text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The World Health Organization (WHO) defines arterial hypertension (AHT) as a disorder that produces persistent arterial pressures equal to or greater than 140/90 mmHg 1. AHT is a serious public health problem worldwide 1. The development of AHT is multicausal and may be influenced by genetic load; race and sex; metabolic diseases, such as diabetes and dyslipidemia; and behavioral factors, such as alcohol consumption, smoking and sedentary lifestyle 1.
According to the Institute for Health Metrics and Evaluation (IHME), AHT is the largest contributor to the disease and mortality burden 2. This condition is the main risk factor for cardiovascular disease, renal failure, premature mortality and disability 3,4. Of the 17 million deaths per year caused by cardiovascular disease, AHT explains up to 9.4 million of these deaths 5. Moreover, during 2008, the WHO estimated that AHT was responsible for at least 51% of deaths due to stroke 6. In 2014, the global prevalence of AHT in patients older than 18 years was 22.2% 7.
In Colombia, the National Health Survey conducted in 2007 showed a prevalence of AHT in the general population of 22.8% 8. During 2011, the prevalence was estimated at 7.29%, with an annual incidence of 191.31 per 100,000 inhabitants and an AHT mortality rate of 13.97 per 100,000 inhabitants 9,10. For 2013 in Colombia, according to data from the High-Cost Account, a total of 2,414,354 people with AHT were affiliated with the General System of Social Security in Health, yielding a prevalence of 5.53% 11. Chow et al. reported a prevalence of AHT of 37.5% in urban and rural Colombian populations aged 35-70 years in the Prospective Urban Rural Epidemiology (PURE) study 12.
The epidemiological importance of AHT, in terms of occurrence and mortality, increases with population growth and aging, particularly in women 9,10. For this reason, and given the increase in the global prevalence of AHT, the variability in estimates for Colombia and the need for reliable and quality information (the key instrument for the development of public policies), the question arises: What is the prevalence of AHT in the population over 18 years of age in Colombia, and what is its pattern according to sex and age?
Materials and Methods
Literature search strategy
A systematic literature search was conducted for studies that estimated the prevalence of AHT in an urban and/or rural Colombian population over 18 years of age. The search was conducted until February 2018 in the PubMed, Lilacs, Ovid, Google Scholar and SciELO databases. There was no restriction regarding the year the studies were conducted.
The search languages were English and Spanish. Studies were identified in all search engines with the following strategy: (Hypertension) AND (Colombia) or (Hipertensión Arterial) AND (Colombia) or (Cardiovascular Risk Factors) AND (Colombia). The authors excluded duplicate records and reviewed the titles and abstracts of all studies that were potentially relevant for this review. Last, after reviewing the full text, some studies were excluded because they did not provide prevalence estimates, the population was not representative or there was some other problem with the study's quality.
Eligibility criteria
Studies with the following types of design were included: a) cross-sectional, b) health survey and c) population-based cohort study. Regarding the sample population, studies that aimed to determine the prevalence of AHT in an adult Colombian population aged 18 or older were included. AHT was defined as SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, or the use of antihypertensive medications.
Data extraction
The following data were extracted from all included studies: first author, year of publication, date the study was conducted, sample size, city/municipality, area (urban/rural), age, mean age, proportion of men and women, number of blood pressure readings, position of blood pressure readings, resting time between blood pressure readings, instrument used for blood pressure measurements, mean systolic and diastolic blood pressure and prevalence of AHT by sex and age. The quality of data reporting was determined according to the STROBE statement, and the risk of bias in each study was evaluated.
Statistical analysis
For the systematic review, a meta-analysis was conducted using the random effects model to estimate the prevalence and 95% confidence intervals (CIs) using the DerSimonian and Laird method 13. The variance of the prevalences was stabilized using the Freeman-Tukey arcsine transformation 14. Estimates were made using the metaprop command 15; studies with proportions between 0-100% were not excluded. Heterogeneity was assessed using the I2 statistic. 12 reflects the variance explained by different conditions among studies and not only by measurement errors. The X2 test was used to quantify the heterogeneity among the studies with a level of significance of p < 0.10. Publication bias was visually evaluated using the funnel plot, and the effect of studies with a small sample size was estimated using the Egger test. The analysis was conducted in STATA version 11 and in Microsoft Office Excel 2010. The level of significance adopted was 5%.
Results
Selection process and characteristics of the studies
Of the 527 references identified by the search strategy, after duplicate articles were excluded and titles/abstracts were reviewed, 56 complete documents were obtained for review. Of these, one study did not estimate prevalence, seven did not have a representative sample, three did not perform objective blood pressure measurements, 12 defined AHT according to the metabolic syndrome criterion, and seven had a sample population that included children under 18 years of age.
