











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink"Come, there is no use in crying like that!" said Alice to herself
rather sharply. "I advise you to leave off this minute!"
She generally gave herself very good advice (though she very
seldom followed it), and sometimes scolded herself so severely
as to bring tears into her eyes".
Lewis Carroll, Alice's Adventures in Wonderland
It has long been appreciated that healthy human beings constantly attempt to maximize their positive and minimize their negative feelings. This ancient human ability to modulate how we feel has been referred to as 'intrinsic' emotion regulation (ER) (Gross & Thompson, 2007). The last decade has witnessed an explosive increase of studies exploring how intrinsic ER is related to mental health and well-being (for reviews see Gross, 2013; Nyklícek, Vingerhoets, & Zeelenberg, 2011; Werner & Gross, 2010). Two ER strategies have been the main focus of attention: re-appraisal and suppression. Reappraisal is a cognitively oriented form of ER, in which a person tries to think about a situation in ways that alter the emotional response (Gross, 2014), commonly re-framing its meaning in more positive (or less negative) terms (Gross & Thompson, 2007; McRae, Ochsner, & Gross, 2011). On the other hand, suppression is a behaviorally oriented form of ER in which a person decreases emotion-expressive behavior while emotionally aroused (Gross, 2014). In other words, suppression does not involve changes in meaning but refers to the capacity to voluntarily manipulate the expression of emotions (Gross & Thompson, 2007).
Reappraisal and suppression are both voluntary forms of ER, appearing to rely -at different levels- on the use of verbal thinking. This is quite clear in the case of reappraisal, a cognitively oriented form of ER, where individuals need to generate alternative narratives to buffer the emotional impact of negative events (McRae, Jacobs, Ray, John, & Gross, 2011). In response modulation, which is a behaviorally oriented ER, the role of verbal thinking is less clear. However, it is common to find that individuals often talk to themselves as a way of reinforcing the inhibition of emotion-expressive behavior. This idea is supported by data from neuropsychological studies suggesting that both forms of ER rely on verbal thinking. Indeed, together with inhibition, verbal fluency (or the capacity to generate language-based mental representations) has been reported as a key component in both reappraisal and suppression (Gyurak, Good-kind, Madan, Kramer, Miller, & Levenson, 2009; McRae et al., 2011; Salas, Gross, & Turnbull, 2014). In sum, it seems that several forms of voluntary ER require the use of verbal thought addressed to the self. This form of verbal thinking has commonly been described as 'self-talk', or inner speech (IS), and has recently been proposed as a potential component of ER (Salas, Gross, Rafal, Viñas-Guasch, & Turnbull, 2013, Salas, Radovic, Yuen, Yeates, Castro, & Turnbull, 2014b). Unfortunately, the existing ER models have not yet explored the role that inner speech may have in implementing ER strategies.
It is interesting to note that, outside the field of ER, there is large body of research documenting the development of verbal thought and its role in self-regulation (for a review of this early research see Luria & Yudovic, 1971; Sokolov, 1972). Vygotsky, for example, noted that when children are between 3-7 they move from egocentric speech to inner speech. Egocentric speech is typically defined as overt audible speech that is not addressed to another person but to oneself (Winsler, 2009), and is used as a 'mental orientation', particularly when facing difficult situations that demand consciousness and reflection (Vygotsky, 1934/2012). As children grow up, egocentric speech fades away, the frequency of vocalizations decrease, and speech becomes internalized. With this inner speech, children start thinking in words instead of pronouncing them (Vygotsky, 1934/2012) and begin talking to themselves inside their heads (Winsler, 2009). According to Sokolov (1972), in adulthood, elements of inner speech can be found in conscious perceptions, in actions and also in emotional experiences, where they manifest themselves as verbal sets, instructions to oneself, or as verbal interpretations of sensations and perceptions.
In recent years, researchers have shown an increased interest in exploring the role of inner speech in the regulation of cognition and behavior. For example, several articles have provided evidence to support a link between inner speech and cognitive flexibility (e.g. Miyake, Emerson, Padilla, & Ahn, 2004), cognitive performance and self-monitoring (e.g. Perrone-Bertolotti, Rapin, Lachaux, Baciu, & Loeven-bruck, 2014), planning (e.g. Lidstone, Meins, & Fernyhough, 2010), reflexive awareness (e.g. Morin, 2005) and self-regulation (e.g. Clowes, 2007; Emerson & Miyake, 2003; Tullett & Inzlicht, 2010). Even though existing research appears to offer strong evidence to support inner speech's central role in the regulation of cognition and behaviour, no studies have yet explored its relevance in the regulation of emotion.
