











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Underground mining involves work activities that may have an impact on miners' health and in which they are exposed to several risk factors such as being in direct contact with particulate material. This exposure means a higher probability of developing occupational lung diseases, including pneumoconiosis, lung and pleura cancer, anthracosis, silicosis and occupational asthma. 1,2
Coal worker's pneumoconiosis is a chronic and irreversible lung disease that is caused by the inhalation of coal dust and its accumulation in the lungs. 1 In order to reach a diagnosis a documented history of exposure and a chest X-ray are required, besides the X-ray must meet the criteria established by the International Labor Organization (ILO) International classification of radiographs of pneumoconioses technical guidelines ILO/2011, which are based on the presence of parenchymal and pleural abnormalities. 3,4
Spirometry is used to monitor workers with pneumoconiosis as it allows the quantitative assessment of the mechanical aspects of breathing. 5,6 In the present study the forced expiratory volume in 1 second (FEV1) is the most appropriate indicator, since it can reflect reduced lung capacity and bronchial obstruction when associated with forced vital capacity scores (FEV1/FVC ratio); furthermore, based on its analysis it is possible to determine the type of respiratory disorder: obstructive, restrictive or mixed. 1
In the case of workers who have been exposed to coal dust it is of great importance to ask them whether they have a history of smoking or not, since this condition increases the risk of experiencing airway obstruction, which in turn means a reduced FEV1/FVC ratio. In this sense, Guerrero-Medina & Gutiérrez Strauss 2 state that the FEV1 result and the FEV1/FVC ratio allow a better characterization of lung function in smoking patients and in those with bronchitis.
In 1995, Rendón et al.7 reported a 5.12% (95%CI: 2.6-7.64) prevalence of pneumoconiosis in the municipality of Amagá, Antioquia (Colombia), while in 2000, Orduz-García 8, in a study conducted in coal workers of the same department, reported 189 cases of pneumoconiosis. Furthermore, in a study carried out in 2013 in underground miners of Boyacá exposed to coal dust, spirometry findings associated with obstructive and mixed patterns were observed in miners who had been working more than 20 years in these conditions. 9 Other studies allow concluding that, although pulmonary function tests are not decisive to reach a final diagnosis of pneumoconiosis, they are useful as an early diagnosis tool and as a medical surveillance measure in mining workers exposed to coal dust, besides they are cheap and easy to perform. 6,10
Occupational exposure in underground mines implies unfavorable factors due to workers being exposed to high levels of coal and silica dust; in addition hygiene and industrial safety measures in this work environment, as well as the workers' self-care practices, are not always adequate. 11
However, pneumoconiosis can be prevented as long as the amount of dust in the work environment is substantially reduced, and therefore the amount that is inhaled and accumulated in the lungs. 12 Current knowledge on the pathogenesis of the disease and technological advances that allow the implementation of control measures can reduce its progression, especially in the case of acute or rapid progression types, which have been associated with an increased exposure to dust. 13-15
The objectives of the present study were to determine the prevalence of pneumoconiosis in underground mining workers exposed to coal dust in Cundinamarca, Colombia, and to characterize their spirometry tests results and the presence of respiratory disorders symptoms.
Materials and methods
Study design
A cross-sectional study was conducted. The study population consisted of underground mining workers from Cundinamarca, Colombia. Estimators and statistical tests were constructed using a probabilistic, stratified and multistage cluster sampling design.
Sample
A probabilistic, multistage and cluster sampling design was carried out in two stages: in the first stage, the primary sampling units consisted of the underground mining companies in Cundinamarca, while in the second, the secondary sampling units were made up by the workers of the companies that were randomly selected. The selection of companies and workers was made using the simple random sampling technique.
The following values were obtained: accuracy: 5%; reliability: 95%: prevalence: 40%, and cluster sampling design effect: 1.5. The sample size was 215 workers from a sample universe of 1 901 individuals with occupational exposure to coal dust and who, at the time of conducting the study, were working in 11 companies; selection was carried out by establishing homogeneous groups of similar exposure to coal dust (SEGs). In the event a selected worker refused participating or was not able to take part in the study due to not being present in the mine, said individual was randomly replaced by another subject taking into account the SEGs.