A total of 23 studies met the proposed inclusion criteria (Figure 1); 10 of these were population cohort studies, and 13 were cross-sectional studies. These were characterized by the year of publication; the location of the study, including the geographic area (rural and/or urban); the data collection period; the number of participants, stratified by sex and age; the blood pressure measurement technique used; and the prevalence of hypertension in the population and the geographic area 8,16-37.

Studies on the prevalence of hypertension in the adult population in Colombia have been published in scientific journals since the 2000s and intensified in 2010-2013, with 14 studies published from 2010-2013. Of these, 18 were carried out in urban areas, one in a rural area and four in rural and urban areas (Table 1).
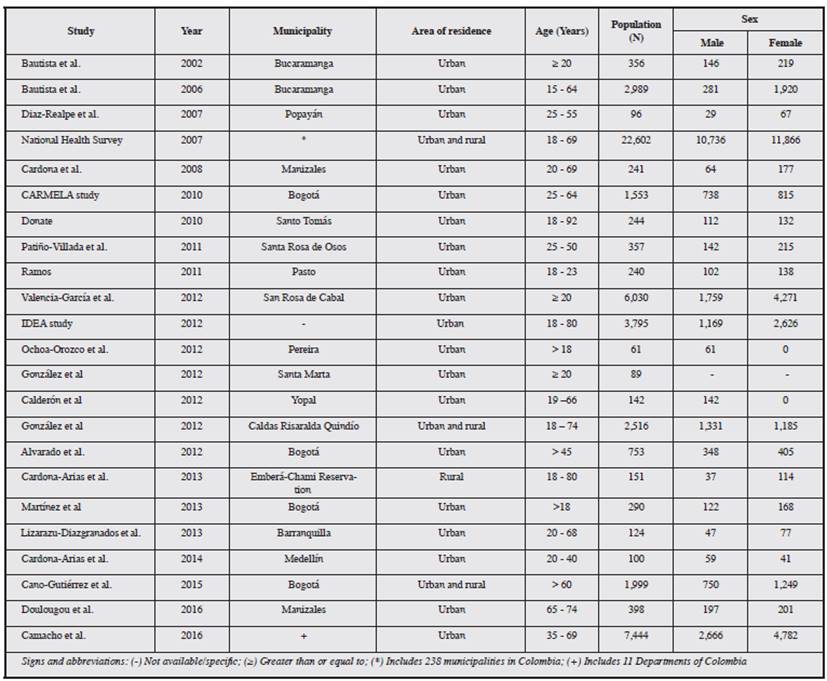
The largest sample included 22,602 people, and the smallest comprised 61 people. The female sex predominated in most studies, with females representing more than 60% of the study population. The Andean region, especially the coffee zone (Caldas, Quindío and Risaralda), was the most studied, and only one study on AHT in an indigenous population has been published (Table 1).
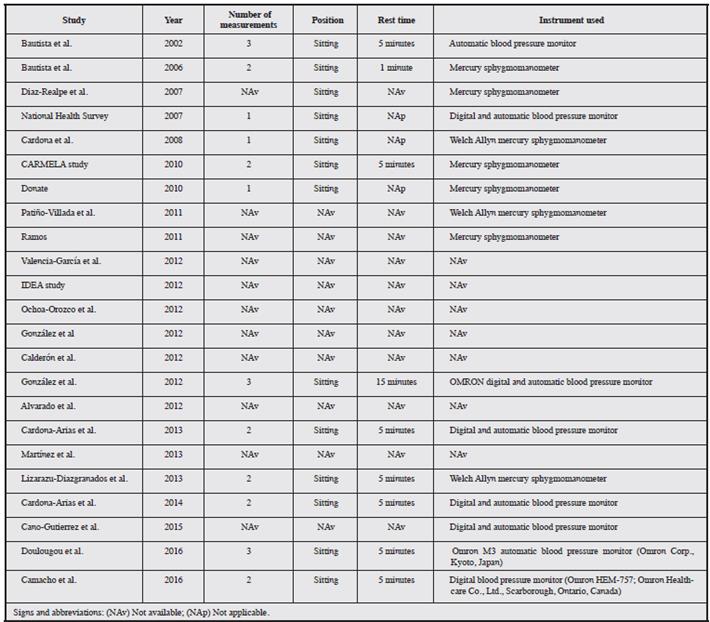
Regarding blood pressure measurements in the evaluated studies, 17 of the 23 studies described the measurement procedure used (Supplementary Table 1); the auscultation technique was the most frequently used technique, with automatic devices used to a lesser extent. Most of the studies stated that blood pressure was measured with the patient in the seated and indicated the use of a time interval between measurements. Processes prior to measurement were not mentioned, except in the case of studies that were based on the techniques suggested by the American Heart Association and the Pan American Health Organization-World Health Organization, which recommend avoiding caffeine consumption, resting for at least five minutes, emptying the bladder, among other precautions prior to blood pressure measurement.
