











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Cardiovascular disease has become a major worldwide problem and is a serious health threat that causes numerous biological, psychological and social problems and is one of the leading causes of death and disability.1 These diseases also impose a huge cost on the health system of countries.2 According to the World Health Organization, 17.7 million people died of cardiovascular diseases in 2016, and cardiovascular diseases account for 31% of all global deaths.3 According to the Global Borden Disease Study Center in Iran, the rate of death from cardiovascular disease has increased from 31.9% in 1990 to 46.8% in a decade,4) and represent 43% of the total number of deaths.3) Coronary Artery Bypass Graft (CABG) surgery is one of the most commonly used surgical procedures for patients with coronary artery stenosis.5 Annually, 30 000 to 40 000 people undergo cardiac surgery, and CABG constitutes 50-60% of these surgeries.6) One of the frequent problems of patients before the surgery is higher levels of anxiety in this case as compared to that in other surgeries, since heart is closely related to human life and death.7
Actually Cardiac surgery is often associated with anxiety and fear in patients undergoing it.8) Anxiety before cardiac surgery can lead to stimulates the sympathetic system and significant changes in the patient's heart rate and blood pressure,9,10 elevates the risk of mortality,11 increases the intraoperative anesthetic requirement and can prolonged recovery.12 ways to control anxiety include medication and non-medication.6 Routine use of anxiolytic medications to reduce anxiety in patients with pain can prevent the reporting of pain due to drowsiness, pulmonary complications due to reduce her ability to breathe deeply, get out of bed, or participate in treatment.7,13) Non-pharmacological approaches such as inhalation aromatherapy,14 massage therapy,15 and music therapy,16 Visitation by Operating Room Staff,17 and preoperative education programs18 can help reduce anxiety. Among the measures the nurse can take to minimize anxiety before cardiac surgery, giving information about surgery, promoting acquaintance dialogue, and understanding the patient are more important strategies.19
Given that the receptionist in the operating room is one of the last people the patient will be in contact with the patient before surgery, The researcher speculates that if this is a relationship with the patient who was already in touch with the patient, a positive interaction and Having a friendship between them will affect the patient's anxiety and vital signs. According to the researcher, no study has been conducted in this area, so the present study will be conducted to determine the interactive effect of preoperative consultation and patient admission in the operating room by counselor on the level of anxiety and vital signs in coronary artery bypass graft surgery (CABG).
Methods
The present study was a clinical trial study performed at Farshchian Hospital of Hamadan, Iran in April 2019. Using convenience sampling, 90 patients were selected for CABG surgery and were randomly divided into three groups (control, intervention 1 and intervention 2) using random sampling and weekly block method. The inclusion criteria were include the at least 18 years of age; fully conscious and knowledgeable regarding the time, place, and person; having the ability to communicate, not having a history of heart surgery, lacking physical and cognitive disorders; lacking medical education or what was related to it; not having a drug addiction; no prior medical diagnosis of anxiety and depression and not taking tranquilizer, anti-depressants, or anti-anxiety drugs at one month before surgery. The exclusion criteria were the unwillingness of patients to continue the participation in the study and their condition worsening during the study period.
The data collection tool consisted of three parts: personal traits, medical data, and Spielberg state anxiety Inventory. The state of anxiety is the same instantaneous individual anxiety expressing the person’s current feeling or emotion at a time period like getting prepared for the surgery. The Spielberg anxiety questionnaire had global validity and reliability. The validity of this test, in order to reach a meaningful result, the mean anxiety for the standard and normal community was compared at 1% and 5% across all age groups, indicating the validity of the measurement of anxiety. The reliability of the Spielberger's State-Trait Anxiety Inventory has been calculated to be 0.90 and 0.86 in the studies by Roohy et al. (20 and Safara et al., (21 respectively. In addition, its reliability and validity in the Iranian society cardiac patients was confirmed via the study of Akbarzade et al.22) The questionnaire was made up of 20 multiple choice questions, with the options of “very little, little, a lot, and very much”. The minimum score for this questionnaire was 20 and the maximum was 80.