A related topic of relevance is found in the growing number of studies linking inner speech to psychopathology (for a review see Alderson-Day & Fernyhough, 2015). Most of the research on this area has focused on the relationship between inner speech and psychotic phenomena, such as hallucinations (Perona-Garcelan et al., 2017) or dissociation and ideas of reference (Bellido-Zanin et al., 2017). For example, some studies have shown a positive relationship between 'dialogic' forms of inner speech and auditory hallucination-proneness (e.g. McCarthy-Jones & Fernyhough, 2011). Depression has also been linked to inner speech, particularly in the context of ruminative thought process, which typically has a verbal quality (Nolen-Hoeskema, 2000, 2004). However, this link has been rather conceptual, with very few studies directly exploring the relationship between inner speech and perseverative negative thinking (Holmes, Lang, & Shah, 2009; Holmes, Mathews, Dalgleish, & Mackintosh, 2006), with some studies even contesting this claim. For example, in a study by Siegrist (1995), the frequency of inner speech usage, assessed via a self-report questionnaire, was not associated with measures of depression. Anxiety has been another psychopathological symptom associated with inner speech. It has been noted, for example, that worrying is a form of negative repetitive thinking, often verbal, that is uncontrollable and aimed at a problem that has no clear solution (Watkins, 2008). One study (McCarthy-Jones, & and Fernyhough, 2011) has reported that anxiety is positively related to evaluative/motivational forms of inner speech, and the presence of other voices in inner speech.
Taken together, the available evidence appears to suggest that inner speech has a role in the regulation of cognition and behavior, and may be a mechanism involved in some clinical populations that present a dysregulation of emotional processes. However, to date, the relationship between IS and emotion dysregulation, or between IS and the use of ER strategies, has not yet been directly explored. In view of the above-mentioned studies that link inner speech to cognitive and behavior regulation, the first question addressed by the present investigation was whether individuals with a higher usage of IS present fewer difficulties regulating emotion (ER Difficulty Hypothesis). In addition, and because there is evidence suggesting that inner speech usage may be related to psychopathology, a secondary question was whether the level of symptomatology (anxiety and depression) had a mediating role between inner speech usage and the level of emotion dysregulation. We predicted that the negative relationship between inner speech and emotion dysregulation decreases in individuals who have high levels of symptomatology. Furthermore, the present study explored whether inner speech usage was associated with particular ER strategies. More specifically, and due to the fact that reappraisal is a cognitively oriented form of ER and suppression a behaviourally oriented form, it might be expected that inner speech would be positively associated with reappraisal but negatively associated with suppression (ER Strategies Hypothesis).
Method
Participants
180 psychology students participated in this study (Sex: female = 135, 75%; male = 45, 25%; Age: M = 19.85; SD = 2.77, range 18 - 36). Participants were recruited from Bangor University and received credits as payment for their participation.
Instruments
This is a correlational study since the association of inner speech and ER was the main focus of investigation. One self-report inner speech questionnaire and two ER related questionnaires were used. In addition, a questionnaire that assesses emotional symptomatology was also employed.
