











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The Brazilian population has experienced the process of nutritional transition in the last decades, implying the need for transforming the organization of health practices 1) (2. In this context, two extremes share the same scenario: the vertiginous increase of overweight and the persistence of high frequencies of specific nutritional deficiencies 2.
To address this nutritional paradox, the National Food and Nutrition Policy (NFNP) proposes Food and Nutrition Surveillance (FNS) among its guidelines as a central element in the monitoring of the food and nutritional situation and as a support to political decisions aiming to improve health 3. The FNS consists in the "continuous descriptionand prediction of trends in food and nutrition conditions of the population and its determinants" 3. It includes different strategies such as population surveys, nutrition calls, research and scientific production funding 1) (2) (4) (5.
In order to overcome limitations related to the high cost and poor representativeness of population surveys and nutritional calls, which limit health and nutrition policy subsidies, the Food and Nutrition Surveillance System (SISVAN) was established as the basic instrument of the FNS in the decade 19902. The SISVAN represents a system of data collection, processing and continuous analysis that allows to know the nutritional situation of the population served by the Unified Health System (SUS) 6) (7. With the creation of the Familt Grant Program in 2004, the SISVAN became the main provider of information on the health of beneficiary families 2.
In an attempt to overcome some limitations of the System and integrated with the new technological times, the implementation of SISVAN-Web was suggested in 2008 as a computerized system of Primary Health Care (PHC) replacing the SISVAN Municipal Module 8) (9) (10. This new system allows the registration of food consumption and anthropometric markers (based on current references) through an interface that facilitates its use by users 11.
Recent literature review pointed out the lack of studies on SISVAN in the scope of the Family Health Strategy (FHS) 12. Furthermore, few studies have paid attention to the quality of the information collected to feed the system 13. However, assessing the SISVAN is important for guiding the NFNP and the subjects involved with it (public managers, health professionals and target population) 9.
Focusing on the SISVAN-Web, this study aimed to evaluate the reliability of anthropometric data of under-five children, describe the coverage of the System and know aspects of the implementation from the perception of managers.
Methodology
Research scenario
The study was conducted in the context of FHS in two municipalities in the state of Paraíba, Brazil, selected for convenience. The choice of municipalities considered similarities of geographic position (location in the metropolitan area of the state capital with access to the available network of services), degree of urbanization (almost 100%), demographic-social indicators (average human development index - 0.748 in a municipality 1 and 0.649 in the other one) and traditional organization of PHC (almost 100% of the population covered by the FHS). The municipalities have a population of 4,596 and 7,862 under-five children, with 19 FHS teams and the other with 28 teams, respectively.
Sampling plan
The sampling plan aimed at the inclusion of 314 randomly selected under-five children (157 from each municipality) from 18 FHS teams (nine from each municipality that corresponded to about half of the teams of a municipality and 1/3 of those of the other municipality). This calculation was established in the larger research from which the results of the present study are part, which evaluated the implementation of feeding and nutrition actions in the FHS and their relation with the quality of care. The SISVAN-Web analysis was one of the objectives. A study developed in the municipality of Montes Claros (MG) 14 indicated a higher proportion (58.1%) of negative evaluation of health services provided by FHS teams formed by physicians and nurses without residence in Family Health compared to the proportion (41.9%) of the teams composed by professionals with this training. Based on this, it was necessary to observe 157 children in each of the municipalities of Paraíba, considering the expected proportion of the negative evaluation of the health services by the users of 41.9% in the municipality with a better human resource situation of health professionals and 58.1% in the other, with 95% of confidence level, 80% of power, 10% of increase to compensate for possible losses and design effect of 1.2.
Data collection
Data collection was carried out in health facilities between July and December 2014. The field team was formed by professionals and students of the health area. The quality control of the study included: training and standardization of interviewers, use of the Instruction Manual, pilot study and supervision. In order to train the anthropometrists, the recommendations for PHC of the Ministry of Health were adopted 15. Data collection includes the measurement of the children's weight and height, consultation with the SISVAN-Web to verify the individuals monitored by the System, the quantification of beneficiaries of private health plans and of those who use the public health service, and the application of a questionnaire to the managers responsible for the System.
Anthropometric data were obtained from children scheduled for childcare consultations on the day of data collection, on a typical work day. It was established that each child included in the study would be measured in three situations:
- by health professionals with the use of the available equipment in the health units, respecting their work routine;
- by the anthropometrists of the research using their own equipment, considered of adequate reliability (standard gold measure);
- by the anthropometrists of the research using the equipment of the health units.