After consenting to the samples at the first visit and before any intervention, the patient completed a three-part questionnaire as a pre-test. The control group received only the routine counseling program that the ward provides for all patients, but intervention 1 and intervention 2 group’s in accordance with Table 1 received two one-hour counseling sessions in the day before surgery in addition to the routine counseling program. Counseling sessions were organized individually for each patient by the counselor, counseling sessions were held in the conference room of the ward, and the counselor, the patient and the experienced nurse were present at these sessions. At admission to the operating room, the control group and the intervention group 1 samples were admitted to the operating room according to the routine program of the hospital with a non-consultant in the operating room. But in order to admission Intervention Group 2 patients in operating room, they were accompanied by a consultant and patient transfer team from the ward to the operating room; consultant would admitted the patient in the operating room and perform the tasks performed on the patient's admission in the operating room; while waiting for anesthesia, the consultant stayed with the patient and acted as an emotional support and mentor in the operating room for the patient by benefiting from the positive interaction that was created during the two meetings with the patient. Then before receiving anesthesia, their vital signs and state anxiety were recorded as a post-test.
At the beginning of the counseling program and after introducing herself to the patients and explaining the purpose of the study, the researcher obtained consent from all patients. Also, participants were assured that all information collected from them would remain confidential. Finally, the data resulting from descriptive statistics, independent T-test, analysis of variance, analysis of covariance and ANOVA at the significant level of p<0.05. Were analyzed by SPSS V.23.

Results
The results of this study showed that the mean age of the control, intervention 1 and intervention 2 groups were 61.9±8.02 years, 62.13±7.04 years, and 65.6±9.3 years, respectively and Mean BMI of the control, intervention 1 and intervention 2 groups were 24±3.2, 25.6±2.4 and 25.6±4 respectively In addition, no significant difference was observed in the age and BMI by the ANOVA test. Most of the patients in these three groups were male (68.9%) and most of the subjects were illiterate (55.6%) and the results of Chi-square test showed no significant difference between the three groups in terms of gender and education (Table 2).

One-way covariance analysis test was used to compare the pre-test score of anxiety variables and vital signs. According to the results, the p-values in the pre-test of the variables of heart rate, respiratory rate, systolic blood pressure and positional anxiety showed no significant difference between the three groups. But for the variables of temperature and diastolic blood pressure were significant at the 0.05 level (Table 3).

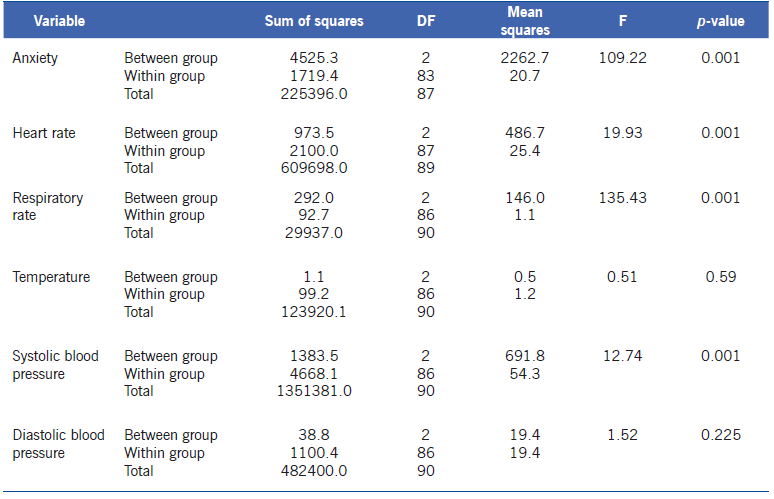
Covariance analysis test revealed that collaboration effect of preoperative counseling and patient admission in operating room by counselor on anxiety, heart rate, respiratory rate and systolic blood pressure has been meaningful, but it was not significant on temperature and diastolic blood pressure (Table 4).
