevalent (50%), followed by payment for procedure (27%), and wages (23%) (total n = 698). No differences were found between women and men regarding the form of payment for their services (x2, P> 0.05); however, a difference was found regarding time since graduation, where hourly payment was more frequent among those who had graduated less than 5 years before (x2, P <0.05). On the other hand, there was a trend towards hourly payment among Level II institutions (x2, P=0.052).
Of the anesthetists surveyed, 28% were not happy with their current jobs and 32% stated their wish to change jobs (total n = 690). There were statistical differences between satisfaction and the desire to change jobs as related to the form of payment, hourly payment being the factor in both cases (x2, P < 0.05).
Regarding the number of work days per week, 49% (n = 340) worked 6 days, while close to 7% worked all the days of the week; and 67% worked 12 or more hours per day (total n = 697). In terms of the number of hours per month, 71% (n = 496) of the anaesthetists (total n = 697) work more than 200h/month. Men worked more hours per month (x2, P < 0.05) and worked more frequently more than 12 hours per day as compared to women (55% vs 41%; x2, P <0.05).
On-site night shifts were done by 61% (n = 429) of the anesthetists (n total = 699), with 45% doing 4 to 6 night shifts per month and 28% doing 1 to 3 night shifts per month. Among those who did on-site night shifts, 72% continued working after the shift. The difference again was in favor of the men who did on-site night shifts more frequently than women (65% vs 50%), and worked more after the night shift (76% vs 58%). For all these cases, the difference was statistically significant (x2, P <0.05).
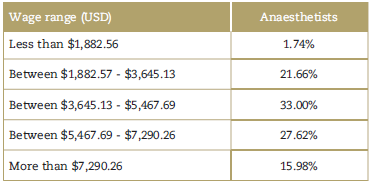
The majority of the anesthetists (64%) earn between USD$18.23 and $27.34 per hour, close to 21% earn between USD$27.34 and $36.45, nearly 6% earn less than $18.23, and close to 8.5% earn more than $36.45 (Table 4). Wage differences were proportionally higher for men than for women (x2, P <0.05).
In terms of satisfaction with the hiring and compensation system, the majority of the anesthetists report an intermediate or low level of satisfaction (72%). In terms of satisfaction with their professional practice, the majority report a high or superior level of satisfaction (73%) (Table 5). There were no differences between men and women in relation to the level of satisfaction with compensation, hiring or professional practice (x2, P > 0.05).

Regarding coverage under the General Social Security System in Health (SGSSS), the majority of the anesthetists surveyed have additional coverage under the Mandatory Health Plan (POS); 61% of the professionals have pre-paid medicine insurance plans, and 12% are covered by special health insurance policies (total n = 698).
Of the anesthetists who participated in the study, 93% make their contributions to the mandatory pension plan; 34% also make payments towards voluntary retirement funds (total n = 698). In terms of the percentage of payment reported, the majority of the anesthetists pay on the basis of 40% or less of their income (53%); 23% pay on the basis of a salary range between 41% and 75%. Of the respondents, 12% had no knowledge of the percentage on which they based their payments to the Social Security System in Health (total n = 700). Regarding affiliation to Work Hazard Insurance (ARL), ARL SURA insurance company is at the top, with a total of 44% of the anaesthetists covered, followed by Positiva ARL, with 19%.
Regarding vacation time, anaesthetists take an average of 17 ± 10 days of vacation per year (based on data derived from their estimates for the past 2 years at the time of completing the questionnaire) (total n = 694). There were no differences between men and women regarding vacation time (Mann-Whitney, P > 0.05). A different approach to analyze the data shows that close to 50% of the anaesthetists take between 15 and 25 days of vacations in the year, 17% take more than 15 days, and 33% take 14 days or less. It is worth noting that there are reports from professionals who do not take vacations. Likewise, the average number of months since the last vacation was 7 ± 6 months at the time of completing the questionnaire, but it is worth highlighting that the upper range for this variable was found to be 36 months, that is, 3 years since the last vacation.
Anaesthetists report an average of 1.86 ± 1.04hours of leisure time in the week, with no differences found between men and women (Mann-Whitney, P > 0.05). The main leisure activity was cinema/TV, followed by sports, reading and music. Other less frequent activities included outdoors (farming or gardening, pet training, horseback riding), cooking, writing, sharing with the family, sewing, carpentry, puzzles, eating out, tourism, video games, yoga or meditation, dancing, photography, and extreme sports.
Discussion
Close to 60% of the anaesthetists who participated in the study were from Bogotá, Antioquia, Atlántico, and Valle del Cauca. The distribution according to gender, age and geographic department is similar to the one found in the S.C.A.R.E. databases.8
The vast majority of the anesthetists (89%) practice in capital cities for financial and quality-of-life reasons. In view of the above, if salary adjustments are achieved and some living and working standards are maintained (technology resources, training opportunities, housing), these professionals might find it attractive to work in places other than the capital cities.
