











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Disability is a generic term that includes deficits, limitations in activity and restrictions in participation indicate the negative aspects of the interaction between an individual and its contextual factors, environmental and personal factors 1. It can be associated with chronic health and other problems, such as traffic accidents, natural disasters, conflict, eating habits, and substance abuse. Their rehabilitation culminates in the labor inclusion considered as part of a broader process that is social inclusion, based on equal opportunities, full social participation and finally in practice, which takes place once the person joins a job and participates in all labor and social activities of the company 2.
In addition, the labor inclusion of people with disabilities (PwD) represents one of the greatest challenges for social and labor policies, which leads to experiencing inequality of opportunities, social disadvantages, few job opportunities adapted to their skills, interests, and aptitudes 3.
The employment rate varies according to each country, for a person with a disability finding and keeping a job is a challenge, the World Health Organization (WHO) describes that, in the world, a PwD is less likely to be employed than a person without disabilities 4.
According to the International Labor Organization 5 PwD represents approximately one billion of the world's population and around 80 percent are of working age. However, PwD's right to decent work is often denied, thus facing enormous attitudinal, physical, and informational barriers to equal opportunities in the world of work.
In the same way, some PwD experiences report that when they manage to obtain a job their income is very low and usually worsens with the severity of the disability. Furthermore, they do not correspond to their professional profiles and sometimes they do not have reasonable adjustments in the workplace in accordance with their conditions or the regulations that promote accessibility. It is largely derived from the attitudes of rejection of society due to the social representations that conceive them from incompetence, risk, disability, and inadequate performance that affect the perception of the individual's quality of life 1)(6.
In Colombia, according to the Registry for the Location and Characterization of People with Disabilities (RLCPD) with cut-off as of September 30, 2019, 1,521,114 people with disabilities are registered (Ministry of Health and Social Protection, 2019), of which only 12% are working, 80% do not have a labor contract and only a minority 7% have a fixed-term contract 7.
According to the results of the study by Barisin et al. 8, unemployed women with disabilities have a lower quality of life and health compared to employed women, thus confirming that employment is an important determinant of quality of life-related to employment. On the other hand, we have that Gil et al. 9 suggest that staying busy and productive generates in PwD a feeling of well-being and fulfillment, which is reflected in a better perception of the quality of life 10.
On the other hand, Aguilar & Yusta 11 found that PwD are not fully integrated into the labor market, they have lower activity rates, higher unemployment rates, and lower wages than the rest of the workers .
In the city of Neiva Huila Colombia, as of February 12, 2020, 19,910 people with some type of disability are registered Ministry of Health and Social Protection of Colombia, 12. however, there are no known data on the quality of life and labor inclusion of this population.
In accordance with the above, the objective of this study was to identify the characteristics of labor inclusion and health-related quality of life of people with disabilities.
Methods
Descriptive, analytical, cross-sectional study with quantitative approach and non-experimental design, in a sample of 64 people with disabilities.
Initially, there were 74 adults with some type of disability residing in the city of Neiva, of which 10 were excluded who did not accept to participate in the study due to issues unrelated to the research, the sample finally consisted of 64 people with disabilities.
The inclusion criteria for the study were the following:
1) Be over 18 years old. 2) have a disability. 3) be able to answer the questions of the quality of life scale the WHOQOL-BREF questionnaire, 2004. World Health Organization, 13. And sociodemographic and labor survey. 4) agree to participate in the study by signing the informed consent.
The exclusion criteria were: 1) not working at the time of the survey, 2) not accepting to participate in the study.
The study was carried out in the City of Neiva (Colombia), during the period 2018-2019.
Recruitment was carried out through the identification of public and private companies that had links of people with disabilities within their employees. After locating the companies, letters are sent to the managers to authorize their participation in the study.
Once the participation was accepted by the managers of the companies, the participants were placed to socialize the objectives of the study and invite them to participate.
A survey prepared by the research team was applied with demographic variables such as the participant's age, sex, marital status, education, socioeconomic status, link to the social security system in health, and type of disability DANE 14.
For the evaluation of labor inclusion, a survey was designed with questions such as occupational situation, type of employment relationship, type of company (private, public), the position held, economic sector to which it is linked, salary ranges, type of contract among other. Both questionnaires were subjected to expert judgment and pilot testing.
Quality of life was evaluated by applying the WHOQOL-BREF questionnaire, 2004 (World Health Organization Quality of Life Assessment Instrument, abridged version), World Health Organization- Division of Mental Health. (1996) 13, for which authorization was obtained from the WHO for your use. In its Spanish version, it contains 26 questions that refer to the twenty-four facets of the Whoqol-100 and two general responses, and the rest grouped into four quality of life domains. Each question has five responses that are scored to generate a profile of four dimensions or domains Physical Health (includes seven questions), Psychological Health (includes six questions), interpersonal relationships (includes three questions), and Environment (includes eight questions). the questionnaire allows us to show the perception that people have of the quality of life. With the instrument scores from 0 to 100 are obtained, with zero being the worst quality of life and 100 being the best.