Regarding the mean SBP and DBP, 8 of the 24 studies had this information. The mean SBP varied between 110.58125.5 mmHg, and the DBP between 66.6-78 mmHg. Both the SBP and DBP tended to be higher in men than in women. Cardona-Arias and Arroyave-Martínez 34 found a difference of almost 8 mmHg in SBP between men and women.
Prevalence of arterial hypertension
The prevalence of AHT in the 23 studies (52,570 individuals) was 24% (95% CI 19-29%; I2 = 99.36%, p < 0.001) with a range from 4.6 to 67.6% in the reviewed studies (Figure 2). A visual inspection of the funnel plot showed asymmetry, and the Egger test suggested publication bias related to the selected studies (p < 0.001). Heterogeneity among the studies was evident (X2 = 3421.92, df = 22, p < 0.001). The meta-regression evaluating the year of publication explained the heterogeneity observed in the prevalence of AHT (p = 0.007; R2 = 26.82%) (Supplementary Figure 1).

The prevalence of AHT increases according to age (Supplementary Table 2). Ramos 23 reported a prevalence of 4.6% in adults between 18 and 24 years of age. Camacho et al. 37 found a prevalence of 22.33% in individuals aged ≤ 50 years, but the prevalence increased to 51.62% among individuals aged ≥ 50 years.

Subgroup analysis
In the meta-analysis, eight studies with a sample size greater than 1,000 individuals were identified; these studies were considered extreme data. A meta-analysis was performed without these studies, and the prevalence was similar to the results when these studies were included (22%, 95% CI: 12-33%; I2 = 98.28%, p < 0.001).
In the analysis by type of study, population-based and cross-sectional studies comprised 28% (95% CI: 20-37%; I2 = 99.64%, p < 0.001) and 21% (95% CI: 43-29%; I2 = 98.57%, p < 0.001) of the sample, respectively (Table 2). In the studies whose sample included individuals aged > 45 years, > 60 years and 65-74 years, the prevalence reached 57.1, 56.9 and 67.5%, respectively, while the study that included only a young adult population (18-23 years of age) showed a prevalence lower than 5% (Supplementary Table 2).
Regarding sex, men had an AHT prevalence that ranged between 8.8 and 69%, with an overall prevalence of 29% (95% CI: 23-37%; I2 = 98.02%, p <0.001); in women, the prevalence ranged between 6 and 81.5%, with an overall AHT prevalence of 28% (95% CI: 21-36%; I2 = 99.17%, p < 0.001) (Figures 3 and 4). AHT was more common in studies conducted in both rural and urban areas, with a prevalence of 35% (95% CI: 23-49%; I2 = 99.78%, p < 0.001), compared to studies conducted in rural or urban areas only, which had prevalences of 34% (95% CI: 26-42%) and 21% (95% CI: 14-29%; I2 = 99.17%, p < 0.001), respectively (Table 2).


The meta-regressions by subgroups showed that not all covariables were possible explanations for the high heterogeneity among the studies (p > 0.05); the exception was the year of publication (p = 0.007; R2 = 26.9%). The percentage of women, sample size and geographic area of residence did not explain the heterogeneity among the studies; however, the year of publication and study design partially explained the observed heterogeneity (p = 0.002; R2 = 40.9%).
Discussion
This systematic review compiles the published evidence on the prevalence of arterial hypertension in Colombia. The small number of publications available and/or the use of adequate methodology; the failure to describe patterns of AHT according to age, sex and socioeconomic status; and the nondescription of the method used to measure blood pressure limit the analysis and comparison of the data.
The prevalence of AHT in Colombia estimated in this study was 24% (95% CI: 19-29%; I2 = 99.36%, p < 0.001); however, the prevalence was higher only when based on the data reported in population-based studies (28%; 95% CI: 20-37%), in which the population is more representative than in the descriptive studies with no sampling that were included in this review. These findings are similar to the global prevalence reported in the systematic review of Mills et al. (38), who estimated that in adults ≥ 20 years of age, the prevalence was 31.1% in 2010 (95% CI: 30.0-32.2%), 31.9% (30.3-33.5%) in men and 30.1% (28.5-31.6%) in women; despite the lack of a significant difference between the sexes, AHT tends to more commonly affect the male population, as was also estimated in this review.
In Latin America and the Caribbean, there is a disparity in the prevalence of AHT according to sex compared with the estimations found in the present study. Mills et al. estimated that the female population is the most affected, with a prevalence of 32.7%, while the prevalence in men is 30.4%. Those findings disagree with the prevalences found in Colombia, where despite a minimal difference, this chronic disease is more common in men: 29% (95% CI: 23-37%; I2 = 98.02%, p < 0.001) in the male population and 28% (95% CI 21-36%; I2 = 99.17%, p < 0.001) in the female population.