According to the study, 74% of the anesthetists surveyed have children, most of them 2 (35%), or 1 (21%). These figures are similar to those reported for the general population in other studies, such as the 2012 survey conducted by the National Consulting Centre (Centro Nacional de Consultoria).9
Regarding academic training, the number of anesthetist trained abroad (14%) is worth noting, and it correlates with the steady increase in the number of title recognitions. According to the training recognition system of the Ministry of Education, the number of title recognitions increased from 327 in 2011 to 558 in 2014, accounting for an increase of 85%. Training abroad took place mainly in Spain, Brazil, Argentina, Mexico, Ecuador, Venezuela and Costa Rica. Of 231 new title recognitions recorded between 2011 and 2014, 104 were formalized in 2016.8
Close to 75% of the respondents reported having some level of mastery of the English language, a proportion that is much higher than the national average. However, only 12% are proficient in English, a factor that might have a negative influence on the competitiveness of Colombian anaesthetists, limiting academic and job opportunities abroad.
In terms of work conditions, the service agreement modality is the most frequent form of labor relation, followed by hiring through associations (unions, cooperatives, simplified stock partnerships), and finally, employment. These results are similar to those found by prior studies conducted by S.C.A.R.E, which show the same trends. 8 Together with the most recent finding of the "Cendex" study, these results point to the lack of contractual regulation and the existence of sundry hiring modalities that require comprehensive regulation and unity in terms of form and denomination.10
As far as the work schedule is concerned, the Colombian Labour Ministry recommends a maximum of 8 hours per day and 48h/wk.11 According to the study, most anaesthetists usually work 12 hours or more per day, and more than 60h/wk. Consequently, the average of the number of hours per day, number of days per week, number of hours per week and number of hours per month, is higher than recommended by the Labour Ministry11 and higher than the average work schedule of anaesthetists in countries like the United States or Canada, where the average number of work hours per week is not greater than 50, and this includes clinical care, administrative work, and time devoted to teaching and professional development.12,13 It is worth highlighting that the results of this study are no different from those of prior studies conducted by S.C.A.R.E in this regard. 8 This means that, despite the recommendations, there still an issue with work overload among Colombian anaesthetists.
Both the Australian Medical Association as well as the Latin American Confederation of Anaesthesia Societies (CLASA) have established Burnout Guidelines and determined the risk based on the work schedule. Under those standards, low risk means working less than 50h/wk and no more than 10 consecutive hours per day with three or more short rest periods during the day, and no night shifts or extra time.14,15 According to these standards, the vast majority of Colombian anaesthetists are at a high or significant risk of burnout due to work overload. Comparisons between genders show significant differences in terms of number of working hours and larger number of shifts (higher among men), which is reflected in a higher monthly income among men.
Burnout has been shown to affect attention, vigilance, memory, decision-making ability, reaction time, psycho-motor development and, consequently, patient safety. Because of the medicolegal implications, there is a need to adopt strategies and take steps designed to prevent and manage burnout.14,16-24
In terms of compensation and income, the average for anaesthetists is close to 22 minimum monthly wages. According to a study conducted by the Colombian Association of Clinics and Hospitals (ACCH) hourly compensation for anaesthetists in 201425 amounted to USD $25.86 in high complexity institutions, and to USD $27.43 in intermediate complexity hospitals. In another study conducted by S.C.A.R.E in 2013, 8 the average hourly compensation was USD $21.30, and the average monthly income was USD$5,443.70. Finally, an older study called "Environmental and contextual factors that influence compensation and quality of life of anaesthetists in Colombia" conducted in 2011 by "Empresa del Eje Cafetero" University Foundation26 reported an average monthly income of $4,348.62 (21.6 minimum monthly wages), and USD $19.74 per hour. Consequently, it would be right to infer that there is no evidence of increase in the income received by anaesthetists in Colombia over the past five years. This is in contrast with countries like the United States and Canada, where the average annual income for anaesthetists was approximately USD $325,000 in 2011, and USD$358,000 in 2015.12,13
Finally, in terms of satisfaction with professional practice, the vast majority of the anaesthetists were highly satisfied with their specialty, although the level of satisfaction with the hiring and compensation systems was low. A recent study conducted in the United States12) showed that only 53% of the anaesthetists were satisfied with their income, and only 49% would specialize again in anesthesiology.
The strength of this study is the number of participating anaesthetists, which could reflect the real conditions regarding the factors assessed. However, its downside is the low representation of non-capital cities in the analysis. Although validated tools were not used for determining work satisfaction, it is expected that the questions asked will reflect this variable at least in a preliminary way.
Conclusions
Evidence was collected about a population of anaesthetists who practice mainly in capital cities because of financial reasons and standard of living. Although there is evidence of a growing number of anaesthetists trained abroad, most of them have a basic level of proficiency in the foreign language, this being quite notorious as relates to English, the main language for publication in medical science.
Work overload was identified among anaesthetists, with a significant or high risk of burnout. However, the reason for work overload might be the need for higher income for which a price is paid in terms of individual health. This is also related with the fact that although the majority of the anaesthetists were highly satisfied with the practice of their specialty, their level of satisfaction with hiring and compensation systems was low.
If the health needs of the population are to be met, healthcare human resources must be afforded optimal working conditions. These results deserve in-depth analysis and require a reflection on the situation of anaesthetists in order to take the relevant steps to improve the wellbeing and quality of life of Colombian anaesthetists.
Ethical responsibility
Protection of human beings and animals. The authors declare that no human or animal experiments were performed as part of this research.
Data confidentiality. The authors declare that the protocols of their place of work regarding patient data disclosure have been followed.
Right to privacy and informed consent. The authors declare that this article does not contain information that may allow identification of the participants.

