










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Espanhol (pdf)
Espanhol (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
versão impressa ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.24 no.1 Medellín jul./dez. 2012
ORIGINAL ARTICLES DERIVED FROM RESEARCH
Penetration of three adhesives in proximal white- spot carious lesions: an in vitro study
Olga Lucía Zarta1; Alba Lucía Zuluaga Valencia2; María Cristina Huertas Díaz3; Juan Sebastián Lara4; Ingrid Katherine Quintero5; Marisol Téllez6; Margarita Úsuga7; Stefanía Martignon8
1 Dentist, Universidad Javeriana, Bogotá; Specialist in Prosthodontics,
Universidad El Bosque, Bogotá. Associate Professor, Director of the
Specialization Program on Operative Dentistry, Esthetics and Dental
Materials, Universidad El Bosque, Bogotá. Member of UNICA (Caries
Research Unit)
2 Dentist, Colegio Odontológico Colombiano, Cali, Specialist in Pediatric
Dentistry, Universidad El Bosque, Bogotá
3 Dentist, Universidad Cooperativa de Colombia, Pasto, Specialist
in Pediatric Dentistry, Universidad El Bosque, Bogotá, Specialist in
Functional Orthopedics and Orthodontics, Universidad Cooperativa de
Colombia, Bogotá. Professor, Universidad Cooperativa de Colombia,
Pasto
4 Dentist, Universidad El Bosque, Bogotá. Member of UNICA. Pediatric
Dentistry MSc Candidate, Universidade de São Paulo, Brasil
5 Dentist, Universidad El Bosque, Bogotá, Orthodontic student,
Universidad El Bosque, Bogotá
6 Dentist, Universidad El Bosque, Bogotá. MSc in Public Health and
PhD. in Clinical Epidemiology, University of Michigan, Ann Arbor,
USA. Associate Professor, Dental Public Health Sciences, Maurice H.
Kornberg School of Dentistry, Temple University, Philadelphia, USA
7 Dentist, Universidad de Antioquia, Bogotá, Specialist in Pediatric
Dentistry, Pontificia Universidad Javeriana, Bogotá. Dentistry MSc
Candidate, Universidad Nacional de Colombia, Bogotá. Associate
Professor, UNICA, Dental Faculty, Universidad El Bosque, Bogotá
8 Dentist, Pontificia Universidad Javeriana, Bogotá, Specialist in
Pediatric Dentistry; specialist in Higher Education, Universidad El
Bosque, Bogotá. Ph.D. in Health Sciences, University of Copenhagen,
Copenhagen, Denmark. Associate Professor and Director of UNICA,
School of Dentistry, Universidad El Bosque, Bogotá
SUBMITTED: DECEMBER 6/2011-ACCEPTED: MARCH 27/2012
Penetración de tres adhesivos en lesiones interproximales de caries de mancha blanca: estudio in vitro. Rev Fac Odontol Univ Antioq 2012; 24(1): 84-95.
ABSTRACT
INTRODUCTION: the treatment of early proximal carious lesions represents a challenge to modern conceptions of cariology
and operative dentistry. The possible solutions include, besides an early diagnosis, development of new materials to control early caries
progression. The objective of this in vitro study was to evaluate the degree of penetration of three adhesives: Excite (Ivoclar-Vivadent),
Prime & Bond NT (Dentsply), and Single Bond (3M-ESPE), in the process of sealing white-spot non-cavitated proximal lesions.
METHODS: 117 extracted human premolars with ICDAS 2 white-spot non-cavitated proximal lesions mounted on plaster, to simulate oral cavity
conditions, were randomly sorted out in each of the three groups. The lesions were sealed with each of the materials previously mixed
with methylene blue; longitudinal sections of 250 µm were obtained, and they were later analyzed on photographs taken with a stereo
microscope. These variables were evaluated: total lesion coating, lesion's histologic depth (in micrometers), and the adhesive's maximum
penetration.