The measures obtained by health professionals were collected directly from the medical record or from the Child Health Handbook, after the consultation. At the time, the child's birth date was also noted, and later used to calculate age in the date of the interview.
The anthropometric evaluation by the anthropometrists of the research was performed after the consultation, in order to avoid the observation of the procedures used and interfere with the work of health professionals. All measures were obtained by a single pair of anthropometrists, one of which would be in the auxiliary function, following training standards. Children were measured and weighed twice, with the researchers' own equipment and with those available at health facilities. The average of the two measurements was used in the registration in a specific form for this purpose. Children under 24 months of age had length measured in dorsal decubitus. Children aged 25-60 months had the height measured in orthostatic position. Height corresponds to the set of measures of length and height. All children were weighed in light clothing. In children younger than 24 months of age, weight was obtained by the difference between the weigh of the mother with the child in her lap and the value of the mother's weight.
Research equipment were: child anthropometer made of wood with amplitude of 130 cm and subdivisions of 0.1 cm, stadiometer (WCS®) with amplitude of 200 cm and subdivisions of 0.1 cm and electronic platform-type scale with capacity for 150 kg and graduation in 100g (Tanita UM-080®). The equipment of the health units were used in the same conditions by assistance professionals and research anthropometrists.
For the three study situations, the Z-scores of Weight/Age (W/A), Body Mass Index/Age (BMI/A) and Height/Age (H/A) were calculated using the Software WHO Anthro 2009, considering the population of the Multicentre Growth Reference Study as reference 16. The categories of nutritional diagnosis of overweight for age (W/A > 2 Z-score), overweight (BMI/A > 2 Z-score) and stunting (H/A < -2 Z-score) were considered 15.
The municipal coverage of SISVAN-Web for the total population and per life stage (children aged 0 to 4 years, children aged 5 to 10 years, adolescents, adults and the elderly) was calculated based on the totals of individuals monitored, obtained directly in the System, and the number of users using the public health service, estimated by the difference between the number of inhabitants of the municipality and the number of beneficiaries of private health plans. The 2010 demographic census 17 was used as data source of the number of inhabitants in the municipality. Also related to 2010, information provided by the National Agency for Supplementary Health Services made it possible to identify the total number of individuals by age group and sex linked to private health plans 18.
The total coverage was defined as the percentage of individuals, from all life stages, monitored by SISVAN-Web in the health units in 2010. Total coverage was estimated by dividing the number of records of nutritional status of individuals followed in 2010 by the approximated population that used public health services. The same calculation was performed to obtain SISVAN-Web coverage for the different life phases considered in the study.
In order to analyze aspects of the implementation of SISVAN-Web, a questionnaire was applied to the managers responsible for the System in both municipalities. The questionnaire addressed data related to the profile of these managers responsible for feeding the system and transferring information (education and training for implementation of the System), ease of use (user interface, information structure, navigation, search system efficiency, loading time of data files, feeding and flow) and the use of information (reliability: use of protocols, coverage: focused on vulnerable segments or in all life cycles; origin: data exclusive of the health sector or population-based data; nature: anthropometric and/or food consumption data; and intersectorial character: restriction to demands of the health sector or coverage to other sectors such as food security, Family Grant Program and school diet).
Data analysis
Data were organized in spreadsheets and typed in double entry. The Validate applicationof the Epi Info Software version 3.3.2 was used to analyze the consistency of the data.
Three types of comparisons were made in order to test the reliability of anthropometric measurements:
- inter-equipment, considering the measurements obtained by the research team using their own equipment vs. the measurements obtained by the research team using the service equipment;
- inter-examiners (anthropometric techniques), considering the measurements obtained by the research team using the service equipment vs. the measurements obtained in the routine of the service;
- inter-examiners and inter-equipment, considering the measurements obtained by the research team using their own equipment vs. the measurements obtained in the routine of the service.
A t-test to paired samples was applied to verify the difference in means of weight (kg) and length/height (cm) in the three situations. In order to know the degree of agreement between nutritional classifications, the classification obtained by the research team using their own equipment was used as the "gold standard" to comparisons with the other two classifications. The degree of agreement was verified through the Cohen's Kappa Coefficient. Landis & Koch' criterion was used for interpretation of the agreement [19].
The level of significance adopted was 5%. The Software Stata version 12.0 was used.
Ethical aspects
This study was approved by the Research Ethics Committee of the State University of Paraíba under protocol number 19689613.3.0000.5187. All participants signed an Informed Consent form.
