











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The analysis of physical condition and cardiovascular resistance in the university environment has become vital, bearing in mind the current concern for young people to adopt healthy lifestyles1. Many researchers seek to understand and standardize the states of health and physical condition by conducting various field and laboratory tests, with the purpose of establishing physical performance, cardiovascular and ventilatory behavior–indicators that reflect the physical state of each individual–from the VO2max obtained2.
At the university level, field testing is an easy tool to work with and it delivers information rapidly regarding student’s “performance”3. It is important to point out that the universities that offer professional careers associated with the field of physical activity and sports use these tests as a filter to register in their schools. Also, the curriculum of these studies includes the study of these tests, and its recognition, as part of the academic process4. However, submaximal tests that allow evaluating cardiorespiratory fitness also have important applicability in the clinical setting, since they enable predicting maximum aerobic capacity.
Nevertheless, results’ validity and reliability obtained from these tests should be related to other control variables such as heart rate, blood pressure, effort perceived by the subject and pain as complementary strategies that initially guarantee patient safety during the time to apply the tests and provide greater objectivity in the assessment5.
According to García et al.6, in their systematic review, it was concluded that field tests could be used to calculate VO2max quickly and at low cost in untrained healthy adults. It is fundamental to consider not only hemodynamic variables but factors such as age, sex, and physical condition. However, in users with pathologies, it is recommended to check that the field tests to be used are following their current health condition.
Physiological adaptations at moderate altitudes can potentially alter VO2max estimation when either field or laboratory tests are applied. Aspects such as the perception of maximum effort, central peripheral fatigue, and cognitive performance can lead to changes in pH, hemoglobin mass, and pulmonary hemodynamics7.
In addition, when these tests are given at altitudes exceeding 1,500 meters above sea level, hypobaric hypoxia can cause a significant reduction in VO2max, compromising performance when test-taking, underestimating, or overestimating the values of VO2max obtained. For an altitude of 2,000-2,500 meters above sea level, the maximum oxygen consumption is reduced approximately 12-15%, which is determined mainly by the reduced partial pressure of oxygen in the inspired air. Several research studies have shown that the decrease in maximum oxygen consumption in elite athletes is evident and significant, starting at 900 meters, which could lead to essential performance implications. However, some tests were developed at sea level, low altitude, and for the most part, have not been validated at a moderate height, except for a study reported by Falgairette et al.8, in children at 3700 masl.
In fact, considering the studies of Terrados9 and Bernal et al.,10, the classification of altitude is due to factors such as latitude, temperature, among other environmental characteristics, so a categorization with respect to meters above the sea level (masl), is proposed. In this sense, high height or height is those locations between 2000 – 5000 meters above sea level, in which it has been observed that significant physiological modifications can occur both at rest and during physical exertion.
VO2max values decrease due to different external and internal factors. Among them, the most important for the development of this study is altitude. However, the results obtained are derived from the association between distance and time constants, gender, age, height, weight. It should be noted that other studies have shown that there are other genetic adaptations present in people living at moderate altitude, related to mitochondrial density and effectiveness, which to a certain extent would allow better physical performance, but it is necessary to understand that this will be influenced in a way direct as anthropometric variables are modulated11.
Many field tests allow estimating VO2max and can be applied considering the primary physiological conditions of the subjects to be evaluated. One of them is the Cooper test (CRT), which has clear methodological considerations for its application. As part of the application protocol, it is ideal for it to be performed on an athletics track (400 m), delimited every 100 m to verify the actual distance obtained during the 12 minutes of execution. It is highlighted that it is one of the first tests developed to indirectly estimate VO2max, easy to apply, and with excellent reliability reported in several articles12.
According to Bandyopadhyay, it is stated that it may have an optimal validity coefficient to determine the cardiorespiratory condition. The prediction equation used to predict VO.max was [Y x 21.01X – 11.04 (SEE x 0.193 ml - kg - 1 min - 1 min)], from which the results obtained by correlation tests were calculated. There was a statistical significance (r= 0.93, p<0.001) between the distance covered in CRT and VO2max, as long as they are controlled: race speed, time, environmental factors such as execution time and emotional elements of the participant13,14.
Another validated test that allows determining the VO2max is the Course Navette test (SRT–20m), which has differentiated methodological indications that are preferably performed in an open field. For its development, two cones with a separation distance of 20 meters are placed, and the participants will have to run that distance at speed. The frequency will be mediated by audio, which modulates the initial rate, starting at 8.5 km/h, increasing 0.5 km/h for each minute. The VO2max estimate proposes various validated equations from Leger’s study using as a formula (5 857 x Speed (km/h– 19 458), taken up in several studies by Duperly et al.7, and García et al.6, which report that this test has been applied in other disciplines demonstrating its validity, which is associated with changes in rhythm that favor the motivation and concentration of the participant.
