











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
On February 11, 2020, the international taxonomy committee gave the new coronavirus the name of Severe Acute Respiratory Syndrome Coronavirus type 2 (SARS-CoV2) 1. It is the etiologic agent responsible for COVID-19, the disease declared as a pandemic by the WHO on March 11, 2020, and which has caused more than 319 million cases and over 5 million deaths worldwide 2. Two coronavirus-related outbreaks had already occurred in this century, the first in 2002 caused by SARS-CoV and the second in 2012 caused by MERS-CoV (Middle East Respiratory Syndrome Coronavirus) 3-5.
With at least 28 million elective procedures postponed during the first three months of the COVID-19 pandemic, the number of patients who will be requiring surgery after suffering from the disease will grow rapidly. Due to the potential multi-system compromise caused by COVID-19, timing of an elective procedure must be carefully planned 6.
The objective of this article is to carry out a literature review on the topic of the adequate time to subject a patient who has had COVID-19 to an elective procedure, the preoperative tests and the degree of clinical optimization required according to the complexity of the procedure and the patient's clinical condition, with the aim of reducing perioperative risks.
PATHOPHYSIOLOGY OF COVID-19
SARS-CoV-2 replication starts when the virus binds to the epithelial cells of the respiratory tract, triggering an uncontrolled immune reaction aimed at containing the infection but which also explains damage to the healthy tissues 7-9.
There is a wide range of clinical manifestations. The most frequent symptoms include fever, fatigue, anorexia, headache, rash, diarrhea, myalgia, arthralgia and neurologic compromise. Tissue damage resulting from immune response imbalance may trigger coagulation disorders such as disseminated intravascular coagulation, thrombosis and consumption bleeding. The most commonly described complications are pulmonary, such as acute respiratory distress syndrome (ARDS) 10, followed by acute renal injury, liver injury, and inflammatory and functional cardiomyopathy 11. Tissue damage markers, which are also considered indicators of disease severity, include C reactive protein (CRP), elevated ferritin, D dimer, LDH, lymphopenia, anemia, thrombocytopenia, leukocytosis or leukopenia 12.
Among patients infected with SARS-CoV-2, 85% will have no symptoms or a mild form of the disease, 15% will need hospitalization due to moderate disease, 5% will require advanced oxygen therapy, and 1% will need critical care. Moreover, up to 5% of all patients will have residual symptoms for as long as 8 weeks or may even develop chronic symptoms associated with the primary SARS-CoV-2 infection.
POST-COVID-19 SYNDROME AND ASSOCIATED COMPLICATIONS
Patients with persistent COVID-19-related symptoms after the acute phase have been categorized under a clinical syndrome called Long COVID, which is divided into two main categories: subacute COVID and chronic COVID or post-COVID syndrome 13-14.
An important relationship has been found between the onset of long COVID and factors such as symptom intensity during the acute infection: need for intensive care unit (ICU) management with or without invasive mechanical ventilation; persistence of symptoms during the subacute or chronic phase; perception of diminished quality of life; and pulmonary function abnormalities 14. Other variables associated with this condition include prior pulmonary disease, high body mass index, advanced age, and belonging to a racial minority 14. However, it is clear that asymptomatic patients or patients with mild symptomatology are not exempt from developing this condition 15.
The countries with the most extensive published literature on this topic are China, the United States, France, Spain, Italy and the United Kingdom, since they were epicenters of contagion during the initial phase of the pandemic 16-20. One of the largest studies describing the long-term effects of COVID-19 was conducted in a cohort of1733 patients in Wuhan, China 16. Using tools such as questionnaires, physical exam, 6-minute walk test, serum tests, pulmonary function tests in selected cases, and high resolution lung tomography, it described that 76% of the patients reported at least one long COVID-related symptom, the most frequent being fatigue and muscle weakness (63%), sleep disorders (26%), and anxiety/depression (23%).
Similar findings were reported in the study by Carfi et al. 20, which followed 143 patients during a 60-day period following acute SARS-CoV-2 infection. The study documented persistent symptoms in 87% of cases, including fatigue (53.1%), dyspnea (43.4%), joint pain (27.3%) and chest pain (21.7%); 55% of the patients continued to experience three or more symptoms, and 44.1% reported diminished quality of life.
