











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Contextualization of carious lesions
Dental caries is an important oral health problem in most industrialized countries, affecting 60-90% of schoolchildren and the vast majority of adults. The earliest manifestation of the decay process is a small patch of demineralized (smoothed) enamel on the surface of the tooth, often hidden from view in the fissures (grooves) of the teeth or between the interproximal surfaces. The destruction extends to the softer part. The weakened enamel collapses to form a cavity and the tooth is progressively destroyed. Cavities can also attack the roots of the teeth if they are exposed by the gum recession of the gums. This is more common in older adults.
Dental caries caused by the action of acids on the surface of the enamel. The acid is produced when sugars (mainly sucrose) in foods or beverages react with bacteria present in the dental biofilm (plaque) on the surface of the tooth. The acid produced leads to a loss of calcium and phosphate from the enamel; this process is called demineralization. The main treatment option for a dental cavity is to perforate caries and place a restoration made of several materials (e.g., composite resins, and other filling materials). Extensive tooth decay may require a crown, root canal treatment or even tooth extraction [1].
Therefore, since 1975 the chemical and mechanical removal of caries was introduced, countless studies have been carried out including a recent study showing the usefulness of papain [2]. Therefore, this article aims to show the development of an innovative chemical formulation for the Atraumatic Restorative Treatment (ART) of the carious lesions carried out in a Clinical Dentist located at Bogotá DC-Colombia.
THEORETICAL BASIS
Types of cavities
Dr. G.V. Black (1836-1915) developed a system to classify carious lesions according to the type of tooth affected (anterior or posterior tooth) and the location of the lesion (for example, lingual, buccal, occlusal, etc.). The six kinds of carious lesions are.
Class I: Cavity in pits or fissures in the occlusal surfaces of molars and premolars; Facial and lingual surfaces of the molars; Lingual surfaces of the maxillary incisors (Class I corresponds to the surfaces of a posterior tooth that can be seen clinically: occlusal/lingual/ buccal surfaces, therefore, the interproximal surfaces are not classified as Class I).
Class II: a cavity in the proximal surfaces of the premolars and molars (class II corresponds to the surfaces of a posterior tooth that cannot be seen clinically).
Class III: Cavity in the proximal surfaces of the incisors and canines that do not involve the incisal angle (Class III corresponds to the surfaces of an anterior tooth that cannot be seen clinically).
Class IV: Cavity in the proximal surfaces of the incisors or canines that affect the incisal angle (the Class IV lesion is the largest version of Class III that covers the incisal angle).
Class V: Cavity in the cervical third of the facial or lingual surfaces of any tooth (think of the neck of the tooth).
Class VI: Cavity in the incisal edges of the anterior teeth and tips of the cusp of the posterior teeth (Class VI corresponds to the upper surface of a tooth) [3].

Classification of caries according to its severity
The appearance of interproximal caries can be classified as incipient, moderate, advanced or severe, depending on the amount of enamel and dentin involved in the caries process.
Incipient: a lesion that extends less than half of the enamel.
Moderate: a lesion that extends more than half of the enamel, but does not involve the dentin-enamel junction (DEJ).
Advanced: an injury that extends to or through the DEJ but does not extend more than half the distance to the pulp.
Severe: an injury that extends through the enamel, dentin and more than half the distance to the pulp.
The above can be seen in the following figure:

Caries removal techniques
Dental caries is an infectious microbiological disease of the teeth that results in localized dissolution and destruction of calcified tissues (figures 3 and 4).

Figures 3-4 Dental caries covers and infect four surfaces; these are the outer layer, the translucent zone, the opaque zone, the area of the body of the lesion, which we will enunciate respectively. Modified from Hinestroza et al. [4].