The Inner Speech Scale or ISS (Siegrist, 1995) is an 18-item questionnaire designed to measure the frequency of inner speech usage. Participants are asked to report on their level of agreement with each statement (e.g. If I am not feeling well I often talk to myself about my state; In difficult situations, I sometimes say to myself: 'you can do this, you will do all right') using a 6-point Likert scale (1= strongly disagree; 6 = strongly agree). Uttl, Morin, and Hamper (2011) used the ISS with a sample of 380 students and reported high reliability with a Cronbach's alpha of .85. The Emotion Regulation Questionnaire or ERQ (Gross & John, 2003) is a 10-item questionnaire designed to capture the frequency use of ER strategies. It has two sub-scales: Reappraisal (e.g. When I want to feel more positive emotion (such as joy or amusement), I change what I'm thinking about) and Suppression (e.g. I keep my emotions to myself). Individuals rate each of these items using a 7-point Likert scale (1 = strongly disagree, 7 = strongly agree). The ERQ has shown high reliability and has a Cronbach's alpha of .79 for the Reappraisal scale and .73 for the Suppression scale. The Difficulties in Emotion Regulation Scale or DERS (Gratz & Roemer, 2004) is a 36-item questionnaire designed to capture emotion dysregulation. It has six subscales: Non Acceptance of Emotional Responses (e.g. When I'm upset, I feel guilty for feeling that way), Difficulties Engaging in Goal Directed Behaviour (e.g. When I'm upset, I have difficulty focusing on other things), Impulse Control Difficulties (e.g. When I'm upset, I feel out of control), Lack of Emotional Awareness (e.g. When I'm upset, I take time to figure out what I'm really feeling), Limited Access to Emotion Regulation Strategies (e.g. When I'm upset, I believe that wallowing in it is all I can do) and Lack of Emotional Clarity (e.g. I have difficulties making sense out of my feelings). Individuals rate each item using a 5-point Likert scale to indicate how often the statements apply to them (1 = almost never (0-10%), 5 = almost always (91-100%)). All the subscales in the DERS have shown high reliability with Cronbach's alphas ranging from .80 to .89. The Hospital Anxiety and Depression Scale (H4DS, Olsson, Mykletun, & Dahl, 2005) is a self-rating questionnaire that assesses the presence of emotional symptoms. The scale consists of 14 items that measure different manifestations of anxiety and depression. For each item, participants are expected to select an answer from four possible choices that reflect the frequency of such symptoms experienced during a week.
Procedures
Bangor School of Psychology's Ethical Board reviewed and approved this research project. Participants completed the assessment using an online survey platform provided by Bangor University that allowed no missing data. Information about the main goal of the study was provided in writing, and consent was obtained electronically. Once the questionnaires were complete, participants were debriefed on the investigation's main goals.
Analysis
In order to test Hypothesis 1 (ER Difficulty Hypothesis), different models of relationship between inner speech usage (ISS) and difficulties in ER (DERS) were explored. We initially built a hierarchical linear regression by successively incorporating new predictors. First we tested the independent relationship between the dependent variable Difficulties in Emotion Regulation (DERS total score) with Inner Speech usage (ISS total score). Then we added the level of symptomatology as a predictor to the model, using the HADS total score. In order to investigate this hypothesis further, a similar approach, using hierarchical linear regression models, was employed to explore the relationship between inner speech usage (ISS total score) and specific types of difficulty in regulating emotions (DERS subscales). In relationship to Hypothesis 2 [ER Strategies Hypothesis] a similar approach was followed. Two different linear regressions, with reappraisal and suppression frequency use as dependent variables, were carried out separately, both following the same structure. In the first step, the independent effect of inner speech was assessed including the total score of the ISS. In the second step, the model was controlled for the level of difficulties regulating emotions reported by subjects (DERS total score) and the interaction of this variable with Inner speech usage (DERS*ISS). The interaction term was computed on the variables centred by their mean (to avoid problems of multicollinearity). This step allowed exploring if the effect of inner speech remained the same when controlling for difficulties in ER and if this effect changed at different levels of ER difficulty. Finally, in the third and final step, the level of symptomatology as control was added (HADS total score). When addressing hypothesis 1 and 2, assumptions of multicollinearity, homoscedasticity and independence of errors were tested by exploring residual plots, Durbin-Watson test and the variance inflation factor. If any of these assumptions were not met, this was reported in the manuscript.
Results
Instrument reliability and concurrent validity
As can be observed in Table 1, the Inner Speech Scale presented adequate levels of internal consistency, with a Cronbach alpha of .91. Regarding the instruments that measured ER and symptomatology, adequate levels of internal consistency were also observed. In the case of the DERS, the total scale presented a Cronbach alpha of .94, while its subscales ranged between .80 and .90. As for the ERQ, both subscales also exhibited adequate levels of internal consistency (Reappraisal = .89; Suppression = .77). Finally, The Hospital Anxiety and Depression Scale presented a Cronbach alpha of .83.
Table 1 Descriptive Results and Reliability Information of Questionnaires.