Subjects who were administered the structured questionnaires, as well as the paraclinical tests, were selected from a list in which all workers were included.
Inclusion criteria
Having worked in the mining industry for 10 or more years
Being an active worker in the selected companies at the time field work was conducted
Voluntary acceptance to participate in the study
Workers who were younger than 18 years old, those with a condition in which the performance of forced spirometry was contraindicated (recent pneumothorax, active respiratory infections, recent myocardial infarction, unstable angina, thoracic aortic aneurysm, among others), those diagnosed with any respiratory disease or under treatment and pregnant women, were excluded.
Data collection instruments
Two surveys were used to collect data, the first was administered to the selected workers in order to obtain information on their social and demographic (age, sex, place of residence, educational level, socioeconomic level, marital status), occupational (years of service in the mining industry, posts held, type of job, and exposure time at the time field work was conducted), and toxicological characteristics (whether the worker was a smoker or not), as well as information on their respiratory symptoms. The second survey focused on the occupational medical history of the workers, in which the occupational health assessment made by physicians specialized in occupational health with a valid license was recorded.
Paraclinical tests included a chest X-ray, which was performed and interpreted according to the criteria established by the ILO, and a forced spirometry test performed by a respiratory therapist.
Chest X-rays were interpreted by two people certified by the National Institute for Occupational Safety and Health (NIOSH); in addition, compliance with the requirements established by the ILO was ensured.
Spirometry is considered a practical tool to monitor workers, for it allows the quantitative assessment of the mechanical characteristics of breathing. In order to perform this test, the patient, after performing a maximal inspiration, is asked to exhale all the inhaled air as fast as possible. In the present study, the assessment was made based on the official ATS/ERS technical standards, where values are considered normal when FVC is >80% of the expected value in relation to height, weight, age and sex; FEV1 is >80% of the expected value, and FEV1/FVC ratio is >70%. 16.
Operationalization of the variables
The respiratory signs and symptoms (respiratory system alterations reported by workers) and the results of the spirometry tests (spirometric alterations and values according to the ATS/ERS standards) were defined as independent variables, while pneumoconiosis (workers whose chest X-rays results were compatible with pneumoconiosis diagnosis) was defined as the dependent variable. In addition, the other occupational and sociodemographic variables were considered as confounders: years of service in the underground mining industry, type of job according to the SEGs classification (mining activities performed at the face of the mine, faceworkers and pick miners; transport related activities, those responsible for carrying the coal from the pithead to the unloading area; maintenance work, those hired as timbermen and who are responsible for cutting and installing timbers to support the roof and walls of haulageways, passageways, and the shaft of the mine; services, those in charge of transporting materials and supplies, and loading point, those responsible for selecting coal by size and removing other rocks and foreign bodies), length of time in the current position (number of months the worker has held the position), company size (small: from 1 to 50 workers; medium: from 51 to 99 workers, and large: more than 100 workers), age of the worker (in years) and history of smoking (total time in months).
Pilot test and data quality control strategies
In order to standardize all procedures, a pilot test was conducted on a sample equivalent to 10% of the final sample used in this study (n=215). It is worth noting that the companies whose workers participated in the pilot study were not included in the final sample.
Data collection was achieved through the individual administration of structured questionnaires to each participant by members of the research team who were previously trained to ensure a standardized application of the surveys. Both, the questionnaires and the clinical tests were conducted on the same day for each worker.
At the end of each day, the information obtained from the administration of the questionnaires was reviewed by another member of the research team in order to ensure its quality and identify any inconsistencies or missing data that could affect its analysis. When inconsistencies were found, the information was checked again with the company or the worker. Likewise, all data were checked before their inclusion in the project database and its subsequent analysis.
Data was systematized by creating the database structure in the Variable View module and then it was entered into the database View. Data input was checked using automatic control programs provided by the SPSS Statistics software version 25.0.
Statistical analysis
Regarding the description of variables, absolute and relative frequency distributions, expressed in percentages, were used for qualitative variables, while measures of central tendency and variability were used for quantitative variables. Estimators and statistical tests were constructed using the probabilistic, stratified and multistage cluster sampling design available in the Complex Samples module of the IBM® SPSS package, version 25.0.