Dental caries can be controlled by what is known as "non-invasive" methods, which include thoroughly cleaning the plaque of the teeth, recommending a healthy diet and using fluoride to prevent cavities from getting worse. If the decay progresses, it is possible that these "non-invasive" techniques should be combined with "invasive" management, which consists of removing carious tissue and restoring teeth where the cavities caused by caries impede cleaning. The dental operation will improve the appearance of the teeth and allow the patient to clean them.
Traditionally, dentists have removed all caries with a rotary instrument (burr) before placing a filling. However, the elimination of all caries has some disadvantages, which include damage to the tooth nerve, toothache and possibly weakening of the tooth structure. This method is known as complete caries removal in one-step. Despite a large amount of restorative material placed around the world on a daily basis, dentists still do not know what is the best "operational management" strategy for dental caries. Three alternative surgical interventions for the management of caries have been evaluated comparing them with the traditional treatment of removing all caries at once (removal of complete caries). These interventions were.
- Step-by-step removal: this technique eliminates caries in stages during two visits a few months apart, which allows the dental pulp to be repaired and dentine deposited.
- Partial elimination of caries: the dentist removes part of the dentinal cavity and sees what remains in the tooth permanently.
- Operative dentine is not removed - tooth decay is not removed before sealing or restoring.
It was found that when the complete caries extraction technique was compared with the stepped excavation, the pulp or nerve of the tooth would have been exposed in 347 out of every 1000 teeth treated with complete caries removal, whereas when the technique was used step excavation, this has happened in only 154 teeth per 1000.
When the technique of partial removal of caries was used, it found that the pulp or the nerve would have been exposed in 50 teeth out of every 1000 treated. However, when the complete caries removal technique was used, this figure would have been 219 teeth per 1000 treated.
There was less damage to the nerves when part of, or all of the decay was left behind, both for the baby's teeth and for the adults. There was no difference in the number of teeth with toothache with any of the techniques. One of the dentin-free caries removal techniques required fewer replacement fillings, although no differences were found when comparing any of the other techniques to complete tooth decay.
In the included studies, mainly specialized dentists placed the fillings and the teeth were followed for a relatively short time (1 year). More studies are needed to help answer more questions. Non-specialized dentists to verify if the results would be similar should perform future studies. These studies should follow patients for long, check if there is any difference in toothache, more cavities, and fill replacements. They should also check what techniques patients prefer and if there is a long-term difference in cost [5].
Traditional caries removal techniques generally include the use of high, low-speed hand pieces, and manual cutting instruments. The advancement of the diagnostic systems has achieved a more precise knowledge of the caries process, improved materials, cutting instruments and new removal techniques with a minimum invasive approach. A minimally invasive criterion in the treatment of caries emphasizes the conservation of healthy tooth structure and can minimize the replacement cycle of the initial restoration.
Minimally invasive dentistry
The term Minimally Invasive Dentistry (MID) can be defined as the management of caries with a biological approach instead of surgical, which is more related to traditional dentistry.
The golden triangle of the MID is constituted by:
The histology of the dental substrate that will receive treatment.
The chemistry and manipulation of the adhesive materials used to restore the cavity
The considerations of the operative techniques available for the selective elimination of caries.
This current integrates concepts of prevention, control, and treatment, including the detection of early lesions, the identiication of risk factors (risk assessment) and the establishment of prevention and education strategies for the patient's health. When the effects of the disease are present, in the form of a carious lesion, therapeutic strategies with less invasive solutions are required [6].
Atraumatic restorative technique
On the other hand, and as it is normal to be in this type of techniques, we have to say that there are some cases in which its use is not recommended, especially in this case in those patients who have pulpal problems, or in whom the Caries is not accessible with manual instruments, as well as in the case that the caries is located on the proximal surfaces of the adjacent tooth. This is a technique that stands out due to the low cost it has, and because it is a very simple and painless intervention, which is carried out under the modern concept of minimal cavitation preparation [7].