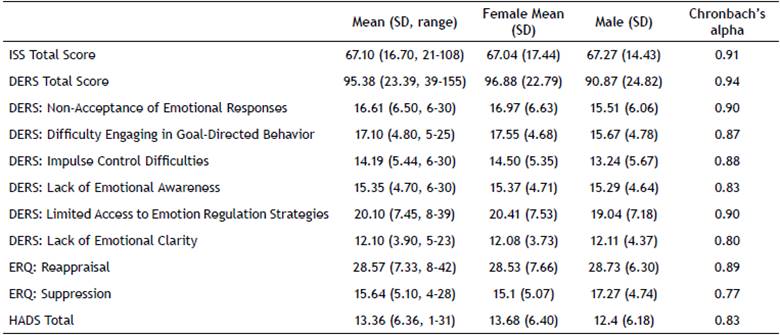
ISS: Inner Speech Scale; DERS: Difficulties in Emotion Regulation Scale; ERQ: Emotion Regulation Questionnaire; HADS: Hospital Depression and Anxiety Scale.
When exploring the concurrent validity of both ER instruments, a moderate correlation between scales was observed. This was higher between the DERS and the ERQ subscales (see Table 2). More specifically, the DERS total score presented a negative correlation of small size with the Reappraisal subscale (r = -.22, p= .002) but a positive correlation of medium size with the Suppression subscale (r = .31, p< .001). When looking at how specific subscales from the DERS related to the ERQ subscales, we observed that the Suppression scale exhibited medium positive correlations with a lack of Emotional Clarity (r = .43, p< .001), Non-acceptance of Emotional experience (r = .33, p< .001) and Lack of Emotional Awareness (r = .34, p< .001). Only a small positive correlation between Suppression and Limited Access to Emotion Regulation Strategies was found (r = .16, p= .04). In contrast, the subscale of Reappraisal only presented a medium negative correlation with Lack of Emotional Awareness (r = -.29, p< .001) and a small negative correlation with Limited Access to Emotion Regulation Strategies (r = -.23, p= .002) and lack of Emotional Clarity (r = -.15, p= .05). It is also interesting to note that both ER scales were associated with levels of emotional distress (HADS). The DERS total score presented a large positive association with the levels of symptomatology (r = .61, p< .01). In contrast, the associations of the ERQ with the HADS were of small size, negative for Reappraisal (r = -.26, p< .01) and positive for Suppression (r= .13, p< .05).
Table 2 Bivariate Correlations (Pearson).

** Correlation is significant at the 0.01 level (2-tailed). * Correlation is significant at the 0.05 level (2 tailed).
ISS_TOT = Inner Speech Scale Total; ERQ_REAP = Reappraisal subscale; ERQ_SUP = Suppression Subscale; DERS_TOTAL = Difficulties in Emotion Regulation Scale total score; DERS_NON = Non-Acceptance of Emotional Responses subscale; DERS_GOA = Difficulties Engaging in Goal Directed Behavior Scale; DERS_IMP = Impulse Control Difficulties Subscale; DERS_AWA = Lack of Emotional Awareness Subscale; DERS_STR = Limited Access to Emotion Regulation Strategies Subscale; DERS_CLA = Lack of Emotional Clarity Subscale; HADS_TOT = Hospital Anxiety and Depression Scale.
Emotion Regulation Difficulties
Investigating the relationship between inner speech and ER produced mixed results. The ER difficulty hypothesis suggested that inner speech usage would be negatively associated with ER difficulties. In other words, this hypothesis expected that individuals who frequently used inner speech would have fewer difficulties regulating negative emotions. However, this hypothesis was not supported in the present study. On the contrary, a positive relationship was found (ß = .22, p < .001), with the model accounting for 5% of the variance (F (1, 178) = 9.43, p = .002). On further exploration, it was also found that the level of symptomatology (HADS total score) fully mediated this relationship. More specifically, when adding to the linear regression a second block that included level of reported depression and anxiety symptoms, the relationship between inner speech usage and ER difficulties dropped and became non-significant (ß = .098, p = .108). This model explained 37% of the variance, a significantly higher proportion than the previous model (ΔR2= .33, F (1, 176) = 46.94, p < .001). For further details on this model see Table 3. In sum, the ER Hypothesis was not supported since individuals with a high IS usage also presented higher levels of ER difficulties. This relation, however, was completely mediated by the level of symptomatology, which indicated that, when controlled by emotional distress (anxiety/depression), the frequency of use of inner speech does not have an effect on difficulties to regulate emotions.