The prevalences of pneumoconiosis, spirometric obstructive patterns and respiratory signs and symptoms were estimated with their respective 95% confidence intervals (CI). The precision of the estimators of these parameters was measured with the standard error of the estimate (SE) and the relative standard error (RSE), using the quality criteria of the estimators established by the Canadian Statistical Office for the RSE (A quality: 0-15%; B: 15.1-30%; C: 30.1-50%, and D:> 50%).
Associations between qualitative and independent variables (symptoms and spirometry) with pneumoconiosis were evaluated using the Pearson's chi-square test (aka chi-square test of association), the prevalence ratio (PR) and their respective 95% confidence interval. On the other hand, the t-Student test was used to evaluate spirometry numerical variables for pneumoconiosis, and the multivariate analysis of pneumoconiosis was constructed from a Cox regression model with constant risk time and robust variance estimators for multistage stratified cluster sampling. The level of significance used in the statistical tests was 5% (p<0.05).
Ethical considerations
This research is part of a larger project (Evaluation of the exposure to coal dust in underground mining in three departments of Colombia) carried out jointly by Universidad del Rosario, Universidad de los Andes, Positiva Compañía de Seguros ARL (Workers' compensation insurance company), Instituto Nacional de Salud (National Institute of Health) and the Governor's Office of the Department of Boyacá, and co-financed by Colciencias (Administrative Department of Science, Technology and Innovation) through contract No. 379-2011.
Also, this article derives from a master's thesis available in the digital archive of Universidad del Rosario 17. The scientific, technical and administrative standards on health research established by Resolution 8430 of1993, issued by the Colombian Ministry of Health, were followed in the development of the research project, which was classified as a minimum risk study according to this resolution. 18 Similarly, the ethical principles for medical research involving human subjects outlined in the Declaration of Helsinki were followed. 19
The execution of the study was approved by the Ethics Committee of Instituto Nacional de Salud (Minutes No. REG-R03.002.0000-006 of October 18, 2011) and prior to collecting the information and performing the spirometry tests and chest X-rays, workers were fully informed on the objectives of the study and were asked to sign an informed consent form in which they agreed to participate.
Results
Demographic and occupational characteristics
The study population consisted of 215 workers, of which only 1 was a woman. The average age was 45.5 ± 9.4 years, with minimum and maximum ages of 24 and 76 years, respectively. The average length of service was 21.7 ± 10.0 years, with minimum and maximum lengths of employment of 10 and 57 years, respectively. Pick miner was the most frequent post, followed by timberman; less than 10% of the sample held other posts. In relation to smoking, 4 out of 10 workers reported a history of smoking (Table 1).

Respiratory signs and symptoms
Expectoration was the respiratory sign or symptom most frequently reported (73.5%, 95%CI: 64.3-81.0), followed by coughing in the morning after waking up (63.3%, 95%CI: 52.9-72.5), waking up in the middle of the night due to a coughing fit at least once in the last 12 months (63.7%, 95%CI: 52.8-73.4), and chest tightness (46.0%, 95%CI: 38.6-53.6).
Assessment of spirometry tests
Regarding spirometry tests results, a normal pattern was observed in 89.8% subjects, while obstructive, restrictive and mixed patterns were observed in 5.1%, 0.5% and 0.9%, respectively. In addition, a peripheral airways dysfunction pattern was observed in 10.2% participants (95%CI: 6.3-16.3). Prevalence of pneumoconiosis
The prevalence of chest X-ray interpretations compatible with pneumoconiosis diagnosis according to the ILO criteria was 42.3% (95%CI: 33.9-51.2).
Factors associated with pneumoconiosis
FEV1/FVC ratio (p=0.045) and FF25-75% (forced expiratory flow at 25-75%) (p<0.001) spirometry values were significantly lower in workers compatible with pneumoconiosis diagnosis (Table 2). There were no significant differences regarding FVC (p=0.658).
Table 2 Estimates of spirometry values for pneumoconiosis diagnosis.