RESULTS: a total of 116 teeth were analyzed. Entire lesion coating was found in 52.5% of the cases; 75% were located in the
enamel's internal half, with an average depth of 854 ± 493 µm. The adhesive's maximum average lesion penetration was 697 ± 412 µm. No
statistical significant differences were found among the groups (Kruskal Wallis and Spearman correlation; p > 0.05).
CONCLUSION:these
three low-viscosity adhesives with high amounts of TEGDMA and HEMA effectively achieved covering and penetrating of the material for
sealing early proximal carious lesions.
Key words: white-spot lesions, dental caries, adhesive dental coating.
INTRODUCTION
Dental caries is defined as an imbalance of dental structure and surrounding plaque fluid, which triggers mineral loss and may produce dental structure loss.1, 2 Proximal caries occurs from the interdental contact point towards the gingival margin, a spot that easily retains biofilm and which is hard to access for mechanical plaque removal.3
Carious lesions on proximal surfaces are challenging to both industrialized and developing countries.4, 5 It is therefore necessary to detect these lesions in their initial stages, in order to avoid their progression, by means of preventive therapies and therefore preventing surgical treatment.6
Thanks to modern dentistry principles—specifically cariology—minimally invasive treatments are now available, as well as adhesive restoring materials which protect the maximum possible amount of dental structure, stop progression of the lesions, and allow easy dental cleansing.2 The concept of minimal intervention dentistry involves five general principles: 1) initial scientific diagnosis, by means of suitable diagnostic methods; 2) disease control by educating patients and reducing biofilm; 3) re-mineralization of early lesions; 4) minimum surgical interventions; 5) favoring faulty restorations repair instead of replacing them.6, 7
With the purpose of restoring early enamel carious lesions, a conservative approach has been recently suggested consisting of arresting, controlling and monitoring lesions by means of techniques and materials such as sealants8 and adhesives,9 adhesive patches,10 and more recently, infiltrations.11, 12 So far, both sealing and infiltrating proximal lesions have proven to be clinically effective after using them for more than 18 months.9, 11, 12 There is no consensus on the most effective and practical material to control progression of early carious lesions.
Sealing proximal carious lesions with adhesives has yielded greater benefits than fissure sealants13 because adhesives have lower viscosity, greater facility to reach the proximal region, lower technique sensibility, and more retention.14 Filling the enamel's demineralized pores is an emerging research field supported by studies that have verified these materials' effective penetration in carious lesions, thus preventing their progression.15-18
The purpose of this in vitro study was to evaluate the degree of penetration of three adhesives: Excite (Ivoclar-Vivadent), Prime & Bond NT (Dentsply), and Single Bond (3M), in the process of sealing natural lesions of non-cavitated proximal caries in human teeth.
MATERIALS AND METHODS
This study was conducted at Universidad El Bosque, Bogotá. In order to assess the three adhesives' degree of lesion penetration, the methodology reported by Martignon in 2005 was used.13
Sample
The study was performed on extracted natural (premolar) teeth with ICDAS type 2 white-spot proximal carious lesions.
In order to establish the proportions for calculating sample size, a pilot test was conducted with the aforementioned technique13 in nine samples, three for each of the adhesives: Excite (Ivoclar Vivadent), Prime & Bond NT (Dentsply) y Single Bond (3M ESPE), with subsequent stereomicroscope evaluation of the material's penetration depth in proportion to lesion depth. The arcsine formula was applied in order to compare the test of proportion hypothesis, with 0.05 alpha and 80% power. This produced a total sample of n = 117 lesions, that is, 39 per group.