Mechanical, chemical removal
The chemical-mechanical removal of caries part of the minimally invasive dentistry stream is based on the action of a chemical agent that softens the dentin altered by the action of the carious process, denatured and infected and that is complemented with a mechanical removal by means of non-cutting manual instruments [8].
This technique has been shown to decrease the risk of pain due to the selective elimination of caries. In general, a chemical agent for the removal of caries must be able to cause a greater degradation of collagen partially degraded by the action of bacteria. This is achieved by the rupture of the non-covalent bonds of the triple helix in collagen structure, the mentioned phenomenon generates that the application of chemical agents such as caries removers does not act on the intact collagen but they dissolve only the dentin that is altered allowing the selective removal of it. More recently, proteolytic agents such as papain can be used to further degrade the partially demineralized and altered dentin matrix that has been previously exposed to bacterial action (infected dentine), which facilitates its elimination and prevents damage to the underlying rem-ineralize tissue (affected dentin) [9].
Papain is an endoprotein similar to human pepsin, which has bactericidal, bacteriostatic and anti-inflammatory activity, from the latex of the leaves and fruits of the ripe green papaya, Caricapapaya, cultivated in tropical countries such as Brazil, India, Ceylon, South Africa and Hawaii [10].
Papain interacts with collagen exposed by the dissolution of dentin minerals by bacteria, which makes infected dentin softer, allows its extraction by means of non-cutting instruments and dispenses, thus the use of anesthesia and rotary instruments. The degraded part of the collagen of decayed dentine is chlorinated by chloramine and is easily removed with the excavator. That is to say, that this auxiliary formulation is used to chemically soften decayed dentin, as well as, the degraded portion of the collagen of decayed dentin is colored by the solution used in the chemical and mechanical removal of caries. This coloration affects the secondary and/or quaternary structure of the collagen, breaking the hydrogen bridges and facilitating the removal of decayed tissue [11].
On the other side, Dragon's Blood is an important ethnobotanical medicine that is common in South America and Latin America. Dragon's blood has an anti inflammatory action due to the taspine alkaloid from the dragon's blood that was irst documented in 1979. Later studies conirmed these actions, leading to further studies in the area of wound healing. In one study, Oil-based was found to be the cicatrizing active principle of an in vivo test in mice; increase migration of human ibroblasts was suggested as the probable mechanism in this acceleration of the wound-healing process. The most well-known source of Dragon's Blood is Croton lechleri, ranging primarily from the rain forests and low mountains of Colombia and Ecuador to Bolivia. C. lechleri resin and bark are used in traditional medicine in South America. Externally, it is employed, as a wound-healing agent. Dragon's Blood also cleans the wound by killing bacteria, microbes and other junk with its antiseptic properties, helps take the pain away, helps the wound heal faster, helps lower inflammation and stops the bleeding. Dragon's Blood may be able to help with receding gums and dental health [12].
New formulations have been introduced that add some other enzymes, for example, in Mexico, containing papain and bromelain (enzyme extracted from pineapple fruit) has been distributed since 2013, and in 2016 it was marketed in Argentina based on papain which, unlike its conventional presentation, is bio encapsulated, which gives it greater stability and increases enzymatic activity [13], in addition to other more recent products based on papain and clove oil [2].
For this reason, this article aims to address a new formulation of a dental gel for the chemical removal of dental caries based on the use of an active ingredient and a phyto-therapeutic extract: Papain and Dragon's blood respectively.
MATERIALS AND METHODS
Materials
Relative insulation: (roll cotton), small round cavity cutter, # 5 teaspoon, dental gel, final filling material: 37% orthophosphoric acid, adhesive, and resin.
Methods
Procedure in a 20-year-old patient. The procedure for tooth decay in tooth # 22. It is done by isolating the area with rolls of cotton, spoon # 5. The Gel product is applied. In pits and pigmented fissures, in carious tissue. For three minutes. The mechanical removal of the contaminated gel is carried out. Pigmented and softened tissue is observed, the Gel is applied again for two minutes, until finding no pigmented tissues. The entire gel is removed with # 5 teaspoon, water is applied under pressure, no pulpal protection is applied and it is dried with a cotton swab and dry air.
