











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalinkintroduction
Falls are defined as involuntary events that cause an individual lost of balance and strike his/her body against the ground or other firm surface, halting the individual 1. Approximately 30% of adults older than 65 years of age fall each year 2 with an annual incidence among the population increasing by 25% at 70 years old and by 35% after age 75 3; added to this, being female represents a higher risk factor for falls, according to the systematic review made by Gama et al 4. The high incidence of falls combined with a high susceptibility to injury is a concern in this population 2, as the increase in falls directly escalates the health and social costs associated with treatment and rehabilitation; and indirectly aspects related to losing functionality 4.
Early identification of older individuals who are at risk of falling is crucial for beginning fall prevention strategies. Many of these occur while older individuals are performing mobility tasks such as rising from a chair or walking 5.
The accumulation of organic and cognitive deficits frequently presented in older adults, that together generate or predispose to muscle weakness, decreased balance or neuromuscular abnormalities, result in mobility changes that can cause falls and make daily life activities difficult 3. Likewise, age and cognitive impairment are associated to changes in a proper performance of gait and balance control. Recent research based on the performance of double motor tasks for screening the risk of falls stresses that walking requires more attention, effort, and coordination in older adults than in younger ones 6. Such findings prompt the consideration of falls in older adults as a multifactorial process that involves a double task in which walking is accompanied by a second cognitive or motor task.
Considering that 98% of accidents resulting from falls are highly preventable 5, it is important to assess fall risk using physical tests and then generate tools to reduce falls and their consequences.
There are several tools used to assess the risk of falling. Among them, the Tinetti and Berg scale is remarkable, which assesses the risk of falling by evaluating aspects such as the execution of gait, and equilibrium 7, and the Timed Get Up and Go Test (TGUG) that has been established as an effective method for assessing mobility and quantifying locomotor performance 3. The latest version of this test, known as the modified version of the Timed Get Up and Go Test (TGUGM), arises from the need to evaluate double motor tasks, mimicking everyday processes in older adults and making evident in them two functions: one cognitive and another motor, which allows evaluating cognition with the motor component in gait added to the individual's coordination and balance 8. Evaluating the risk of falling with the TGUGM would then imply a possible relationship not only between age and risk of falling, as it has been documented so far 9, but also between falls and the educational level.
This study applies up the TGUGM test considering that this screen the risk of falling using a double motor task and, based on it, seeks to determine if there is an association between the risk of falling, age and educational level in older active women.
METHOD
The study is part of the investigation developed by the group of research on human body movement of the Department of Nursing and Rehabilitation, at the University of La Sabana (Colombia), and had its approval and ethical verification. This is descriptive, cross-sectional study.
Participants
The sample included 200 women older than 55 years of age who were participants in a physical activity program at the town hall of Chía, Cundinamarca (Colombia). Individuals with cognitive deficiencies that prevented them from following simple orders, those who were unable to walk independently or with some external assistance, those with low back pain that was currently being exacerbated, those with vestibular or central nervous system diagnoses, and those with orthostatic hypotension were excluded. All criteria were identified and evaluated by an initial interview that included social data and medical history. Participants provided their informed consent approved by Institutional research board.
Measurements
Age of the participants was obtained in complete years through direct interview and proved with data from clinical records. The educational level was determined through direct inquiry on the maximum level of education studied in the following way: no studies, elementary school, high school, and higher education including technical and university levels.
Other data obtained from the participants and that allowed a better characterization was marital status, occupation, history of falls in the last two years, number of drugs currently ingested, pathological background, visual or hearing problems. These last data correspond to the items evaluated on the Downton scale of risk of falls 10; this information was included in an evaluation form and then into the database analysis.
In order to assess the risk of falls, the TGUGM was administered. It is a physical test that measures balance and gait simultaneously to cognitive tasks, and it is subdivided into six phases that are scored by the time spent in each phase and the total time of the test, as well as a qualitative evaluation (QE) for each phase that uses a Likert scale from zero (deficient execution) to three (excellent execution). TGUGM has shown high and strong correlation with a) fast and normal gait speed test, b) five chair rises, c) single-leg balance time, d) Tinetti scale; and e) two maximal isometric quadriceps and hamstrings contraction strength 8.
The first phase of the TGUGM involves standing up from a 42-cm high chair in a stable way without using the hands for supporting. The second phase involves kicking a ball 19 cm diameter and weighing 0.2 kg in the strongest possible way without losing balance. The third phase involves walking toward a cone placed 10 meters from the chair, while counting from 15 to 0, without changing gait speed and without making mistakes during counting. Phase four involves turning around the cone; the rotation should be stable without touching the cone. Phase five involves stepping within rings arranged 60 cm apart; no steps should be made outside the rings. Finally, the sixth stage consists of sitting down in the chair using controlled movement and without hands support (figure 1). Following the rating of each phase of the test, a sum of each of the phases is performed to obtain a total. Scores under twelve indicate a risk of falling 7 (figure 1).