Two trained examiners (ALZ, MCH) collected 420 human premolar teeth extracted for orthodontic purposes, from a stock of teeth stored in timol aqueous solution. An examiner who was previously calibrated on ICDAS dental caries visual diagnosis criteria (SM) examined the samples with the aid of a ball-ended probe (WHO), selecting the ones that presented non-cavitated proximal carious lesions, with a visual diagnosis of ICDAS 2, white spot lesion.19 Exclusion criteria included teeth with hypoplasia, fractures, fracture lines, fluorosis, and any other enamel development defect. Photographs of all the lesions were taken.
Sample preparation
The 117 selected teeth were coded and randomly allocated into each of the three groups, by means of a random number table:20 1) Excite (Ivoclar Vivadent) (E), 2) Prime & Bond NT (Dentsply) (PB), 3) Single Bond (3M ESPE) (SB). The teeth were temporarily removed from their conservation solution and three marks were drawn on their occlusal surfaces with indelible ink in order to delineate the proximal lesions' buccal and lingual/palatal borders, thus leaving a guide for the subsequent longitudinal sections. They were later mounted on plaster casts imitating their location inside the mouth and on the alveolar bone, leaving the crowns free. In order to imitate the proximal gap achieved after several days of using orthodontic separators while sealing an proximal lesion in clinical conditions,8 a neighboring tooth was located at a distance equivalent to the width of a toothpick (0.8 mm in diameter).13
Afterwards, the samples were submerged again in timol solution until the time of the sealing procedure.
Lesion sealing
Each adhesive was previously mixed with 5% methylene blue in 100% ethanol —a staining used for in vitro coloring—. Two drops of each adhesive were mixed with a drop of staining. Once one of the authors (OLZ) was trained, she performed this procedure on each proximal lesion (figure 1):13

- Cleansing the tooth to be sealed, with conventional toothpaste and a prophylactic brush.
- Isolating of the adjacent tooth with a nonstick (Teflon) tape.
- Previously dryed, the proximal surface was etched with 37% phosphoric acid for 15 s.
- Rinsing with water for 30 s and drying without dehydrating the tooth.
- Replacing the Teflon tape.
- Once dried, applying the adhesive (mixed with methylene blue) on the lesion with a micro-brush, a probe, and dental floss in order to reach the lesion and to remove remains.
- Gentle air drying.
- Photo-polymerization of the adhesive, according to the manufacturer's instructions.
- Polishing the sealed surface with polyester sandpaper.
Histological sections
After sealing, the samples were removed from the plaster casts and introduced in bottles that had been previously coded. Longitudinal sections of 250 µm were obtained by means of a microtome (Isomet, Buehler) of lower speed at 500 rpm, having the markings as a reference to include the interproximal lesion in each case. Sectioning was performed at Universidad Nacional de Colombia's Research and Technical Development Laboratory, Bogotá.
Analysis of histological sections
Each dental tissue section was placed at the stereomicroscope (60 amplifications) with an incorporated digital camera. Photos of the sections were taken and filed independently in a computer for subsequent analysis. These aspects were analyzed on each section (figure 2):
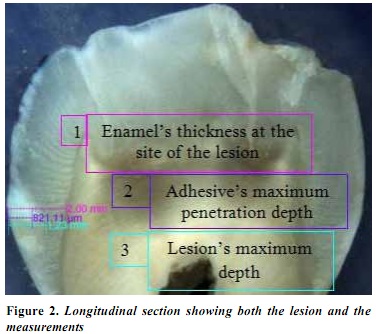
- Lesion entirely covered with the adhesive: yes; no.
- Lesion's histological depth: external enamel half; internal enamel half; enamel cement junction- ACJ- external dentine third.
- Lesion depth in µm.
- Maximum penetration (depth) of adhesive in the lesion (in µm).