Table 3 Regression Models for Inner Speech and DERS total score.

a Dependent Variable: DERS_TOT
ISS_TOT = Inner Speech Scale Total; DERS_TOTAL = Difficulties in Emotion Regulation Scale total score; HADS_TOT = Hospital Anxiety and Depression Scale.
The Emotion Regulation Hypothesis was also explored by using models that tested whether IS usage presented significant associations with different types of difficulty in regulating emotions (DERS subscales). Here results were mixed (see Table 4). IS usage did not present significant associations with the Difficulties Engaging in Goal Directed Behavior (ß= 0.13, p= .09) or Lack of Emotional Clarity subscales (ß= .09, p= .22). In contrast, significant positive correlations were found between inner speech usage and Non-Acceptance of Emotional Responses (ß= .28, p< .001), Impulse Control Difficulties (ß= .27, p< .001) and Limited Access to ER Strategies (ß= .29, p< .001). It is interesting to note that, when controlling for level of symptomatology (HADS), the size of all three relationships decreased, but did not disappear. This suggested that there is a small independent positive relationship between inner speech usage and these types of ER difficulties. In other words, individuals that frequently experience difficulties accepting their emotional responses, refraining from impulsive behavior, or accessing to ER strategies when experiencing negative emotions, also tend to frequently use inner speech. Only one subscale of the DERS, Lack of Emotional Awareness, presented a negative relationship with inner speech usage (ß= -.26, p< .001). Interestingly, this association appears not to be mediated by symptomatology, for when the HADS was included in the model, the relationship even slightly increased (ß= -.29, p< .001). This result suggests that individuals who report high levels of inner speech usage also report fewer difficulties becoming aware of their feelings when experiencing negative emotions. Overall, these results appear to suggest that inner speech is not equally related to different types of difficulties experienced by people when attempting to regulate their negative emotions.

ISS_TOT = Inner Speech Scale Total; DERS_NON = Non-Acceptance of Emotional Responses subscale; DERS_GOA = Difficulties Engaging in Goal Directed Behavior Scale; DERS_IMP = Impulse Control Difficulties Subscale; DERS_AWA = Lack of Emotional Awareness Subscale; DERS_STR = Limited Access to Emotion Regulation Strategies Subscale; DERS_CLA = Lack of Emotional Clarity Subscale; HADS_TOT = Hospital Anxiety and Depression Scale.
Emotion Regulation Strategies
The ER Strategies Hypothesis suggested that inner speech usage would be negatively associated with suppression but positively associated with reappraisal. Results from this study partially supported this hypothesis (see Table 5). In the case of suppression, no significant associations were found with inner speech usage (ß= .07, p= .34). In fact, data suggested that suppression rather depended on the level of ER difficulties experienced by individuals (DERS controlled by ISS ß= .31, p< .001), and was not associated with self-reported level of symptomatology (HADS controlled by ISS and DERS ß= .00, p= .99). Reappraisal presented a positive and significant association with IS usage (ß= .26, p< .001). In other words, participants with higher levels of inner speech did use reappraisal more often. Interestingly, even though difficulties in ER (DERS controlled by ISS ß= -.30, p< .001) and levels of symptomatology (HADS controlled by ISS and DERS ß= -.23, p= .01) had a negative association with reappraisal use, these two variables did not moderate the medium-size relationship between inner speech usage and reappraisal use. This result suggests that IS usage and reappraisal are independently related. In conclusion, data from this analysis suggests that reappraisal and suppression are not equally related to inner speech.
Table 5 Regression Models for Inner Speech and Emotion Regulation Strategies.

*** Correlation is significant at the 0.001 level (2-tailed), ** Correlation is significant at the 0.01 level (2-tailed).
ISS_TOT = Inner Speech Scale Total; DERS_TOTAL = Difficulties in Emotion Regulation Scale total score; HADS_TOT = Hospital Anxiety and Depression Scale.