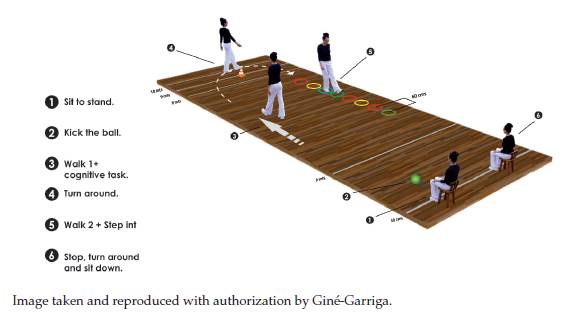
The instructions given to each participant performing the test were the following: "Sit with both of your hands resting on your legs. When you hear number three, stand upright without using your hands. Kick the ball that is in front of you as hard as possible using the foot with which you feel safety. Then, walk at your own pace speed while counting backwards from 15 to 0. Pass around the cone without touching it, and then return to the chair, stepping within the circles and trying not to touch any of the edges. Finally, sit down again, trying not to use your hands". An attempt was made by each participant prior to the actual test to verify an understanding of the instructions. The performance of each phase of the test was rated by means of the QE, that later were added, and each participant was provided with their total score and an explanation of its meaning. The maximum possible score achieved was 18.
Data analysis
A dichotomous variable that indicated the risk of falls was created from the result of the QE, being a score of 12 points or less a reference of a high risk of falling. The age range was classified in years and grouped in three: 55 to 65 years old, 66 to 75 years old and older than 75 years old. The educational level was classified in four levels: no studies, elementary school, high school, and higher education. Once the level of risk of falling was calculated, descriptive for all variables were obtained and associations with qualitative variables, such as age and educational level, were established using the chi-squared test. Data were analyzed with SPSS software, version 21.0.
RESULTS
The mean age of participants was 68.4 (SD: 7.6) years; where 40% between 55 and 65 years, 42% between 66 and 75, and 18% older than 75 years. In terms of educational level, 13% of the population declared no education, 50% elementary, meanwhile high school 22% and 14% higher education. Regarding the level of risk of falls, 23% presented a high risk of falls, while the remaining 77% had low risk (table 1).
The analysis of the relationship between education level, age and level of risk of falling reflected association between them (table 2).
Table 2 Association between educational level and the risk of falling according to the TGUGM
| Educational | Low risk | High risk | Sig. |
|---|---|---|---|
| level | |||
| No education | (12) 44.4 % | (15)55.6 % | |
| Elementary | (74) 74 % | (26) 26 % | 0.000 |
| High School | (43) 97.7 % | (1) 2.3 % | |
| Higher | (27) 93.1 % | (2) 6.9 % | |
| Age | |||
| 55-65 | (69) 86.40% | (11) 13.60% | |
| 66-75 | (64) 76.50% | (20) 23.50% | 0.017 |
| > 75 | (23) 62.90% | (13) 37.10% | |
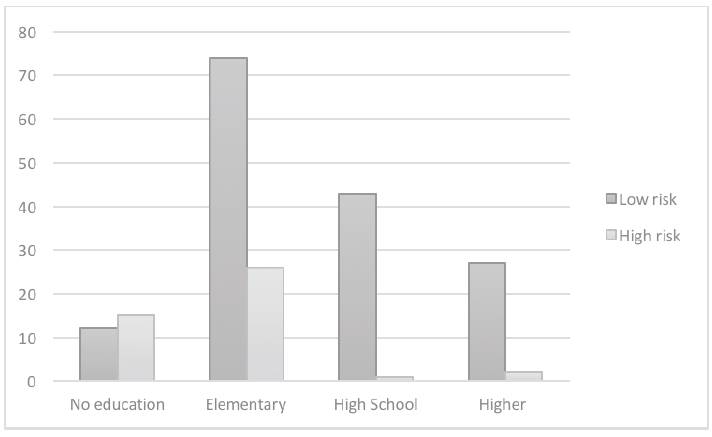
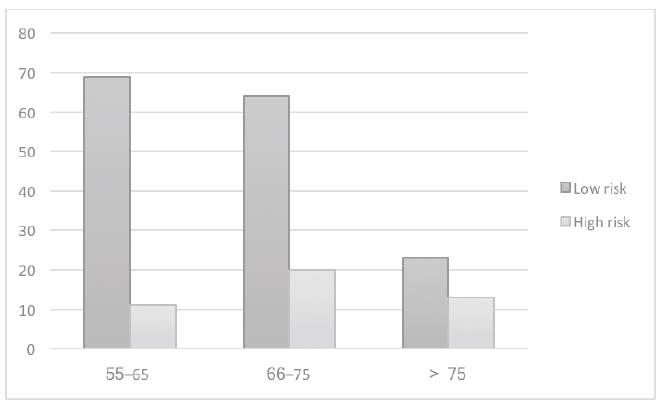
An inverse association appeared between the level of study and the risk of falling, where women with no studies had higher risk of falls (scores lower than 12 in the TGUGM); this probability decreases as the education level increases (figure 2). On the contrary, the association between age and the level of risk of falls was positive, as it was found that for women over 75 years, the risk of falling increases, showing that there is a less level of risk with a lower age (figure 3).