The high heterogeneity in our study is partly explained by the age of the population, the year of publication and the design of the studies evaluated. The study by Doulougou et al.36, which reported the highest prevalence (67.5%), included only adults aged 65-74 years; thus, it had a higher probability of detecting a population with AHT. Several mechanisms explain the occurrence of AHT in older adults; in summary, it is derived from changes in the arterial wall and in the neurohormonal regulation system, which together cause an increase peripheral vascular resistance 39.
On the one hand, there is loss of elasticity and distensibility in large and medium vessels, which together increase the stiffness of the vessel walls; on the other hand, there is a fundamental change in the endothelium-dependent vascular responses that is caused by the deterioration of the nitric oxide (NO) and alteration in the secretion of vascular relaxing factors and platelet antiaggregants, which favor vasoconstriction and the consequent increase in peripheral vascular resistance 39-41.
The prevalence of AHT in Colombia has increased in recent years. Studies conducted in 2012, such as the IDEA study 25, showed a prevalence of 22%, which is very different from that found by Bautista et al. 15, who estimated a prevalence of 9.51% in 2006. This sharp difference could be related to the adoption of lifestyles in the population that are recognized as favoring the development of cardiovascular morbidity: greater dietary intake of salt and fat, physical inactivity, obesity and increased recreational use of alcohol and tobacco 42-5.
The immediate harmful effects of smoking on AHT are related to the hyperactivity of the sympathetic nervous system, caused by the activation of excitatory nicotinic receptors present in peripheral chemoreceptor cells. This generates an increase in blood pressure, heart rate and myocardial contractility; in addition, chronic smoking induces rigidity in the arterial wall that can persist for a decade after smoking cessation 46.
There are several mechanisms through which alcohol elevates blood pressure; among these, an increase in sympathetic activity has been described, most likely related to the secretion of corticotropin-releasing hormone and the decrease in the vasopressor reflex via interaction with receptors in the nucleus tractus solitarii and rostral ventrolateral medulla 47.
Sex is also a determinant of AHT in Colombia. The data provided by the CARMELA study 20 show that in the young Colombian population, the prevalence of AHT is higher in males. However, in adulthood, this trend is reversed, and AHT becomes more prevalent in women. This epidemiological pattern is consistent with that reported in the study by the American Heart Association (AHA) and in the Framingham study 48-9. At present, AHT in older women is due to the loss of the protective role of estrogens. The reduction in estradiol levels and the imbalance in the estrogen/testosterone ratio resulting from menopause generate endothelial dysfunction and an increase in the body mass index. These factors result in increased sympathetic activity and the consequent release of renin, a determinant enzyme in the activation of the renin-angiotensin-aldosterone system, a hormonal system that regulates blood pressure. In turn, endothelial dysfunction is accompanied by a reduction in NO and an increase in endothelin levels, mechanisms that induce vasoconstriction and therefore increase blood pressure 50-2.
Cardona-Arias et al. 31 reported the alarming finding of an AHT prevalence of ~34% in the Emberá-Chamí people, a native population in which cardiometabolic disease had been thought not to exist. A similar prevalence rate was obtained in the study of an indigenous population residing in the regions of Norton Sound and Yukon-Kuskokwim in western Alaska, where there was a prevalence of 30% 56. This prevalence, which surpasses those found in urban populations in the same age range, is a reflection of the impact of the adoption of unhealthy behaviors within the indigenous population, secondary to a lack of knowledge of chronic diseases associated with unhealthy habits in this type of population.
Regarding distribution according to the area of residence, the urban area has the lowest prevalence of AHT. González et al. 29, whose sample resided in a rural area in the coffee zone, highlights that a low educational level is preponderant in the population and that this influences the presence of risk factors for the development of AHT. This conclusion is similar to that reached by Camacacho et al. in the PURE study; those researchers emphasized that AHT was consistently associated with a low educational level, especially in rural populations, where access to education is limited and there is a higher level of social inequity. In addition, the PURE-Colombia study showed that among hypertensive patients, only 51.9% were aware of the diagnosis, 46.6% were receiving treatment and 17.3% had controlled disease 12,36, findings that may be related to these inequalities.
In conclusion, the data compiled in this review provides an overview of this chronic disease in the country; an upward trend was observed over time, as was variability according to sex, age and geographic area. The estimation of AHT prevalence in Colombia can facilitate both public health surveillance in the country and the development of intervention and evaluation strategies. There is a need to establish a standard method for measuring blood pressure and to carry out further studies on hypertension in rural, young and indigenous populations in order to characterize them and design public policy interventions directed specifically towards these populations