











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
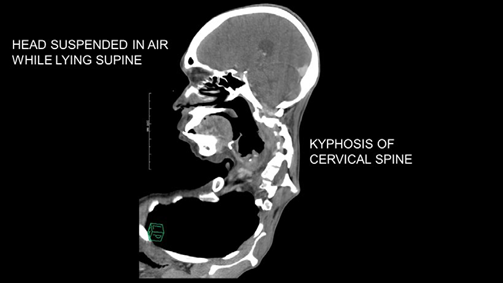
PermalinkCervical kyphoscoliosis is an uncommon spinal deformity. Kyphosis or outward curvature of cervical-spine (Image A) has led to a fixed flexion state resulting in suspension of patient's head in the air while lying on the imaging table. Additionally, dextroscoliosis or rightward convexity of the cervical vertebral axis has resulted in a persistent leftward head tilt (Image B). Head and neck radiation and trauma can lead to cervical kyphoscoliosis. In addition to the cosmetic deformity, patients present with myelopathic sensorimotor symptoms such as weakness and tingling of upper extremities. The Poisson effect states that flexion of the spine lengthens and stretches the spinal canal, reduces its area and narrows its lumen. This causes spinal cord impingement and myelopathy.1

An anterior-posterior surgical approach is often needed for deformity correction. Inability to achieve the "sniffing" position, laryngeal shift away from the midline and limited neck extension, make airway management challenging, often necessitating an awake fiber-optic intubation.1,2 Invasive arterial monitoring and large-bore vascular access are essential in view of possible prolonged surgical duration and heightened risk of profuse bleeding. In conjunction with prone position, these conditions confer a higher risk for perioperative vision loss, warranting a preoperative discussion with patients.
In addition to avoiding direct pressure on the eyes, positioning the head at or above the level of the heart may help decrease risk of vision loss. Although reverse Trendelenburg maneuver aids in achieving appropriate head positioning, it increases risk of venous air embolism.3 Propofol and remifentanil infusions facilitate evoked potential monitoring without interfering with signal acquisition or interpretation while vasopressor infusions may be required to maintain systemic and spinal cord perfusion. It is prudent to delay extubation after prolonged surgery. Airway distortion from edema and potential cervical hematoma can render ventilation via a mask or supraglottic device ineffective and hamper re-intubation efforts.1,4