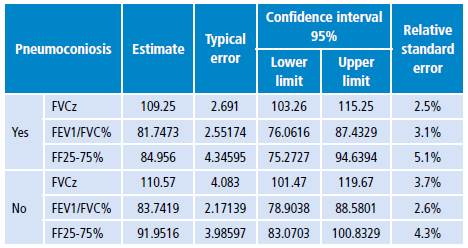
FVCz: Z-score of Functional Vital Capacity; FEV1/FVC%: Tiffeneau-Pinelli index, FF25-75%: Forced expiratory flow at 25-75%.
Source: Own elaboration.
However, there were not statistically significant differences between the presence or absence of any spirometric alteration and reported symptomatology (p>0.05). Likewise, based on the chest X-ray interpretation, there were not differences between the respiratory symptoms reported by workers with pneumoconiosis and those without this condition (p> 0.05).
Multivariate analysis
In the case of independent variables, in relation to pneumoconiosis, FEF25-75% was the only significant spirometric variable, while occupational exposure length was the only significant occupational variable (Table 3).

Discussion
Long-term exposure to coal dust in underground mining workers is significantly associated with negative effects on their health that mainly lead to the development of chronic respiratory disorders.
In the present study, the prevalence of chest X-ray readings compatible with pneumoconiosis diagnosis (according to the ILO criteria) was 42.33%, which is higher than what similar studies have reported. 7,8,20,21 This might be caused by the minimum time of exposure (≥10 years) established as an inclusion criterion here, and the fact that pneumoconiosis is a chronic disease. Also, 50.2% of the subjects worked as pick miners, i.e., those in charge of working at the face of the mine using picks, hammers and hand saws to remove rocks and extract coal, which is considered a high exposure post.
Likewise, the prevalence of respiratory symptoms and spirometric obstructive patterns reported here suggests that this population might develop other lung diseases such as chronic bronchitis and chronic obstructive pulmonary disease. On the other hand, in terms of respiratory symptoms, expectoration and coughing were more frequent than what Caballero et al.22 reported in a study conducted on general population over 40 years old from five cities of Colombia.
Contrary to what is described by Balmes et al.23, an association between smoking and pneumoconiosis was not found.
Regarding spirometry results, the FEV1/FVC ratio and FF25-75% values were significantly lower in workers with pneumoconiosis, which coincides with the findings by Wang et al.20
Spirometry is a poorly sensitive test, since in some cases respiratory diseases won't be detected with it. In addition, the variability of spirometric measurements is attributed to factors such as size, age and sex, among others. 24 However, it is a useful test in the context of pre-employment testing and periodic occupational testing in workers exposed to coal dust.
Radiological findings alone are not enough to reach a pneumoconiosis diagnosis, but they allow determining cases that are compatible with this condition. For a proper diagnosis, the history of exposure must also be considered, including the years of service in underground mining activities and clinical signs. 3 Therefore, performing a more detailed analysis of the exposure to coal dust combined with and early identification of symptoms and the occupational history of the patient is suggested.
Data collection and paraclinical tests were performed on the same day for each worker, yet the quality of the information and the tests results were not affected by this situation, since chest radiographs were read two days after they were performed and the physicians who assessed them did not know the diagnosis that was made based on the readings made at the moment the test was carried out.
On the other hand, in order to minimize memory biases during the provision of information by the workers, they were not asked open questions regarding information available in their personal medical history; however, as pneumoconiosis is a chronic development disease, only those workers with at least 10 years of exposure were included, which might represent a possible selection bias.
Conclusions
The prevalence of pneumoconiosis in underground mining workers from Cundinamarca was very high and its occurrence was associated with the FEV1/FCV ratio and FF25-75% values of the spirometry test, since they were significantly lower in workers with pneumoconiosis. Given that there are no effective medical treatments for pneumoconiosis, it is necessary to establish control measures or prevention activities aimed at minimizing exposure to coal dust.
In order to reduce occupational exposure to crystalline silica and coal dust and prevent pneumoconiosis, silicosis and deaths related to these diseases, the following actions are suggested: performing surveillance activities based on the Evidence-Based Comprehensive Care Guidelines for Lung Cancer and Pneumoconiosis of the Colombian Ministry of Health 3, implementing new technologies to reduce exposure, reviewing the effectiveness of the existing control methods in mining companies, and carrying out a comprehensive intervention in these companies based on periodic occupational hygiene monitoring aimed at verifying the effectiveness of the implemented measures.