The surveys and questionnaires were administered in the offices or workplaces of the participants.
A database was created on a Microsoft Excel sheet. The Epidat version 4.2 statistical package was used. The age ranges were defined by the Sturges rule. The measures of central tendency with their dispersions and 95% confidence intervals were calculated in the continuous quantitative variables. Percentage frequencies were determined for qualitative variables.
The following study was approved by the Research Committee of the Fundación Universitaria María Cano in the ordinary session # 02 - 2016 of June 21, 2016. With the assignment of code # 013004022016-3112016 and ethical endorsement in the ordinary session of the Ethics Committee (Act 01), held in the city of Medellín, on June 22, 2016.
The study had the guidelines of Resolution 8430 of 1993 15 categorized as risk-free research, and the guidelines of the Declaration of Helsinki 16.
Results
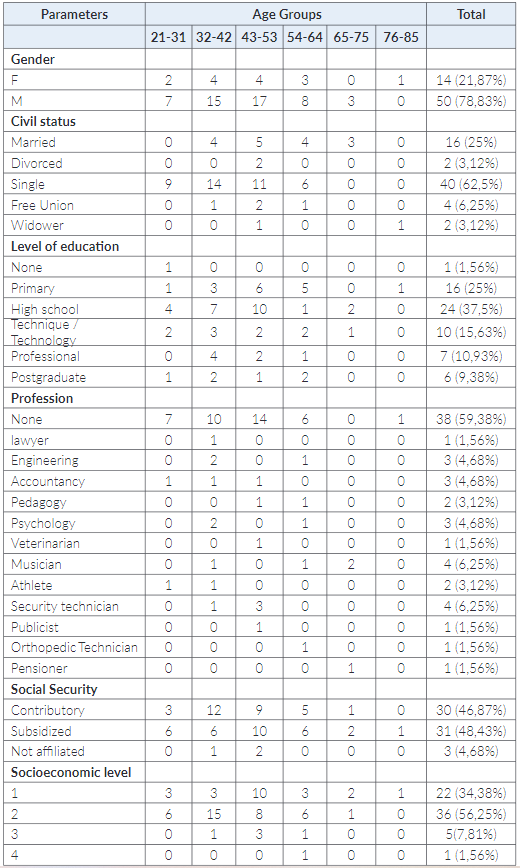
A total of 64 adults with disabilities took part in the study, the mean age was 44.4 years with a standard deviation (SD) of 12.89 and a CI [95%]: 41.18 - 47.62; with a range between 21 and 85 years. The demographic characteristics are presented in Table 1.
The work characteristics are presented in Table 2:

- SMLV current legal minimum wage.
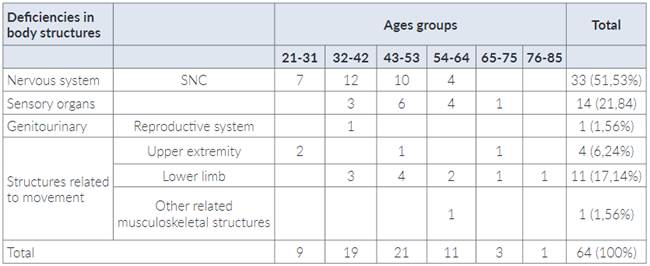
The alterations that generate disability are presented in Table 3:
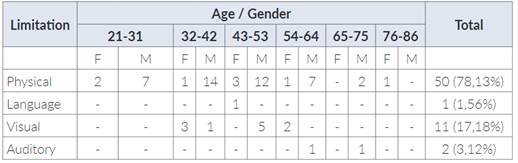
The functional alterations are presented in Table 4. 84.38% of the Participants consulted attend rehabilitation programs, only 15.62% stated that they attended the physiotherapy service.
Table 4 Frequency distribution of the limitation generating disability by age groups and sex of a population with disabilities.
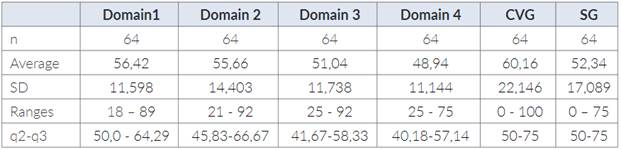
About the quality of life, the following results were found:
Domain 1.
Only for 15.62% of patients, physical pain does not prevent them from doing what they need to do, but 50% said that physical pain had limited them only a little.