The photographs allowed observing the lesion's coating with resinous material (criterion 1) as well as the lesion's histological depth per zone (criterion 2). The remaining criteria were evaluated by means of the Dpx View Pro EE EF software®, once these points of reference had been marked: external site at the enamel surface corresponding to the lesion's midpoint, the proximal lesion's deepest part, and deepest penetration site of the material marked with the staining. The software calculated lesion's depth in µm (criterion 3), and maximum adhesive penetration in µm (criterion 4).These calculations were performed by two examiners (JSL, IQ), who had been previously trained and calibrated by an expert (Kappa inter-rater reliability = 0.81) at the Department of Cariology and Endodontics of Copenhagen University, Denmark. The obtained data were directly registered in an Excel database.
Statistical analysis
The results were analyzed by means of descriptive statistics (MT). H. Kruskal-Wallis tests were performed in order to identify penetration differences among the three adhesive groups.
Whenever differences appeared, the non-parametric Mann-Whitney test was applied. Moreover, Spearman's correlation test was used to establish correlation between adhesive penetration and lesion depth.
RESULTS
In total, the sample comprised 116 teeth with proximal sealed lesions, distributed in three groups, like this: PB: n = 39, E: n = 39 and SB: n = 38; one tooth from the sample was lost during the sectioning process.
Amount of lesion coating
In 52.5% of the sealed teeth, the adhesive covered the whole lesion, with these percentages by group: 66.7% (E), 43.6% (PB), and 47.4% (SB), with no statistically significant differences among the groups (p > 0.05).
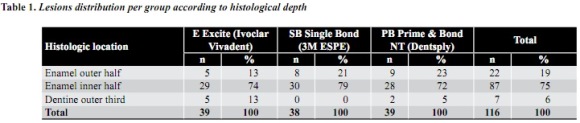
Lesion histological depth
The analysis of interproximal lesions histological depth revealed that most of them (75%) were located in the enamel inner half—and each group experienced the same tendency— (table 1). Nearly 1/5 of the lesions (19%) were located in the enamel outer half, and only 6% in the dentine.
Lesion depth in micrometers
Table 2 shows the lesions average depth in µm (854 ± 493 µm) and these averages per group: 761 ± 415 µm (SB), 889.5 ± 499.5 µm (E), and 911 ± 308.5 µm (PB); correlation among the groups did not present significant differences (p > 0.05).

Maximum penetration (depth) of adhesives in lesions (in µm)
The maximum average of adhesive penetration in the lesion was 697 ± 412 µm, with these average values per group: 612.5 ± 354 µm (SB), 693.3 ± 471.6 µm (PB), and 786 ± 393.5 mm (E), and no significant differences among the groups (p > 0.05).
DISCUSSION
This study showed that the three adhesives were able to seal and penetrate white-spot proximal lesions. In 1975, Dávila et al15 reported that low molecular weight adhesives may flow through carious lesions and partially or entirely fill the microspaces. In vitro studies on artificial carious lesions carried out by Robinson et al (2001)16 and Gray et al (2001)17 demonstrated the effectiveness of a material that successfully allowed sealing and partially filling the demineralized intercystal gaps of artificial lesions.
We decided to use adhesives in our study because they have a greater capacity to retain sealants,14 and because in an in vitro pilot study they proved to be more efficient for sealing and penetrating lesions.13
Sealing white-spot proximal carious lesions with three dentinal adhesives yielded a penetration degree close to 80% of lesion depth—similar among the three groups—.
Paris et al (2007)18 analyzed the penetration capacity of five dentinal adhesives and fissure sealants available in the market on artificial early lesions of bovine enamel, finding out a greater penetration coefficient in the materials containing ethanol (20%) as agent, as well as TEGDMA and HEMA, which matches the components of the adhesives used in the present study.