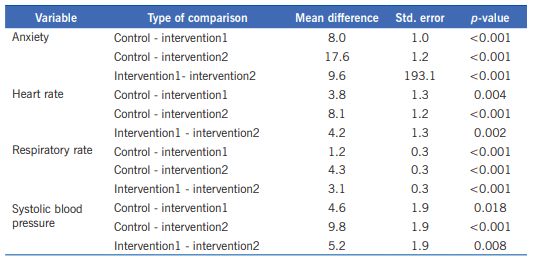
In the following, Tukey's post hoc test was used to compare two-way mean anxiety, respiratory rate and systolic blood pressure in the control and intervention groups. Based on the results, there was a significant difference in the level of anxiety between the control group and the intervention group 1 and 2 (p<0.001). There was also a significant difference in the level of anxiety between intervention group 1 and intervention 2 (p<0.001). accordingly, the mean of anxiety in intervention 2 was lower than the control group and intervention 1 and the mean of anxiety in intervention 1 group was lower than control group (Table 5).between the mean of heart rate in the control group with intervention 1 (p=0.004), between the mean of heart rate in the control group with intervention 2 (p=0.001) and between the mean of heart rate in the intervention 1 group with intervention 2 (p=0.002) there was a significant difference that mean of heart rate in intervention 2 was lower than the control group and intervention 1 and the mean of heart rate in intervention 1 group was lower than control group (Table 5).
Between the mean of respiratory rate in the control group with intervention 1 and 2 groups (p<0.001) and also between the mean of respiratory rate in the intervention group 1 and intervention 2 group (p<0.001) there was a significant difference. It’s that the mean of respiratory rate in intervention 2 was lower than the control group and intervention 1. The mean of respiratory rate in intervention 1 group was lower than control group (Table 5). Between the mean of systolic blood pressure in the control group with intervention 1 (p=0.018), between the mean of systolic blood pressure in the control group with intervention 2 (p<0.001) and between the mean of systolic blood pressure in the intervention 1 group with intervention 2 (p=0.008) there was a significant difference that the mean of systolic blood pressure in intervention 2 was lower than the control group and intervention 1 and the mean of systolic blood pressure in intervention 1 group was lower than control group (Table 5).
Discussion
The results of this study show that there is no significant difference between the pre-test anxiety scores of the three groups, which is in agreement with the results of studies such as Fazlollahpour et al.,23) Amiri et al.24 and Abbasi et al.25 It has also been shown that pre-test three vital signs including systolic blood pressure, heart rate, and respiratory rate were not significantly different between the three groups, which is consistent with the findings of Amiri et al.,24 Abbasi et al.25 and Hemmati et al.26 However, there were significant differences between the two groups in the pre-test of diastolic blood pressure and temperature variables, which is inconsistent with the results of Abbasi and Hemmati's study.25,26) The results show that there is a significant difference between the mean scores of post-test anxiety of the control group with the intervention group 1 and intervention 2, which Indicates the effectiveness of the preoperative counseling program that this consistent with the studies of Karama et al.,27 Rosiek et al.28 and Timurie et al.6
The results also show that there is a significant difference between the post-test scores of the two groups of intervention 1 and intervention 2, which indicates the effectiveness of consultant admission in the operating room which no relevant article has been found in relation to this finding to compare the results that this indicating the novelty and importance of this study.
This study showed that there is a significant difference between the three variables of heart rate, respiration and systolic blood pressure in the control group with the intervention group 1 and intervention group 2, which indicates the effectiveness of preoperative counseling on these variables. This is consistent with the findings of the study by Amiri et al.,24) Hasan Genc et al.,29) Degirmen et al.,30) but is inconsistent with the results of the study by García Sierra et al.31 The results also indicate that there is a significant difference in pre-test of these three variables between the two groups of intervention group 1 and intervention group 2 which indicates the effectiveness of consultant admission in the operating room on these variables no study was found to compare these results that this indicating the novelty and importance of this study. But the results of this study showed that comparison of post-test and pre-test two variables of temperature and diastolic blood pressure were not significantly different in the three groups. This finding is in line with the results of studies such as the García Sierra et al.31 and is inconsistent with the findings of the Zarei et al.,32) and Degirmen et al. (30) studies.
Based on the findings, it can be concluded that preoperative consultation and admission in operating room by counselor can reduce the level of anxiety and stability of vital signs in patients. According to the data it can be decided that the admission in operating room by counselor will increase the effectiveness of the surgical consultation, reduce the level of anxiety and stabilize the vital signs of the patients. This approach can be considered as a strength and superiority of the present study than previous studies which suggest that cardiac surgery centers should adopt these results in order to reduce the anxiety and stability of the vital symptoms of patients.