In accordance with the above, there are other investigations which establish that the correlation between SRT-20m and the values obtained in laboratory tests is high, making it a valid and sensitive test capable of replicating in various population groups3. However, it was pointed out in a study, carried out in elite athletes at moderate altitude that hypobaric hypoxia may be a factor that, in an acute way, can have a notable impact on athlete’s sports performance, but that if it is used as a training element seeking to “acclimatize” athletes, its positive effects can be decisive when evaluating aerobic resistance12.
Currently, there is an investigative gap regarding studies with subjects born at moderate altitudes, which allow us to define whether the VO2max data provided by indirect tests such as SRT-20 m and CRT are predictors and resemble the data obtained in ergospirometry. Additionally, the information reviewed does not establish whether the data obtained in a submaximal test is reliable or underestimates the resistance capacity of the subjects. These tests were developed at low altitudes. However, currently are being used the same scores to classify the population.
The FUPRECOL15 study was used as a correction factor, using an exponential regression model whose constant was 1.11 to adjust the results of VO2max in relation with altitude of the city of Bogotá, as it adjusts variables such as temperature, height above sea level and the production potential of hemoglobin, since previous studies report 10% for each 1000 m above 1500 m. It was applied to calculate values adjusted by a correction factor of 1.11 considering Bogota’s altitude (2625 masl) on cardiorespiratory fitness assessment16,17,18.
Based on the above, the objective of this study was to compare the VO2max of men and women obtained by two field tests (CRT and SRT-20m) with the VO2max evaluated using ergospirometry at high altitude, with the aim of establishing which of these two indirect tests approaches the values of VO2max obtained directly.
Materials and methods
Non-experimental cross-sectional descriptive study, which inscribed a total of 30 physically active subjects (8 women, 22 men), with an average age of 19.0±2.2 years for women and 20.1±2.1 years for males who were considered potentially eligible.
The selection of subjects was based on the following inclusion criteria: i) being of legal age; ii) have been born or resident in the city of Bogota, or municipalities of the metropolitan area above 2600 meters; iii) be physically active or practitioners of some endurance sporting discipline for a time not less than one year; and iv) have no medical precedent or restriction that makes participation impossible during the execution of physical tests. Subjects with medical restrictions or no physical activity reported at least three times a week, which was evaluated with the Ipaq short version physical activity questionnaire, weren’t considered. All participants in this study were active university students from 2nd to 8th semester of the undergraduate degree in Physical Culture, Recreation and Sport of the Universidad Santo Tomás.
Endorsement for test delivery was given by the ethics committee of the Universidad Manuela Beltrán, reference number CEI-170528-27, under the framework of the Teaching - Research agreement with the Universidad Santo Tomás. Each participant received information regarding the objective of the study and signed the informed consent considering the ethical and regulatory guidelines of the Declaration of Helsinki (1961)19.
The CRT was applied on an athletics track (400 m) at Santo Tomás University from Bogotá, Colombia; athletic tracks were marked every 100 m to determine distance traveled. The following equation was used to estimate the VO2max: VO2max=22.351 x Distance (Km.) - 11.2883,4,12. On the other hand, the application of the SRT-20m was carried out in the same facilities of the Universidad Santo Tomás, with eight days of difference after the application of the CRT to give space to the muscle recovery of the participant. This test was performed in an open field with a flat and stable surface where two cones with 20 meters of separation between them were installed. The SRT-20m was performed on a covered field with a start speed of 8.5 km/h, which was increased 0.5 km/h every minute. For the calculation of VO2max the following formula was used: VO2max=5.857 x Speed (Km/h) - 19.458 5,8,15,17. Participants were quoted in the morning hours (between 8–10 AM, GMT-5), times when exposure to sunlight was not so intense as to reduce each subject’s physical performance, and thus, avoid biases in the results.
8 days after the SRT-20m test, the students were summoned for ergospirometry; the students performed the treadmill stress test (1° incline) with an exhaled gas analyzer (Metamax® 3B) using a stepped protocol that starts at 6 km/h, increasing 1km/h every 2 minutes without changing the initial band incline; each participant was given pre-ergospirometry indications such as: don´t eat three hours before, avoiding the use of coffee, ergogenic drinks, alcohol, or tobacco three hours before the test was performed. In addition, they were instructed to avoid any intense physical activity or unusual exercise within twelve hours prior to the application of the test. All tests were conducted after warming up. Statistical analysis was performed using the SPSS® Statistics version 25 for Windows. The Shapiro-Wilk test and the Levene test were used to evaluate normality and homogeneity of variance; and the paired sample T test was used for the comparison between the VO2max obtained by the field tests and the direct test. Direct and indirect oxygen consumption data by CRT and SRT-20m were adjusted to a normal distribution curve (Shapiro-Wilk; p>0.05), therefore, a one-way variance analysis was applied.