Discussion
During the last decade, research on ER has offered valuable insights into how human beings voluntarily modulate negative feelings (for a revision, see Gross, 2014). In this context, a handful of studies have attempted to understand, or 'unpack', the underlying cognitive processes required by different ER strategies. It is known, for example, that both reappraisal and suppression involve the use of inhibition and verbal fluency (Gyurak et al., 2009; McRae et al., 2011; Salas, Gross, & Turnbull, 2014). Even though this knowledge offers valuable information on the problem, it is still preliminary and more theoretical and experimental work on the matter is required. The main goal of this article has been to contribute to this particular strand of literature, by exploring the potential role of a specific cognitive process in ER: inner speech. As noted in the introduction, inner speech -or the capacity to talk to ourselves silently inside our heads- has been generally associated with cognitive and behavioral regulation. Its link to ER, however, has been largely neglected. An example of this omission is the fact that IS is only mentioned once in the recently edited Handbook of Emotion Regulation (Gross, 2014). This contrasts markedly with the level of attention that IS has received in other areas of research, where its role in self-regulation and psychopathology has been widely acknowledged (for reviews see Alderson-Day & Fernyhough, 2015; Winsler, 2009). This study is the first to offer preliminary evidence on the relationship between inner speech and emotion regulation.
A first clear finding is that the use of IS is not related to the self-reported level of difficulties regulating negative emotions, since individuals with high levels of IS usage also tended to exhibit high overall levels of ER difficulties. Furthermore, the level of symptomatology heavily mediated this relationship. This finding appears to be in line with the existing literature that links IS with certain psychopathological presentations. It has been suggested by several studies that, in individuals with high levels of anxiety or depression, IS may fuel negative cognitions and feelings by acting as an 'overly evaluative' internal voice (McCarthy-Jones & Fernyhough, 2011; Newby & Moulds, 2012; Stokes & Hirsch, 2010). This line of argument appears to be supported by evidence from this study, which suggests that individuals who exhibited high levels of IS usage also reported a high frequency of 'secondary' negative emotions when feeling upset (Non-Acceptance of Emotional Responses). In moments of emotional turmoil, these subjects reported feelings of shame, guilt or even anger towards themselves for being upset. Thus, it can be suggested that IS could reinforce a negative emotional loop by acting as an overly evaluative or harsh inner voice.
However, IS was not equally related to all types of 'difficulties' regulating emotions, offering valuable insights into the specific roles that IS might play in ER. For example, IS was frequently used by individuals who also reported having a high frequency of difficulties controlling their behavior when upset (Impulse Control Difficulties subscale) or those who presented problems envisaging potential solutions when upset (Limited Access to ER Strategies subscale). Here, a question that remains to be answered by future experiments, which cannot be addressed here due to the correlational nature of this study, is whether the use of inner speech in individuals with high levels of ER difficulties reflects 'regulatory' efforts. In other words, whether inner speech is recruited as metacognitive tool to refrain behavior from impulsive responses, or to find alternative solutions during emotionally negative situations. This interpretation of data would be in line with the existing literature in cognitive psychology, where IS has been largely linked to impulse control (Luria, 1966; Tullet & Inzlicht, 2010) and problem solving (Emerson & Miyake, 2003; Lidstone, Meins, & Fernyhough, 2010). Behavioral studies, where the use of inner speech to regulate emotions is allowed or obstructed (for a review see Guerrero, 2005), could offer valuable insights into this question.
It is also interesting that another type of ER difficulty that appeared related to IS usage was emotional awareness. However, in this case, individuals who used IS more frequently had fewer problems paying attention to, and acknowledging, their emotions (Lack of Emotional Awareness subscale). These data suggest that the act of talking to ourselves -inside our heads- may facilitate the process by which we become aware of inner states in moments of negative arousal, thus acquiring a more reflective stance towards present emotional experience. This idea is consistent with a current view of IS as having a role in metacognition, self-awareness and self-understanding (Morin, 2005, 2011).
Perhaps the main finding of the present study is that IS does not have the same role for different ER strategies. This confirms the idea that ER strategies rely on dissimilar psychological processes (Gross, 2014). More specifically, data from this investigation suggests that only reappraisal -and not suppression- is related to IS since individuals with high use of IS, despite their level of symptomatology, tended to employ reappraisal as an ER strategy more often. Such finding contributes to a small literature exploring the underlying 'mechanisms' of ER strategies, which has suggested inhibition, verbal fluency and working memory as key components of reappraisal (McRae et al., 2011; Salas, Gross, & Turnbull, 2014). Why, then, is IS associated with reappraisal and not with suppression? A possible explanation may well be that reappraisal, as a cognitively oriented strategy, relies more heavily on the manipulation of mental representations, which are predominantly verbal in nature (McRae et al., 2011). Suppression, in contrast, because it is a behaviorally oriented ER strategy (Gross, 2014), appears to rely more heavily on motor control (Beer & Lombardo, 2007) and response inhibition (Gross, 1999; Gross & John, 2003; Gross & Thompson, 2007; Kühn, Gallinat, & Brass, 2011).