On the other hand, the need for medical treatment to function in their daily lives, only 4.69% said they did not need anything. 34.38% said they need a little. 35.94%: said they need what is normal and 21.88% said they need a lot.
Furthermore, 81.26% of patients consider that they have enough energy for daily life.
Likewise, 45.32% of cases can move from one place to another, while 54.69% can only move a little. It was also found that 92.18% of the patients are satisfied with sleep, 73.44% admit satisfaction with the abilities to carry out daily activities and 26.56% report little satisfaction with the abilities to carry out daily activities.
Regarding the question satisfaction with their work: 7.81 expressed being not very satisfied, 45.31% normal, 37.50% quite satisfied, and 9.38% very satisfied.
Domain 2
Enjoy life: 87.5% of the cases admitted enjoying life in the different ranges, normal 42.19%. quite 43.75% and extremely 1.56%,to the question, how much do you feel that your life has meaning? 53.12% answered normally or quiet. 3.12% that extremely and 43.76% a little or nothing.
Additionally, the ability to concentrate is admitted as good and quite in 85.94% of the cases.
On the other hand, it was found that 59.38% accept their physical appearance, while 37.50% admit it a little.
Regarding self-satisfaction, it was found that 20.31% admit it little, 32.81% normal, 39.06% satisfied, and 7.81 very satisfied.
To the question, how often do you have negative feelings, such as sadness, hopelessness, anxiety, or depression? 64.06% indicated that they rarely experience it, 6.25% report never having experienced it. 25% report having done it moderately, while 4.69% did it frequently.
Domain 3.
Personal relationships: 96.88% said they were satisfied. showing this: Satisfaction with their sexual life: 76.56% of the cases describe dissatisfaction with their sexual; life while only 23.35% were satisfied. On the other hand, 95.31% of the cases are satisfied with the support received from their friends.
Domain 4.
About the question, how safe do you feel in your daily life? It was found that 46.88% feel only a little. 31.25% report feeling normal, while 20.31% quite a lot, and 1.56% feel extremely safe in their daily life.
Equally important, the Perception of an unhealthy environment was found in 60.94% of the cases, while 30.6% was normal and/or quite or extremely.
Next, in the availability of money for their expenses: 78.12% express the normal.
Furthermore, 62.49% of patients admit to having the information they need for their lives. 37.50% say they have a little.
Regarding leisure opportunities, in their majority, 93.74% of the cases admit it.
likewise, 90.62% of those surveyed are satisfied with their housing conditions.
On the other hand, regarding access to health services 89.06% indicate normal and quite satisfactory. Finally, the transport services in their area 89.06% indicate that they have normal and quite satisfactory table 5.
Discussion
The average age of the participants was 44.4 years old, but with a high range from 21 to 85, which shows that there is no predilection for disability for a given age group. Similarly, other studies have been reported 17)(18)(19.
About the sociodemographic variables where the male sex predominates, mostly single men. Results like those referenced by the Economic Commission for Latin America and the Caribbean (ECLAC) in 2012 (20) indicate a higher prevalence of the male gender in countries such as Colombia, Salvador, Guatemala, Honduras, and Mexico. Next, the educational level manifested by the participants of our study was 37.5% basic secondary similar to the data found in different studies carried out in Colombia 21)(10)(14)(22)(23.
In this study, disability prevails in men, which could be directly related to acts of violence or accidents as reported by DANE (14). However, other authors report that the majority are women 20)(23.
60% are affiliated to the Colombian health system with a distribution of 48.43% to the subsidized and 46.87% to the contributory. These results agree with those reported by DANE, RLCPD, and other authors 17)(14)(24 that do not coincide with who found in their series a higher percentage of the contributory regime. However, the proportions of belonging to socioeconomic levels one and two, if shown in agreement with this author and agree with the socioeconomic level with the highest percentage 25. Similar data are reported by the registry for the location and characterization of people with disabilities (RLCPD). The most prevalent economic activity is commerce with 46.87% of cases, they are self-employed and 67% do not have any type of contract. In accordance with our result 26 describes the economic activity as independent workers.
According to the registry of location and characterization of people with disabilities (RLCPD), when analyzing economic activity, it indicates that 80% do not have a labor contract, 64% have no income or earn less than five hundred thousand Colombian pesos per month, they cannot study due to situation disability, a situation similar to the findings of this characterization 27.
The work capacity of the study population is equivalent to 58%, they do not consider their disability condition as an obstacle to being productive, it should be noted that the majority have academic training, have a job. In several countries of the world, they increasingly recognize the enormous potential and its contribution to the economy that generating more employment for people with disabilities would lead to cuts in expenses for disability benefits and would collaborate to reduce poverty, but joint actions of governments to destroy barriers to achieve greater access and participation in the economy and society.