The effectiveness of a sealant depends on its penetration capacity, its wear resistance, the technique used, and its insolubility in the oral environment.6, 17 Histologically, the surface of non-cavitated enamel lesions has a porous volume that ranges between 1 to 5%, that is, 10 to 15 times greater than a healthy enamel.21 In 1989, Goepferd and Olberding reported the presence of resin tags after sealing white-spot lesions with a unfilled sealant, finding out lesion progression underneath the material. They used polarized light microscopy for their study.22
In the present study, in order to evaluate the adhesives' lesion penetration capacity, methylene blue staining was used before assessing the substance penetration in histological sections by means of a stereomicroscope. Tyler et al used this technique by mixing 1% methylene blue staining in 100% ethanol with a given adhesive, seeking to evaluate, after hemisecting the teeth and taking photographs, the displacement of dentinal adhesive applied underneath amalgam fillings, as they were condensed. According to these authors, mixing methylene blue with the substance enables visual and photographic observations without producing physicochemical alterations.23 In the present study, we used 5% methylene blue in absolute ethanol, just as suggested by Martignon et al13 in a study on the same topic after trying different dyes. The adhesive/ staining solution was prepared as suggested by Tyler et al.23 Nevertheless, some changes in terms of the adhesive's viscosity and surface tension may occur, so these aspects must be taken into account.
The results obtained by Martignon in 2006,9 in a study conducted with the intention of assessing the efficacy of sealing proximal lesions in adult patients were positive.
Nevertheless, 43.5% of the lesions progressed after evaluation with radiographic subtraction. The sealing procedure, more rather then arresting the lesion, reduces its progression rate, as suggested by other in vitro studies on the field24 and by the most recent clinical studies which have yielded promising results by sealing non-cavitated proximal carious lesions in primary dentition25 and by using infiltrants in both permanent11 and primary dentition.12
CONCLUSIONS
Based on the results of the present in vitro study, the following conclusions may be drawn:
Low viscosity adhesives with high contents of TEGDMA and HEMA such as the ones used in this study are effective for sealing early interproximal carious lesions.
No statistically significant differences occur in terms of penetration depth among these three adhesives: Excite (Ivoclar Vivadent), Single Bond (3M ESPE), and Prime & Bond NT (Dentsply) when used as sealants for early proximal carious lesions.
The authors recommend conducting further studies on the behavior of these lesion sealing/infiltrating materials.
ACKNOWLEDGEMENTS
We would like to thank Doctor Lars Björndal for his helpful participation and guidance in this study.
CORRESPONDENCE
Judith Patricia Barrera Chaparro
Carrera 18 N.° 80-94. Bogotá D. C.
Fundación Universitaria San Martín
Facultad de Posgrados de Odontología
Posgrado de Ortodoncia
Correo electrónico: barrerajudith@gmail.com
REFERENCES
1. Pitts NB, Stamm JW. International Consensus Workshop on Caries Clinical Trials (ICW-CCT) Final consensus statements: agreeing where the evidence leads. J Dent Res 2004; 83 (Spec Iss C): C125-C128. [ Links ]
2. Thylstrup A, Fejerskov O. Clinical and pathological features of dental caries. En: Thylstrup A, Fejerskov O. Textbook of clinical cariology. 2.ª ed. Copenhagen: Munksgaard; 1994; p. 111-158. [ Links ]
3. Bjørndal L, Thylstrup A. A structural analysis of approximal enamel caries lesions and subjacent dentin reactions. Eur J Oral Sci 1995; 103: 25-31. [ Links ]
4. Martignon S, Chavarría N, Ekstrand KR. Caries status and proximal lesion behaviour during a 6-year period in young adult Danes: an epidemiological investigation. Clin Oral Investig 2010; 14: 383-390. [ Links ]
