











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkA 69-year-old male with high blood pressure, 50% LVEF heart failure, oxygen-dependent chronic obstructive pulmonary disease, a heavy smoking history and treated pulmonary tuberculosis was admitted to the emergency room due to mMRC 4/4 dyspnea, productive cough with yellow sputum, non-quantified fever, and diminished breath sounds. A chest x-ray showed left-sided diffuse heterogenous radiopacity and a high-resolution CT revealed left fibrothorax.
Fibrothorax is defined as the sequela of intense pleural inflammation, causing thickening and fibrosis 1,2. Transforming growth factor-beta (TGF-|3) plays the most important role 3. It occurs most often as a complication of empyema and hemothorax, but also in pulmonary tuberculosis, connective tissue diseases, uremia, paragonimiasis, radiation therapy, asbestosis and with medications such as ergot alkaloids 2-4. It is diagnosed by imaging. Treatment may be pharmacological, using systemic corticosteroids, or surgical with decortication 2,5. It has been associated with lung cancer 6.
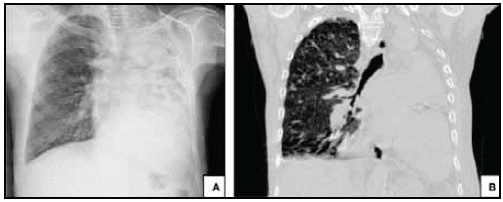
Figure 1 (A) AP chest x-ray showing diffuse heterogenous radiopacity of the left chest with associated ipsilateral loss of volume. Radiografía de tórax en proyección P-A. Evidencia radiopacidad difusa heterogénea del hemitorax izquierdo asociada perdida de volumen ipsilateral. (B) Coronal high-resolution CT in lung window projection showing loss of volume in the left lung with consolidation and varicose bronchiectases.

Figure 2 Chest computerized tomography image using an axial lung window. (A) and a mediastinal window; (B) sagittal mediastinal window; (C) showing left pleural thickening and calcifications. Free right pleural effusion. Mediastinal adenopathies. Cardiomegaly and precapillary pulmonary hypertension showing loss of left lung volume with consolidation and varicose bronchiectases.