Results
A total of 319 under-five children were examined for anthropometric evaluation, 152 from one municipality and 167 from the other. However, the pairing of anthropometric data obtained by the research anthropometrists with their own equipment was possible for 266 cases on weight and 286 on length/height, when they used the equipment of the health services. For data obtained by health professionals, pairing was possible for 132 cases on weight, and 137 cases on length/height. Losses in the first situation were due to the lack or poor quality of anthropometric equipment in some health units. Losses of data obtained in the service were due to lack of measurement and/or lack of registration of measures (our study did not intervene in the work routine). It is important to highlight that the number of children analyzed vs. losses per municipality did not differ with respect to nutritional status.
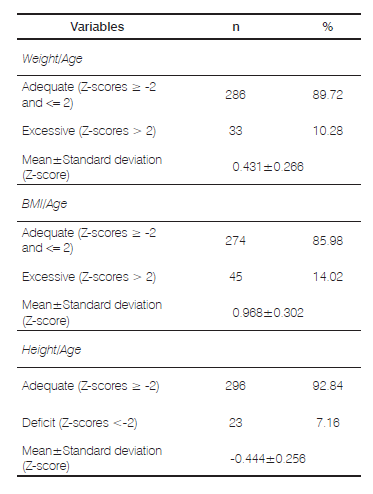
Table 1 presents the description of the anthropometric status of the study sample. The prevalence of overweight for age, overweight and stunting were 10.28%, 14.02% and 7.16%, respectively. None of the children were diagnosed with weight-for-age deficit (Z-score W/A < -2) nor with weight deficit (Z-score BMI/A < -2).
Table 1 Description of anthropometric status of under-five children living in two municipalities in the state of Paraíba, 2014.
When analyzing the measurements obtained with the equipment of the health service, it was observed that health professionals obtained smaller values of weight and height in 540 g and 3.17 cm, respectively, being these differences statistically significant. Similar results were found in the measurements of the research anthropometrists with their own equipment in comparison to the ones that they obtained using the equipment of the service (Table 2).
Table 2 Differences in the measurement of weight and length/height of under-five children assisted by Family Health Strategy health teams of two municipalities of Paraíba, according to the origin of the measures, 2014.

P = Measurement obtained by the researcher using high reliability equipment (gold standard measure).
PS = Measurement obtained by the researcher, using the equipment of the service (the same used in "S" by the professional of the health unit).
S = Measurement obtained in the routine of the service.
Table 3 shows the agreement between classifications of the nutritional status of the children according to anthropometric evaluation of the research anthropometrists with their own equipment (gold standard) with the other two classifications. It was noticed that lower agrrement values were found for classifications related to the measurements obtained by the health professionals, being worse for H/A (Kappa Coefficient = 0.38) and BMI/A (Kappa Coefficient = 0.39). Health professionals overestimated overweight and stunting. When the parameter was the equipment, substantial agreement values were obtained for the three anthropometric indices, being higher for H/A (Kappa Coefficient = 0.74).
Table 3 Agreement between anthropometric classifications of under-five children assisted by Family Health Strategy teams in two municipalities of Paraíba, according to the origin of the measurements, 2014.

P |
= Measurement obtained by the researcher using high reliability equipment (gold standard measure). |
PS |
=Measurement obtained by the researcher, using the equipment of the service (the same used in "S" by the professional of the health unit). |
S |
= Measurement obtained in the routine of the service. |
The coverages of SISVAN-Web were 2.8% and 3.3%. In both municipalities, higher coverage values occurred among children, being 6.5% and 10.1% in the 0-4 year age range and 8.4% and 7.1% for 5-10 years. The elderly presented the lowest coverage, of 0.3% and 0.7%. Among adolescents, coverage was 2.1% and 1.8%; and among adults, 2.3% and 2.2%.
Regarding the answers of SISVAN-Web managers, it was verified that both municipalities had one single person responsible for feeding and transferring information, and this person had complete secondary education and was not trained for the implementation of the System. Regarding ease of use, the efficiency of the searching system was the only aspect perceived as bad by one of the managers. Regarding the use of information, the two managers reported not using protocols, approaching all life cycles, being based exclusively on health care services and restricted to the demands of the health sector. The use of anthropometric data and food consumption was pointed out by one of the managers, while the other pointed exclusive use of anthropometry.
Discussion
Generally, this study indicate several limitations in relation to the SISVAN-Web, such as poor structure, low coverage, lack of integration with other systems and low reliability of anthropometric measurements. This indicates little progress since these factors are highlighted in the literature prior to the implantation of the computerizations of the System 4) (5) (8.