Results
The data reported in this study was obtained from the total number of potentially eligible participants (8 women and 22 men), who met the inclusion criteria and completed the physical tests successfully. Table 1 shows the descriptive characteristics of the population evaluated, as well as the results of VO2max obtained through the application of CRT, SRT-20m and ergospirometry. (Table 1)
Table 1 Characteristics of the population and study variables (n=30).

*Mean ± Standard Deviation; BMI: Body mass index; CRT: Cooper run test; SRT20m: Shuttle run test.
Figure 1 shows the behavior of men who showed statistically significant differences between the VO2max evaluated directly and using the Cooper Test (p<0.001). There were also differences between the VO2max in the ergospirometry test and the Leger test (SRT-20m p <0.001). However, in women there were no differences between the VO2max evaluated by ergospirometry and the field tests (CRT p=0.081, SRT-20m p=0.604). (Figure 1)
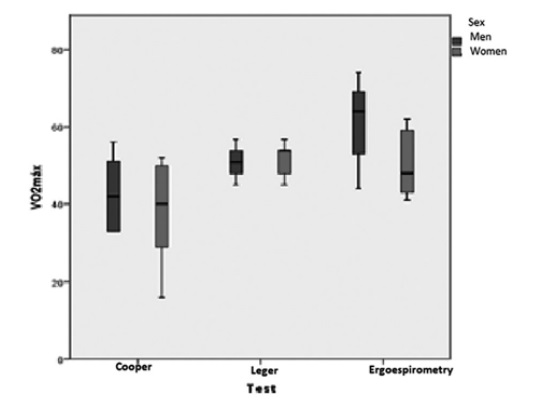
Source: authors
Figure 1 VO2max obtained by Cooper test, Leger test andergospirometry in men and women
Direct and indirect oxygen consumption data by Cooper and Leger were adjusted to a normal distribution curve (Shapiro -Wilk; p>0.05), therefore a one-way variance analysis was applied. The descriptive characteristics and their corresponding level of significance are shown in the following table: (Table 2)

According to the Levene statistic, the data doesn’t meet the assumption of variance homogeneity (p<0.01). Therefore, the significance value of the ANOVA is performed with the welch adjustment (p<0.01), showing differences in the mean of VO.max between the groups. A post hoc analysis was performed with the Games-Howell procedure which is most powerful in small samples and its results are shown in the following graph: (Figure 2)

No significant differences were found in the mean for VO2max of the SRT-20m and the direct method, however, with respect to the CRT, differences were presented (p<0.01), reflecting the increased accuracy of the SRT-20m test to estimate the VO2max in the sample evaluated.
Discussion
Considering the objective of the research, which was based on a comparison between the VO.max obtained by two field tests against a laboratory test in university students living at high altitude, it can be specified that, according to the results obtained, differences in VO2max were found in both men and women, showing in men higher values compared to women, in the three tests performed. This could be related to own factors derived from the morpho functional characteristics that differentiate each sex. This coincides with the study of Fernández et al.20, who made comparisons between VO.max obtained for men and women, finding that in women factors such as the distribution of lean mass and fat change their performance compared to men; on the other hand, hormonal influence, the development of muscle mass along with the level of physical activity should be variable analysis for both sexes.
According with our results obtained, statistically, significant differences between SRT-20m and ergospirometry were not found. In CRT differences were presented (p<0.01), reflecting the increased accuracy of the SRT-20m test to estimate the VO2max in the sample evaluated. This coincides with the review proposed by García et al.21, who after analyzing 30 years of the application of the SRT-20m test, manage to conclude that this test is one of the most used to determine the cardiorespiratory fitness of any sex-independent subject, at any stage of its life cycle since it presents adequate correlations in the VO2max values obtained when compared to other tests such as ergospirometry; however, it has shown good sensitivity when analyzing subjects with different levels of physical condition so it can promote the diagnosis of the health condition.
Therefore, we suggest performing more studies to compare direct and indirect trials at these altitudes and increase population size. However, the field test that most closely approached the VO2max values of the direct test for males was SRT-20m, with the fact that sound stimulation affects the results, causing a variation in execution time and speed, as well as in their level of competitiveness.