A related research question that remains to be explored by future studies is the specific role that IS may have for reappraisal itself, and how it relates to other components. It has been suggested, for example, that in order to reappraise, several cognitive control sub-processes need to take place (e.g. working memory, inhibition, verbal fluency, McRae et al., 2011). It is surprising, however, that theorizations such as this tend to omit the fact that reappraisal, in general, involves the manipulation of verbal representations about reality, which are addressed to the self, as an object of ER. In other words, re-interpretations of negative events often occur in the context of a conscious internal dialogue where the self is at the same time the agent and object of a new narrative. Even though psychological components such as working memory, inhibition and verbal fluency offer some insight into the building blocks of reappraisal as an ER strategy, it is unlikely that they operate in isolation. On the contrary, a more ecological view of this complex process would suggest that they occur in the context of an internal narrative, which acts as a vehicle where cognitive control sub-processes take place, thus directing behavior (Luria, 1959; Luria & Yudovich, 1971). Future studies will need to address this point by exploring how behavioral measures of inner speech relate to cognitive reappraisal performance and its underlying cognitive control components.
Limitations of the Study
The present study had several limitations that need to be considered when interpreting its results. Firstly, data was collected from a student sample, thus, only reflecting a fragment of the population that is not necessarily representative of it in terms of age, educational level or presence of psychological problems. Furthermore, as noted in the description of the sample, women were overrepresented compared to men, a fact that did not allow the proper exploration of sex as a potential moderator variable. A second methodological limitation refers to the correlational nature of the study, and the fact that data was gathered from surveys. New investigations should consider experimental designs where variables, such as inner speech ability, are behaviorally manipulated and participants engage in true emotion regulation tasks. Such approach will allow to control potential bias inherent to the use of self-report questionnaires.
Conclusions
As noted before, this study is the first one exploring the relationship between inner speech and ER. Even though results are preliminary -requiring further testing using experimental designs and non-student populations- they contribute importantly to the field of ER and have the potential to inform clinical work in two main ways. Firstly, data from this study suggests that people's inner speech should be routinely explored during clinical assessments since the frequency of use of inner speech can be associated with both emotion dysregulation and the use of reappraisal. In other words, and contrary to existing data that positively links inner speech to cognitive and behavior regulation, the relationship between inner speech and ER is more complex. Consequently, during clinical interview, it appears necessary to determine whether inner speech is used adaptively with regulatory ends or employed pathologically as a self-critical voice that perpetuates negative emotion. Surprisingly, inner speech is rarely considered a psychological process to be assessed during clinical interviews despite it playing a key role in perpetuating symptomatology or acting as a vehicle for therapeutic change. The use of self-reports of inner speech and the careful exploration of this process during patients' assessment process could offer some important insights to guide treatment.
Secondly, and relating to this last point, inner speech should be considered both as a target of psychological interventions as well as a tool to facilitate therapeutic change. Several intervention models designed to treat psychopathological populations with ER disorders have stressed the need to tackle perseverative cognitive processes that perpetuate negative affect. As noted in the introduction, several authors have linked inner speech to depressive rumination. Interestingly, many intervention models have also considered the use of self-talk itself as a tool to modify cognitive perseverative processes. Emotion Regulation Therapy (Menin & Fresco, 2014), for example, describes re-framing/re-appraising or the capacity to change cognitions to alter their emotional significance as a key component of their regulatory skills programme: an ability that was positively related to inner speech in this study. Furthermore, as a part of this training, clients are encouraged to develop compassionate internal dialogues and self-validating statements, which aim to soften automatic self-critical thoughts. Other therapeutic models, such as Dialectical Behavioral Therapy (Neacsiu, Bohus, & Linehan, 2014) or Affect Regulation Training (Berking & Schwarz, 2014), also consider compassionate self-support (self-soothing or self- encouraging strategies) as key ingredients in achieving therapeutic change.