According to Cohen's Kappa coefficients, the results obtained indicate errors in the nutritional classification, due both to the techniques used by health professionals and to problems of the equipment available in the services. This reality compromises the SISVAN-Web information. The diagnosis of insufficient linear growth (smaller values of stature) becomes overestimated, which is reflected in higher values of BMI/A (greater chance of being overweight). Low agreement between anthropometric measures obtained in the basic health network have also been reported by other researchers 13) (20) (21. In this study, failure to observe the procedures adopted by health professionals makes it impossible to specify deficiencies in measurement techniques. However, the diversity, poor positioning and lack of calibration of instruments available in the health services were problems detected that may be related to the observed variations, which coincides with previous reports 20.
The results of the present study revealed very low coverage, similar to those found in other localities 1) (2) (9, and against the increase in the number of follow-ups suggested after computerization of the SISVAN 4. These findings are reason for concern, especially considering the importance of the System for decisions, programs and policies related to nutrition actions, including those related to the promotion of healthy food practices and the management of the Family Grant Program 3) (22.
Regarding the population coverage in the different phases of life, the highest coverage recorded among children and the lower among the elderly coincides with the results of a national survey4 and of more recent studies 1) (2. This situation may be related to the historical priority of child-centered surveillance 5) (22).Despite the positive consequences derived from this finding, i.e. favoring the care of children who are biologically vulnerable, ignoring the elderly population limits the care to a group that has increased proportionally in the population and who presents significant risks of infectious, deficiency and chronic diseases 1) (23.
The lack of training to implement the SISVAN-Web of those responsible for feeding the system and transferring information in the municipalities of the current study has been previously reported by professionals who carry out similar actions 9. The need to promote professional training and retraining is, therefore, encouraged so as to improve the reliability of the information generated by the System 1. The non-use of protocols, indicated by the managers interviewed, can also be detrimental to the credibility of data 4) (22. It is necessary that the guiding documents of the SISVAN actions 10) (11) (15 be available in the health services and be known and used, which does not seem to be the reality in the country 22) (24. More favourable situation was found in Minas Gerais, where 68.6% of those responsible for the System indicated to use technical documents of the Ministry of Health 25.
In general, the managers' perception of ease of use is indicative of good handling of SISVAN-Web. This result is consistent with the proposal of computerization of the System and the need for a friendly user interface 2.
As verified in Belo Horizonte 9, the non-use of food consumption data was indicated in one of the municipalities of the current study. In Minas Gerais, the registry of this information was informed by only 1/3 of those responsible for the system 25. This situation is worrisome due to the importance of knowing food consumption data to subsidize the implantation and development of nutritional interventions 26, especially in the current situation marked by major changes in the food pattern associated with social transformations of modern life 3. These changes include increased consumption of processed foods in detriment of fruits and vegetables, with possible negative effects on children's health, which demands the implementation of actions to promote healthy eating 3) (27.
The NFNP suggests the issue of food and nutrition be addressed through the articulation of health with other sectors, such as education and social assistance, and programs, such as the Family Grant Program, in a way that will break the history of overlapping and disarticulated actions 3. However, the report of information generated by SISVAN-Web restricted to the health sector was rather observed in the present study, likewise the observed in Minas Gerais 26. It is necessary to recognize that the concretization of intersectoriality is related to the historical process of strengthening and expanding the concept of food and nutritional security, in a conjuncture of governmental integration with civil society and technical levels 3) (27.
The prevalence of overweight and stunting found in this study is in line with the findings reported in a meta-analysis of samples from public health services 28. Another study that also focused on SISVAN presented similar results 13. Despite expressive prevalences that reveal the importance of monitoring the growth of children assisted in public health services, many of them did not have their weight and/or height measured in the current study, which converges with results of previous studies 20) (29. Possible characteristics of professionals associated with this situation such as training, skills and motivation 13) (29, were not analyzed in this study.
The limitations of this study are related to the caution to extrapolate the results, as they represent the reality of two municipalities only. Furthermore, information related to managers may involve information bias. However the results are important considering that research about the validity and accuracy of measured anthropometric data is lacking. The accuracy of anthropometric data is critical to produce robust and interpretable findings. Future researches are important to identify the provision of appropriate training and assessment as essential for health professionals responsible for collecting routine data.
Conclusion
This study allowed us to illustrate problems arising from the reliability of anthropometric data of under-five children obtained in public health services, low SISVAN-Web coverage, and restrictions on the use of information from the System in two municipalities in the state of Paraíba. It is necessary to invest in structure and human resources with a view to the adequate the operationalization of SISVAN-Web and monitoring of nutritional status. These arrangements are fundamental for the planning, management and evaluation of food and nutrition actions under the PHC in the municipalities studied. Further evaluative studies of SISVAN-Web are necessary for its improvement and for the implementation of NFNP guidelines.