The filling process is started by placing at the marginal edges of the cavity, demineral-ized with orthophosphoric acid, for 10 seconds, the cavity is washed with water under pressure. It is dried with a cotton swab, proceeds to apply the Bis GMA obturation material. It is polymerized and the resinous adhesive material is applied. After the final polishing occlusion control is done.
Product development
The qualitative composition of the product
This new product developed into the Fundación Científica 7 in Bogotá-Colombia is basically made up of papain as follows:
Basic Formulation
Table 1 Ingredients with an international denomination (INCI).
| Formulation ingredient | Amount (%w/v) |
|---|---|
| Water | Q.S. |
| Carbomer | Q.S. |
| Triethanolamine | G.967% |
| D-glucono-1,5 lactone (and) calcium Gluconate | G.483% |
| Croton lechleri resin extract | Q.S. |
| Papain | Q.S. |
| Sodium benzoate | G.483% |
*Observations on New Gel Dental Product.
Manufacturing: the formulation of the gel is conceived with the use of a carbomer and its respective stabilizer, which is triethanolamine, the set of these two, and the manufacturing protocol allows obtaining the gel cosmetic form, which is the vehicle of addition for the active principle of papain.
Quality control: tests made in bulk production and finished product correspond to physicochemical parameters (density, pH, viscosity, among others).
Actives agents
Active principle: Papain; debridant, anti-inflammatory, not damaging healthy tissue, accelerating the healing process.
Papain is a proteolytic enzyme, extracted from the latex of leaves and fruits of the adult green papaya (Caricapapaya) (see figure 5).

At the beginning of treatment with papain, there was an increase in the local secretion, softening of the necrotic tissue, detaching the edges of the lesion and a small increase in its diameter (halo of hyperemia). After a certain time, the necrotic tissue detaches and a rapid and gradual decrease in the halo of hyperemia occurs, accelerating the healing process, thus decreasing the recovery period of the lesions in patients using the enzyme papain. It acts on the injured tissue due to the absence of a plasmatic anti-protease, a1-antitrypsin, which prevents its proteolytic action in tissues considered normal. The a1-anti-trypsin inhibited the digestion of proteins, therefore, as the infected tissue does not present a1-antitrypsin, papain acts by "breaking" the collagen molecules partially degraded by the action of caries, since the It has the capacity to digest dead cells [15].
Dragon's Blood (Croton lechleri)
It is a tree native from Peru. The latex Croton palanostigma contains among its main components, an alkaloid called taspine. It also contains pyridone, aporphine, quinoline and the SP-303 principle, which is an oligomer substance with antiviral action. Dragon's blood is the name given to popularly exuding latex by tearing the bark of some tropical plant species. It is a viscous liquid, blood red, and astringent taste. It has chemical components that provide therapeutic properties against various diseases, such as diarrhea, ulcers and wound healing [16].
Previous studies have shown important chemical and pharmacological properties of the dragon's blood sap, as anti-inflammatory [17], healing [18], anticancer, antifun-gal, antiviral and antibacterial. In previous work, it was shown that the dragon's blood (Croton lechleri) at the 100% concentration had an inhibitory effect in vitro on Streptococcus mutans, producing an average inhibition halo of 11mm. Likewise, the dragon's blood at the concentration of 75% had an inhibitory effect in vitro less than the 100% concentration on Streptococcus mutans producing average inhibition halos of 8mm. This strain proved to be sensitive in vitro to Croton lechleri latex in concentrations of 75% and 100% [19]. The suggested use in Dental teets: 5 to 10 drops in a little water as a mouthwash or place directly on a toothbrush for natural toothpaste [20].