5. Mejare I, Kallestal C, Stenlud H. Incidence and progression of approximal caries from 11 to 22 years of age in Sweden: a prospective radiographic study. Caries Res 1999; 33: 93-100. [ Links ]
6. Kielbassa AM, Muller J, Gernhardt CR. Closing the gap between oral hygiene and minimally invasive dentistry: a review on the resin infiltration technique of incipient (proximal) enamel lesions. Quintessence Int 2009; 40: 663-681. [ Links ]
7. Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry: a review. FDI Commision Project 1-97. Int Dent J 2000; 50: 1-12. [ Links ]
8. Gomez SS, Basili CP, Emilson CG. A 2-year clinical evaluation of sealed noncavitated approximal posterior carious lesions in adolescents. Clin Oral Investig 2005; 9: 239-243. [ Links ]
9. Martignon S, Ekstrand KR, Ellwood R. Efficacy of sealing proximal early active lesions: An 18-month clinical study evaluated by conventional and subtraction radiography. Caries Res 2006; 40: 382-388. [ Links ]
10. Alkilzy M, Berndt C, Meller C, Schidlowski M, Splieth C. Sealing of proximal surfaces with polyurethane tape: a two.-year clinical and radiographic feasibility study. J Adhes Dent 2009; 11: 91-94. [ Links ]
11. Paris S, Hopfenmuller W, Meyer-Lueckel H. Resin infiltration of caries lesions: an efficacy randomized trial. J Dent Res 2010; 89: 823-826. [ Links ]
12. Ekstrand KR, Bakhshandeh A, Martignon S. Treatment of proximal superficial caries lesions on primary molar teeth with resin infiltration and fluoride varnish versus fluoride varnish only: efficacy after 1 year. Caries Res 2010; 44: 41-46. [ Links ]
13. Martignon, S. Approximal caries: prevalence and progression rate in young Danish adults and an innovative non-operative approach for lesions around the EDJ [Monografía Ph. D. Caries] Copenhagen: Universidad de Copenhagen; 2005. [ Links ]
14. Feigal RJ, Musherure P, Gillespie B, Levy-Polack M, Quelhas I, Hebling J. Improve sealant retention with bonding agents: A clinical study of two-bottle and singlebottle systems. J Dent Res 2000; 79: 1850-1856. [ Links ]
15. Davila JM, Buonocore MG, Greeley CB, Provenza DV. Adhesive penetration in human artificial and natural white spots. J Dent Res 1975; 54: 999-1008. [ Links ]
16. Robinson C, Brookers SJ, Kiskham J, Word SR, Shore RC. in vitro studies of the penetration of adhesive resins into artificial caries-like lesions. Caries Res 2001; 35: 136-141. [ Links ]
17. Gray GB, Shellis P. Infiltration of resin into white spot caries-like lesions of enamel: an in-vitro study. Eur J Prosthodont Restor Dent 2002; 10: 27-32. [ Links ]
18. Paris S, Meyer-Lueckel H, Colfen H, Kielbassa AM. Penetration coefficients of commercially available and experimental composites intended to infiltrate enamel carious lesions. Dental Materials 2007; 23: 742-748. [ Links ]
19. Ismail AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H, Pitts NB. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol 2007; 35: 170-178. [ Links ]
20. Kramer MS. Clinical Epidemiology and Biostatistics. A primer for clinical investigators and decision-makers. Alemania: Springer-Verlag; 1988. p. 273. [ Links ]
21. Silverstone LM. Structure of carious enamel including the early lesion. En: Melcher AH, Zarb GA. Dental enamel. Development structure and caries. Oral Sci Rev. Copenhagen: Munksgaard; 1973. p. 100-160. [ Links ]
22. Goepferd SJ, Olberding P. The effect of sealing white spot lesions on lesion progession in vitro. Pediatr Dent 1989; 11: 14-16. [ Links ]
23. Tyler DW, Thurmeier J. Amalgam bonding: visualization and clinical implications of adhesive displacement during amalgam condensation. Oper Dent 2001; 26: 81-86. [ Links ]
24. Meyer-Lueckel H, Paris S: Improved resin infiltration of natural caries lesions. J Dent Res 2008; 87: 1112-1116. [ Links ]
25. Martignon S, Tellez M, Santamaría RM, Gomez J, Ekstrand KR. Sealing distal proximal caries lesions in first primary molars: efficacy after 2.5 years. Caries Res. 2010; 44: 562-570. [ Links ]