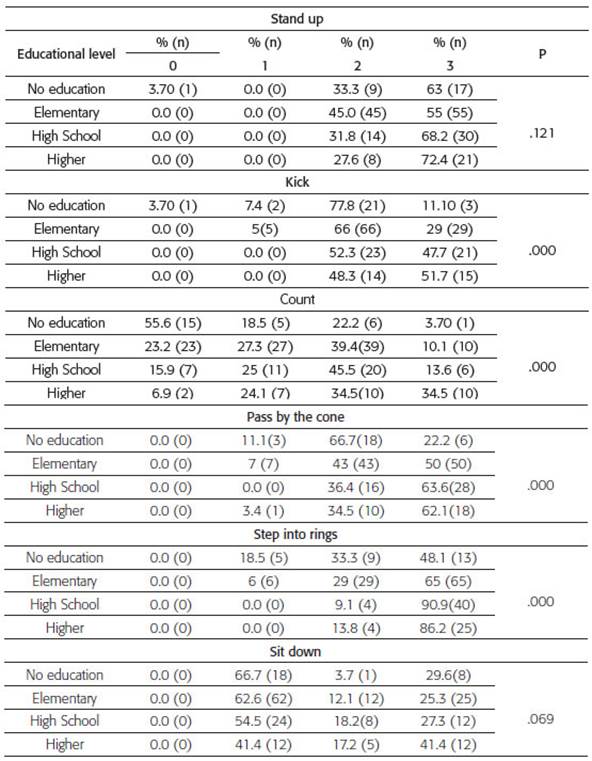
Phases two, three, and four of the test were related to educational level, while phases one and five were not (table 3). In the phase of hitting the ball it was found that the percentage of people achieving a score of three increases as the educational level does. The same was found in the stages of counting backwards, passing around the cone, and stepping within the rings, whereas for the standing up and sitting down phases, the percentages are homogeneous according to the educational level (table 3).
DISCUSSION
The influence of educational level and age on the level of risk of falling, assessed with the TGUGM, in Colombian women was found. That among this population has a low educational level, they could get less score in TGUGM. We found association among specific test items and level of education. It was evidenced in the possible influence of the results of the TGUGM in the double motor or cognitive task occurring from phase two to four of the TGUGM unlike the remaining phases. Similar results were reported by Gomes et al. 9, who found that high levels of education and cognitive functioning can positively influence performance on the TGUG, as better cognitive performance was observed in subjects with higher education.
Another influential aspect is that most falls occur when older people perform cognitive and motor tasks associated with walking during daily activities. There is evidence that these double tasks change motor patterns and that walking should no longer be considered to be purely a motor activity in older persons, as it is for young adults 11. The previous information is directly related to the own results when associating the test phases of kicking the ball, counting backwards, passing around the cone, and stepping within the rings. During these tasks, adults require strength, balance, and the execution of a cognitive task in parallel with the motor action of walking, being highly influential when determining the fall risk, as gait changes that are directly related to the addition of a secondary task have been associated with falls in cognitively intact older adults 12,13.
For this reason, tests that share a common core of double task, created for studying the interrelationships between the motor and cognitive systems when both tasks are executed simultaneously, allow making evident whether there is an alteration in the performance or rendition of the gait when executing the double task 14.
In addition to our results, some studies confirm the importance of the double task in evaluating the risk of falling in healthy older adults 15,12. However, other researchers report that the evaluation of walking, in which a double task is included, does not provide any additional benefit over standard evaluations 16.
Hauer, Marburger, and Oster 15 sought to evaluate the influence of simultaneous cognitive tasks on the motor performance of older adults (mean: 80 years) with a history of previous falls. This study concluded that in older adults, additional cognitive tasks can substantially diminish motor performance, affirming once again the findings of our study, as they present a similar correlation with respect to the cognitive and motor interaction. Chen et al. 17 reported a lower motor performance among older adults in performing a three-part task (giving verbal responses and overcoming obstacles during walking). Other studies also reported decreased performance in the mobility of older individuals by combining motor tasks and walking 17,18. These results could be explained by the interference of cognitive functions that require divided attention between two tasks, combined with a low educational level, which directly influences performance and development of the mentioned test. This study corroborates that performance in physical tests TGUGM is negatively associated with age having lower performance as age advances 12,19,20,21.
CONCLUSIONS
This study found that there is negative association between educational level of women and the level of risk of falls and positive association between advanced age and level of risk of falls valued with TGUGM.
The TGUGM test facilitated the assessment of the risk of falls and allowed better understanding of the performance of older women discriminating tasks where test components move towards a cone set 10 meters away from the chair while a count of 15 to 0 is made without changing the walking speed and without errors in counting and turn around a cone stably without touching it, are relevant components in the detection of risk within the test.
These findings allow us to suggest that interventions to reduce the risk of falls in active adult and older adult women should take into consideration both their age and educational level. It is important to continue using comprehensive and inexpensive screenings like the TGUGM, which promotes holistic interventions without separating the results of the physical evidence of other aspects that influence the people's performance.