DESCRIPTION OF THE CASE REPORT
The new dental gel developed and performed at Clinical trials in patients by one of the authors (O. Bustamante) of the Scientiic Foundation Seven, has been used successfully in 84 patients who presented different carious lesions. To illustrate the use of this product, a case study is shown, performed on a 20-year-old female patient who attended the dental clinic with caries disease. We searched with standardized procedures, the removal of the carious lesion.
Observed characteristics
The patient does not report pain or postoperative sensitivity in control at 8, 15, 30 days and a year. No lucid, apical radio zones are observed.
During the clinical examination, in addition to the evidence of active caries in other regions, the presence of two extensive lesions of caries on the occlusal surface of the teeth was detected.
Clinical procedure
Figure 6. Carious injury, figure 7: application of new dental gel product, figure 8: caries removal, figure 9: demineralization, figure 10: sealing with resin and polymerized polished.

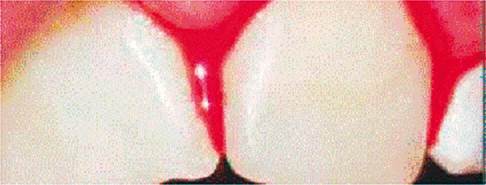
Figure 6 Carious lesion: pit and fissure in the palatal area of tooth 22 (left lateral incisor). B with a depth of the carious tissue in 1.5 mm pit.

Figure 7 Application of the new dental gel: with a small round bur, an opening of 2 mm was made in distal meso direction. The gel was placed for a time of 2 mm.

Figure 8 Removal of Carious Tissue: Mechanical removal of the carious tissue proceeded. The carious tissue was cleaned. The cavity free of carious tissue was observed, profusely washed with water and air for 5 minutes.

Figure 9 Demineralization: 37% orthophosphoric acid was placed on the marginal surface of the cavity for a period of 30 seconds. It was washed profusely, dried with cotton swabs until a whitish surface was observed.

DISCUSSION
The dental clinic into the C7 Scientific Foundation is the first Colombian laboratory to innovate in the development of products for the permanent treatment and removal of dental caries in the Colombian population. Based on the research and development generated so far, we have worked with this product. The label contains the following information for patients who require this product:
New Dental Gel Product
Oral gel with papain and Dragon's blood is a product for the hygiene and care of teeth and gums
How to use: Apply on teeth and gums, leave on for 5 minutes and rinse
Precautions: Recommended for children over two years, with adult supervision, do not expose to high temperatures. Keep in a cool and dry place. Keep out of reach of children. If you observe an adverse reaction, discontinue use and consult your dentist.
This new dental product is made of papain, which is an endoprotein present in the latex of the leaves and fruits green or ripe, of the Carica papaya, is interesting because it is similar to the human pepsin that has antibacterial, bacteriostatic and anti-inflammatory activity, accelerating the healing process once the decay in the affected area is removed [21].
To ensure that papain has a complete antibacterial, bacteriostatic and anti-inflammatory pharmacological activity, the maximum permitted the concentration of papain, i.e. 10%, should be used.
This innovative product also contains Dragon's Blood that is shown that can help protect and even heal teeth from cavities [22]. It is also interesting to note that it is used in the treatment of Gums with infected cavity [23].
These treatments combining dragon's blood with papain actives, resulting in an analgesic/ fast anti-inflammatory effect and in addition to these effects we observe the removal of dental caries, disappearance of edema, bleeding and gingival redness [24, 25] and figure 11.
This is a report that mentions that the dragon's blood supports collagen formation and exhibit wound healing and anti-inflammatory effects. In fact, the dragon's blood preserved the membrane of all cells and the functional viability of periodontal ligament cells [22].
This is a report that mentions that the dragon's blood supports collagen formation and exhibit wound healing and anti-inflammatory effects. In fact, the dragon's blood preserved the membrane of all cells and the functional viability of periodontal ligament cells [22].