WHEN TO TAKE A POST-COVID-19 PATIENT TO ELECTIVE SURGERY
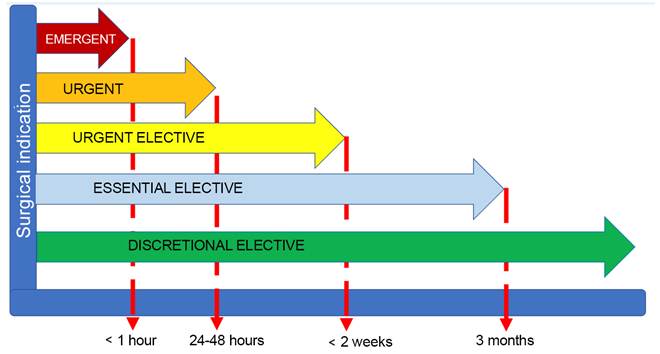
According to the urgency of their indication, surgical procedures are classified as emergent, urgent, elective-urgent, essential elective, discretional elective or non-essential 21 (Table 1, Figure 1).
Table 1 Types of surgeries according to the urgency of the procedure.
| Surgery | Definition | Examples |
|---|---|---|
| Emergent surgery | Cannot be postponed for more than 1 hour after it is scheduled | Trauma in unstable patient Cardiac tamponade Acute occlusive vascular injury |
| Urgent surgery | Must be carried out within 24 and 48 hours | Acute appendicitis Acute cholecystitis Open fractures |
| Elective/urgent surgery | Must be carried out within less than 14 days | Cerebral aneurysm repair Elective cesarean section Closed fractures |
| Essential elective surgery | Can be postponed for more than 14 days but less than 3 months | Oncologic surgery Hernia repair Reconstructive surgery |
| Discretional elective surgery | Can be performed 3 months after it is scheduled | Plastic surgery Bariatric surgery Joint replacements |
Source: Autores.
Elective surgery is defined as a surgical procedure for which there is time enough to adequately assess risk and benefits of the intervention and plan for the right timing 22. It is imperative to understand that elective surgery is not the same as optional surgery, but rather a procedure which does not need to be performed in response to a life-threatening situation; however, it has to be borne in mind that postponing or cancelling an elective surgery could potentially give rise to significant complications in 50% of cases 23.
The following considerations must be taken into account during the preoperative assessment of patients who have recovered from COVID-19 and are scheduled for an elective surgical procedure: severity of the initial clinical picture, persistent symptoms, comorbidity, clinical priority, fitness before and after the infection, risk of disease progression, and complexity of the surgery 6,24.
Apart from the above, the anesthetist must be familiar with the clinical phases of COVID-19: ongoing or symptomatic disease, post-COVID-19 syndrome or chronic COVID-19, and resolved COVID-19. Tools such as the clinical severity scale for this condition can be introduced as part of the assessment, in order to classify the disease as asymptomatic or mild, moderate, or severe, thus providing support for decision-making regarding the management approach in each case (Tables 2 and 3) 6,13.
Table 2 COVID-19 classification.
| Classification | Definition |
|---|---|
| Acute COVID-19 | COVID-19 signs and symptoms that manifest for up to 4 weeks after the onset of the clinical picture |
| Ongoing subacute or symptomatic COVID-19 | Patients who continue to exhibit symptoms between 4 and 12 weeks after the acute infection |
| Post-COVID-19 syndrome or chronic COVID-19 | Includes patients with persistent signs and symptoms beyond 12 weeks after the onset of acute COVID which are not attributable to other diagnoses |
| Resolved COVID-19 | Complete resolution of COVID-19 signs and symptoms |
Source: Autores.
Table 3 COVID-19 clinical severity.
FiO2: Fraction of inspired oxygen; PaO2: Arterial oxygen pressure; SO2: Oxygen saturation. Source: Autores.