Regarding the results obtained in CRT, this coincides with the research by Batista et al22, they compared three test CRT, mile test and SRT-20m to estimate the VO2max and their concluded results indicated that the CRT and MILHA test overestimated (0.9 and 6.9%, respectively) and the SR-20m analysis underestimated (8.5%). However, no statistically significant difference was found (p> 0.05).
In the literature, most studies have developed several regression models for the prediction of VO2max based on a variety of maximal tests in treadmill; a direct estimation of VO2max with more precision has been developed in many stress-testing laboratories into the assessment for cardiovascular fitness. However, when comparing direct test with an indirect test, only studies that applied the regression models correlated moderately with the measured values of VO2max19,23,24.
However, some research has proven that SRT-20m is the validated test at a different altitude. For example, Falgairrete et al.8, carried out measurements between 300 to 3700 masl, affirming that SRT-20m underestimated VO2max obtained in the laboratory, but is more stable to predict physical condition in different ages. In the study proposed by Duperly et al.7, where 64 young adults residing in the city of Bogota, Colombia, were evaluated, it was concluded that cardiorespiratory fitness can be estimated by the VO2max obtained in direct and indirect tests; however, within the field tests with greater validity, they point to the SRT-20m as the most suitable for determining VO2max in population living at high altitude, this being similar to what was reported by Ramírez et al.15, who evaluated this same test in schoolchildren, finding closeness among the values reported by the SRT-20m compared to laboratory test data; however, these authors indicate the importance of applying a correction factor; in order to adjust aspects that at high altitudes become analysis variables such as: temperature, humidity, barometric pressure and physiological adaptations of subjects.
The findings in women have been lower than men. These results may be associated with differences related to training objectives or the preference for the development of specific physical capacities. However, Torres-Luque et al.25, found that physical performance between men and women presents fundamental changes from the age of 11, however, given the imminent hormonal development and its impact on anthropometric markers such as weight and height, qualities such as aerobic resistance tends to decrease, a situation that agrees with our results, which reflect a low performance in the resistance tests26. Despite the above, it is necessary to recognize the difference in sample size between men and women, so it is necessary to increase the number of women participating in the study, to make conclusive statements.
According to the study of Morales et al.27, both CRT and SRT-20m allow to establish the VO2max; however, CRT measures aerobic resistance, while SRT-20m measures aerobic power; these aspects are essential if considered that in the case of cyclic sports the CRT turns out to be the optimal test to estimate cardiorespiratory fitness where the time factor and distance traveled are fundamental basis of this type of sports disciplines. In acyclic sports the SRT-20m, allows to determine much better the VO2max since it analyzes variables such as speed and time, which vary as the stage increases, being a test that resembles the motor gesture of acyclic sports.
Establishing why SRT-20m shows higher VO2max values could be associated with the objective of SRT-20m being the determination of aerobic power, which differs significantly from the CRT objective. On the other hand, sound stimulation affects as a variation in the participant’s time and speed of execution, which would lead to higher concentration and less motivation of the subject, on the contrary to what happens with the CRT where the invariance existing in the test, sometimes makes it monotonous and would only focus on evaluating a quantity of work done, regardless of time, speed, and distance traveled28,29,30,31.
However, it is clear to establish that ergospirometry is considered a “gold standard” that allows the determination of cardiorespiratory fitness in subjects. When comparing the VO2max data obtained between the field tests and spirometry, a more related relationship was found between CRT and the direct test. The CRT is a continuous test with characteristics like those used in the direct protocol, allowing to establish the cardiorespiratory condition and resistance training of the participants24,25,31,32.
In the future, it will be necessary research to analyze these data, not only around gender issues but considering the participant’s sports gesture, since the VO.max values for the CRT and SRT-20m could vary due to the metabolic axis of the sports discipline, the training load, the changes of rhythm and the participant’s objective.
As part of the limitations, the reduction in the sample size of women compared to that of men is recognized, a situation that prevents making better claims around performance during testing; aspects such as not knowing the ovulatory conditions or time of ovulatory cycle in which the women were located could lead to biases in the results. Another aspect relates to the non-classification of the type of exercise practiced by the participants, since the motor gesture affects the performance of each test applied. Finally, it is essential to establish climatic and environmental conditions during field and laboratory tests, to have a better understanding of the tests.
Conclusions
The SRT-20m test allowed to establish VO2max appropriately in the population evaluated, additionally, its values resemble those obtained in laboratory tests such as ergospirometry. It is important to consider the sports discipline of the participants to select the test more in line with the motor gesture, in order to obtain more appropriate results.