Besides, the fact of obtaining income from their work not only reports personal benefits but also improves their relationships with the social environment, being able to develop their talents and capacities to the maximum 27. In other studies, they describe that staff with disabilities are more productive compared to workers without disabilities, they found no differences in performance or the need for constant supervision 28.
This study showed that the vast majority of PwD did not have an employment contract and only 11% were professionals, contrary to the results of the study by 29)(4. Where the participants were mostly hired indefinitely, with undergraduate and postgraduate studies. The panorama of the type of labor relations in disability with fixed hiring has been decreasing and at the same time the employment rates are disproportionate according to the population according to the study of 3 due to the economic crisis that some countries are going through, This concept is related to our study where the population characterized in a high percentage does not have a formal contract and also the difficulty to access better-paid occupations.
The information regarding the disability classification in our study, the deficiencies in compromised body structures with a higher percentage (51.53%) of CNS diseases, is related to the data according to DANE 2010 (21.84%) compromising sensory organs and 17.14% structures of the movement the types of disability with 7813% physical and 17.18% visual. 61% consider that it was diagnosed promptly. 51% of the population does not require health care. 70% require the use of support elements; 30 in their study coincide with the data found, reporting the highest percentage of their population with disabilities still need special aids, prostheses, or permanent medications.
Regarding the results of the evaluation of ADL, 79% do not require help in their activities of daily living (ADL) also 84% do not currently attend rehabilitation and only 16% attend Physiotherapy and the cost is assumed in 89 % By others. However, 19 found that the executing entity for spending in a high percentage of rehabilitation processes is given by the General System of Social Security in Health and 80% of the population registered in (RLCPD) attends rehabilitation and the cost is assumed by the SGSSS 27.
Domain one, in general, obtained the highest score of 56.42 points, and the domain that showed the lowest perception was associated with the environment with 48.94% understood (security, education, leisure, housing, access to health services, and transport).
This is related to the study 19 who also report a low score in the population with spinal cord injury. while 24 present similar findings in the environmental domain and 31 found a very low dominance in the environmental factor due to low financial capacity and the most representative score in the social factor for support and assistance provided by the family. They also showed a better average score in the domain of interpersonal relationships and the lowest average in the environment by this study.
On the other hand, Orozco, et al. 32, describe the physical health domain as low and the environment domain as the highest, possibly these data are due to the type of disability associated with the pathology that compromises the individual's self-care and independence, for, Therefore, these results are contrary to those reported in this study.
Among the domain 1 sub-factors, 45.32% of the cases can move from one place to another, while 54.69% a little. Consequently, with the need for assistive products to be able to move around and the type of disability that is mostly physical. In domain3 on satisfaction with their sexual life, 76.56% of the cases describe dissatisfaction contrasted with 33 in their study they analyze male sexuality in terms of a man with motor disability, in the case of an injured medullary where he concludes “that changes must be made in the male representation associated with strength, virility and violence towards a more internal position and the search for ways of living sexuality that value the uniqueness of the experience, to the detriment of the models traditional”.
Additionally, Hess & Hough 34 attributes that relationship factors such as partner satisfaction, quality in the relationship are the most important predictors in a relationship than sexual satisfaction due to genitality in both men and women, concern for Not satisfying the partner is similar to the lack of personal satisfaction, the feeling of intimacy and the ability to please the sexual partner are determinants of their satisfaction.
A systematic review carried out by Aikman et al. 35 related to sexuality in women shows that in various aspects of sexuality there is a negative affectation in the case of spinal cord injury, sexual satisfaction decreases, affecting their quality of life, together with neurogenic bladder disorders and urinary incontinence. Additionally, physiological, psychological, and social changes influence sexual function, it is a permanent rehabilitation priority; social stigmas concerning disability and sexuality prevent a better approach 36.
Burgui 37 in her article analyzes the different environments in which human beings carry out their activities and how they impact on ecological, cultural, and socioeconomic factors in people's quality of life. In our research with the referent of the question, it is not specifically shown that it triggers the study population to think that their environment is unhealthy, since the other sub-factors have better scores, but it is about giving an explanation from the factors or components that They are part of this, and it is considered important for the integral development of the individual.
The limitations of the present study were the sample size and the search for people with disabilities who were working.
Conclusions
The main risk factors for the labor inclusion of a person with a disability are subject to sex, the type of disability, access to decent employment, and remuneration according to their potentialities.
The greatest impact on the quality of life about disability is given by the need to move from one place to another, to feel dissatisfaction with their sexual life and the perception of an unhealthy environment.
Recommendations
It is suggested for future studies to increase the size of the sample and promote, through the entities in charge, training for people with disabilities on the importance of participating in this type of research since its results may be important for the development of programs that allow promoting inclusion to the PwD.