It is important to stress that even if patients who have recovered from COVID-19 have persistent symptoms involving multiple systems, it is those patients with cardiopulmonary compromise who have most commonly been found to have adverse perioperative outcomes. The incidence of potentially lethal complications in these patients is as high as 50%, with 30-day mortality of 19.1% in elective surgery, and 26.0% in urgent surgery 25. The risk is higher in male patients, over 70 years of age, American Society of Anesthesiologists (ASA) classification 3 to 5, with underlying malignant neoplasm, or urgent or major surgery 26.
Several initiatives aimed at tackling this problem emerged during the pandemic. One example is the COVIDSurg Collaborative 27 which conducted a multi-center, prospective cohort study with 140,231 patients taken to elective and urgent surgery during the pandemic; of these, 3,127 (2.2%) had a preoperative diagnosis of SARS-CoV-2. Thirty-day mortality in patients with no SARS-CoV-2 was 1.4% (95% CI [1.4-1.5]). In patients with a prior diagnosis of SARS-CoV-2 infection, an inverse correlation was observed between the time to surgery after COVID-19 and 30-day mortality, which was 9.1% within the first 2 weeks, 6.9% for patients intervened after 3 to 4 weeks, 5.5% for patients taken to surgery within 5 to 6 weeks, and 2% after 7 weeks. In this last group, mortality was higher among patients with persistent symptoms than in patients whose symptoms had resolved or who had remained asymptomatic during the acute phase of the infection. Similar findings were reported by Jonker et al. 28, who described a 30-day mortality of 4% for the group with no COVID-19 diagnosis as compared to 16% in patients with perioperative SARS-CoV-2 infection, for whom higher rates of pulmonary and thromboembolic complications were also described. Finally, in their cohort study, Doglietto et al. 29 reported higher mortality and greater surgical complications in patients with COVID-19 when compared to patients who did not have the infection.
These findings can be readily explained given that, from the cardiovascular perspective, studies have shown that 60% to 78% of patients with SARS-CoV-2 infection exhibit inflammatory changes on cardiac magnetic resonance imaging, which can manifest in the form of left ventricular dysfunction and arrhythmias, among others 30. In patients with risk factors for cerebrovascular disease and advanced age taken to surgical procedures, different types of complications are observed more frequently, including prolonged hospital stay, slow recovery, multiple sequelae, and even death. Moreover, it has been found that SARS-COV-2 infection is a risk factor for pulmonary and venous thromboembolism, with an incidence of 6.6% and as high as 18.9% in critically ill patients 26 who are considered to be at high risk for perioperative thromboembolism.
Added to the above, multiple anesthesia and surgical societies worldwide 6,24 have recommended not to schedule elective surgery during the time that the patient can transmit the infection. The Centers for Disease Control and Prevention (CDC) published their guidelines for extending isolation precautions 10 days following the onset of symptoms in cases of mild to moderate disease, and 15-20 days in cases of severe disease, provided no fever is documented for 24 hours without the use of antipyretics and there is evidence of reduced symptoms like cough or dyspnea 31. In 95% of critically ill patients who are highly immunocompromised, virus with the ability to replicate has not ben documented beyond 15 days after the onset of symptoms 32. For patients who are receiving immunosuppressants such as dexamethasone 6 mg/day (equivalent of 40 mg of prednisolone) for 10 days and/or monoclonal antibodies, the opinion of the infectious disease specialist is required.
Bearing all of the above in mind, some authors suggest that asymptomatic COVID-19 patients can be taken to the surgical procedure 4 weeks after being diagnosed. In contrast, patients who were symptomatic during the acute phase of the infection should not be taken to any elective procedure within the first seven weeks after the diagnosis, unless the risk of postponing surgery outweighs the risk of COVID-19-related postoperative morbidity and mortality 6. In patients who were critically ill and required ICU admission, the recommendation is to perform this type of intervention once 12 weeks after the diagnosis have elapsed 24. However, these recommendations do not eliminate the need for specialized and personalized assessment, as well as multidisciplinary perioperative management for each individual patient.