In comparison to the irst formulations developed, does not contain chloramine because it has been shown over time and with the use of papain that it also has bacteriostatic and bactericidal properties inhibiting the growth of gram-positive and gram-negative organisms [26], and for which it serves to chemically soften decayed dentin.
It should be remembered that this innovative procedure is called the procedure called Atraumatic Restorative Treatment (ART) is based on excavating and eliminating tooth decay using only manual instruments, and then sealing it, looking for a form that would not be painful for tooth removal. It is interesting this procedure used mechanical chemical removal uses an enzyme (proteolytic, bactericidal, anti-inflammatory), or papain, which removes irreversibly carious tissue without action on healthy dentine (selectivity). This action complements the ART technique, giving it optimal efficacy. It can also be used in the entire population to be selected, in addition to promoting chemical debridement, granulation, and epithelialization, which accelerates the healing phases.
This mechanical, chemical method avoids the use of rotary instruments with strawberries and the application of local anesthesia are considered critical procedures, since they can cause fear and anxiety due to unpleasant experiences associated with the use of the needle and fear of the unknown [27, 28], with the advantage of a better acceptance for the treatment of the patient.
The importance of working with papain lies in the elimination of carious dentin present in cavitated carious lesions without pulp involvement. It is very innovative this method is performed without the use of anesthesia and without complaint of pain, promoting the patient a positive dental experience with minimal intervention and maximum preservation of healthy tooth structure.
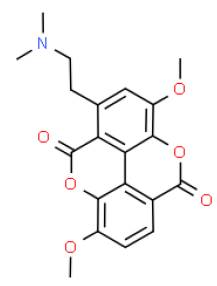
The papain acts only in the injured tissue since it does not possess the plasmatic anti-protease, alpha1-antitrypsin, responsible for the digestion of proteins in healthy tissues. In damaged tissues, papain acts by "breaking" collagen fibers partially degraded by the action of caries, as it has the ability to digest dead cells. Similarly, the beneficial effect of dragon's blood on wound healing was observed. The beneficial effect of the dragon's blood on wound healing was observed. This is due to Taspine (as we mention in the theoretical basis, figure 12) that is an alkaloid which is described as the active ingredient in dragon's blood [29].
Which has been seen in rats and humans when applied in a cream formulation [31]. Dragon's blood stimulated the contraction of the wound, the formation of new collagen and the regeneration of the epithelial layer [32]. For the expertise collected so far, it is recommended to apply the product on the decayed dentin, inside the cavity, for 60 seconds. After that period, the gel does not change color or texture, which is evident, is the agglutination of the decayed tissue. The main characteristic of the complete elimination of the infected dentinal tissue is the vitreous appearance of the cavity that appears after applying the gel. After this phase, the cavity should be washed and dried and the restorative technique monitored. If the decayed tissue has not been completely removed, the product must be reapplied until the cavity presents this vitreous appearance. After this phase, the cavity should be washed and dried and the restorative technique monitored.
This new dental product has many positive characteristics in addition to those mentioned above such as practicality and ease of use. On the other hand, it must be taken into account that the surface of the tooth is in a dynamic equilibrium with the surrounding environment. As the pH falls below a critical value, demineralization of the enamel, dentin or cement occurs, while a mineral gain (re-mineralization) occurs as the pH increases [33].
CONCLUSIONS
We developed an innovative chemical formulation for the Atraumatic Restorative Treatment (ART) of the carious lesions, which is an excellent option for the minimally invasive removal of caries tissue. Achieving a significant reduction of the residual cariogenic bacteria of Streptococcus mutans, among others, in dentin and occurs in the entire population exposed to this dental condition. This is due to the debriding action of papain that has a bactericidal and anti-inflammatory bacteriostatic activity, which is achieved with Dragon's blood in the formulation developed for removing the carious tissue that is achieved without promoting any type of stimulation or pressure in the affected area.
Note: For the structuring of this manuscript, the article called: How to write a patient case report by Cohen [34] was taken into account.