Other factors that must be taken into account when deciding to take a patient to surgery include availability of hospital resources, sufficient healthcare human talent and personal protective equipment needed for safe care. Different societies 33,34 have published scores or scales to help guide the medical team regarding the relevance of performing a surgical procedure. One example is the MENTS (Medically Necessary, Time-sensitive Procedures) score suggested by the American College of Surgery (33). Preoperative assessment should include time since clinical recovery from COVID-19, frailty status, fitness, and return to pre-COVID-19 baseline condition. In certain cases, multidisciplinary rehabilitation or prehabilitation must be performed 35.
PREOPERATIVE TESTING IN POST-COVID-19 PATIENTS
The aim of the preoperative assessment is to determine the patient's clinical condition and, if needed, optimize it before the surgery. There are no clinical practice guidelines to this date that can guide the preoperative assessment and the preoperative tests required for patients who have suffered from COVID-19 and need an elective procedure. In Oregon, United States, a multidisciplinary team consisting of anesthesia and surgery leaders 35 working in a hospital setting developed a protocol for preoperative assessment and selection of laboratory tests for post-COVID-19 patients. This protocol stratifies patients according to the type of surgical procedure (major or minor surgery) and clinical condition at the time of surgery (asymptomatic or symptomatic). In all cases, the suggestion is to ask for an electrocardiogram, complete metabolic panel including lactate, and complete blood count. For symptomatic patients who will be taken to minor surgery and for all patients scheduled for major surgery they suggest ordering D dimer and natriuretic peptides (BNP and NT-PRO-BNP). In the event the latter is outside normal limits and the clinical exam suggests cardiovascular decline, the assessment should be expanded to include an echocardiogram. Coagulation times, fibrinogen and a chest X-ray must be ordered for all patients undergoing major surgery, regardless of their clinical condition. Finally, pulmonary function tests are suggested in patients who had a severe course of CODIVD-19, in case they need major surgery. Other tests such as prealbumin, lactic dehydrogenase and ferritin are left up to the surgical team, depending on disease severity.
The results of a survey conducted among 154 anesthetists with the aim of gathering the opinions and practices of these professionals in their daily practice with patients who suffered COVID-19 and needed elective surgery were published in May 2021 in the Indian Surgical Oncology Journal 36. Most of the respondents concluded that it is important to optimize the management of comorbidities and reassess fitness before a surgical procedure. They also pointed to the need of performing chest X-ray, electrocardiogram and coagulation profile in all recovered patients. Regarding lung function tests, they agreed that blood gases, pulmonary high-resolution computed axial tomography (HRCT) or lung function tests must be performed in patients who had moderate-to-severe hypoxemia or significant cardiac symptoms during COVID-19, and also in patients scheduled for major abdominal vascular, cardiac or thoracic surgery and in elderly patients. As for cardiac function assessment, they suggest ordering troponin I as well as an echocardiogram if the patient had significant cardiac symptoms or in patients undergoing major abdominal, vascular, cardiac or thoracic surgery. Only 1.9% of the respondents suggested using NT-PRO-BNP.
In terms of diagnostic testing for COVID-19 in the perioperative setting, Reverse Transcription-Polymerase Chain Reaction (RT-PCR) positivity is not correlated with live virus shedding and, therefore, assessing infectivity risk within the three months following diagnosis has little or no value. Beyond that time, the test should be performed before surgery in order to avoid the postoperative complications and mortality that have been described as significant in patients with acute concurrent infection with this virus 37,38. Another aim of preoperative diagnosis is to preserve the safety of the surgical team. This has been a controversial topic due to the lack of publications with high-quality evidence to this date. The urgency of the condition, the local resources and the potential outcomes in case of postponing the surgery must all be part of the decision.
CONCLUSIONS
Although evidence is still limited, different scientific societies have issued recommendations regarding adequate timing for elective surgery. For patients who were asymptomatic, the time interval is four weeks after the diagnosis of SARS-CoV-2 infection, while for symptomatic patients with mild to moderate disease course, the interval is al least seven weeks, and twelve weeks if ICU admission was required. Although there are no guidelines regarding which preoperative tests should be ordered, there are institutional protocols based on expert consensus that can guide the treating surgical team in this setting. Despite the fact that these guidelines are useful in our practice, they should not take the place of personalized assessment as the starting point for decision-making. More robust studies that approach this topic are required.

