











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Intestinal coccidia are intracellular protozoa of the intestinal epithelium classified taxonomically in the Phylum Apicomplexa. It´s have a life cycle that includes asexual and sexual reproductive stages, producing resistant parasitic stages called oocysts that are expelled into the environment and allow the spread of infection1. Its epidemiological significance is associated with opportunistic infections responsible for a high morbi-mortality in individuals with HIV/AIDS, intestinal coccidia are also involved in acute diarrhea commonly selflimited in immunocompetent2.
Cryptosporidium spp., Cyclospora cayetanensis and Cystoisospora belli are the most frequent agents involved in coccidiosis, have a cosmopolitan distribution; however, are reported more frequently in developing countries, especially in tropical and subtropical zones3. The species of the genus Cryptosporidium, have been reported in reptiles, fish, birds and mammals mainly4. Taking into account its zoonotic potential, Cryptosporidium can also be transmitted person to person through feces, consumption of contaminated food, additionally it has been described that water constitutes a vehicle for this coccidian, since it resists the purification techniques. Oocysts are acidresistant alcohol can be of two types: thick-walled that are released with fecal matter, have infective capacity once expelled, and are resistant to environmental conditions, on the other hand thin-walled that are related to infection endogenous or autoinfection. Cryptosporidium spp. is the etiological agent of cryptosporidiasis emergent associated with acute and chronic diarrhea whose morbidity and severity of symptoms are related to the immune status of the host. The cryptosporidiasis was considered a serious public health problem in 1993 due to an outbreak in Milwaukee Wisconsin caused by contaminated water consumption where more than 400,000 people were affected5. Equally, C. cayetanensis is the agent of endemic parasitosis worldwide, whose first case reported in humans was from Papua New Guinea5. The resistant acid-alcohol oocysts sporulated in the environment, so a direct person-to-person transmission by fecal matter is rare. They have recovered from water sources, soil and food by infecting through the oral route immunocompetent and immunosuppressed individuals who produce acute inflammation, shortening and widening of the villa6. For another hand, Cystoisospora belli is responsable for human cystoisosporiasis which has a worldwide distribution, is more frequent in tropical regions and its association with HIV patients has been described7, transplant patients, with lymphomas, leukemias, considering itself a pathogen opportunistic and generating a serious clinical conditions under immunosuppression. It is also associated with traveler’s diarrhea.
Commonly founded in the Tropical regions as Africa (subSaharan Africa), Latin America and the Caribbean and Asia. Have been observed a variability in epidemiological frequency into 1 - 40 % prevalence infection by coccidia, and that may be increase in situation related with HIV/AIDS infected patients. Therefore, these types of individuals due to immune commitment are disadvantaged, and it’s evidenced by the progressive increase in prevalence in the population, which are identified in the common and differential clinical manifestations. However, the symptomatic description starts from a series of causes that are initiated from the transmission and incubation of these agents inside the enterocyte where it achieves its differentiation and multiplication, and therefore it is exacerbated in patients with this type of alterations in the health.
It has been shown that those coccidia are frequently reported species in patients suffering from HIV/AIDS, whose clinical conditions at the gastrointestinal level such as excessive bowel movements and poor nutrition are observed, the direct causes due to infection and spread within the system is initially evidencing an apical complex consisting of structures such as rhoptries, micronemes and conoids that allows them to internalize and reproduce in the enterocyte, this internalization of invasive forms induces a proliferative development of sexual and asexual forms that they continue successively its life cycles8; mainly due to the contribution of virulence factors that will facilitate interactions with the host cell, developing encysting, anchoring, motility, parasitophorous vacuole formation and the own damage generated at the level of enterocytic cells9. Many of these mechanisms are related to the functioning of adhesion molecules (CSL, Gp900 reported in Cryptosporidium spp.)10, invasion and survival inside the host cells. It also increases the pathogenic aspects and susceptibility at the intestinal level in patients with HIV/AIDS are reflected in the activation of proteases capable of damaging the epithelium and inside the enterocyte, subsequently triggering an inadequate immunological response, with the expression of mediators and pro-inflammatory cytokines9. Alike, at the level of intestinal cells, ruptures of junctions between cells with increased mitotic activity are induced, alterations in the microvilli that condition the emergence of the malabsorption syndrome, as well as cellular involvement with increased permeability and eosinophilic infiltrations. Comparable, as infection in immunocompetent individuals producing self-limited watery diarrhea, with abdominal pain, steatorrhea and peripheral eosinophilia11.
However, due to few epidemiological reports of coccidia in worldwide and Tropical regions as Colombia is necessary realize a detailed review with respect to presence of these microorganisms and areas with poor reports, offers a new dates, criterion and perspectives of scenery of presence of these species in national territory and its implications in the health of the population.
Material and Methods
We searched PubMed, Scielo, ScienceDirect and Google Scholar databases for studies reporting Cryptosporidium, Cyclospora cayetanensis and Cystoisospora belli infection in normal patients and HIV-infected populations from May and October 2018. The databases were searched using the term “Cryptosporidium”, “cryptosporidiosis”, “Cyclospora cayetanensis”, “cyclosporiasis”, “Cystoisospora belli” and “cystoisosporiasis” combined by cross-referenced employed term as “HIV”, “immunodeficiency”, “immunocompromised”, “immunocompetent”, “AIDS”, without language restriction.
Selection dates criterio
The included studies in this review were based in reports populations, epidemiological behavior and presence of coccidian in normal and HIV- infected communities, were needed obtain raw data to calculate the prevalence of Cryptosporidium, C. cayetanensis, and C. belli infection. We excluded studies as reviews or repeated studies; likewise, were not selected studies that present sample size was less than 20; or if the diagnostic methods of parasite infection were establishing. The reviewers examined titles, abstracts and keywords of the search, thus considered the full text considered great relevant. For condensation and data analysis the reviewers extracted the information related with the first author, reported year of selection sample of the publication, country of the study, calculated prevalences associated to HIV-infected and uninfected populations and its relationship with reported coccidia, type of sample and diagnostic techniques.
Results
In this review research were identified 2.365 publications related with ours studied thematic. After primary screening and excluded of duplicates, were evaluated 326 articles of selective form. Likewise, of these, 119 articles were excluded for present insufficient data that were required according to the criteria of this review, 76 were unavailable for full text and 67 present duplicate samples. Following, 64 articles were selected for review full-text of content and have been distributed in reports of prevalence’s of worldwide and Colombia, including 55 and 12 articles, respectively (Figure 1).

Epidemiological reports of coccidia in worldwide
According to 55 studies included, have been related 46 references with reports of Cryptosporidium infection in HIV-infected and uninfected people. Equally, for C. cayetanensis were founded 28 studies with reports of prevalences in populations of the World and C. belli have been related around 32 studies which have determinate populations infected with coccidian. These studies were done with reports of Cryptosporidium in 29 countries, C. cayetanensis in 25 countries and C. belli around 19 countries (Fig. 2), including a distribution patron in countries of Europe, North America, sub-Saharan Africa, Latin America and the Caribbean and Asia. Evidencing a generalization de this type of microorganism typically in Tropical regions which may be related with its development and few sanitary conditions. However, the increase of these species is continuous, with high values of cases reports of infections, that have conditioned with major force clinical manifestation and management of new diagnostic techniques, have generated most investigations with respect the frequency of coccidia at level worldwide, where have been observed reports of infection in population that may be important your countries as in urban and rural areas. However, the infection by coccidian are widely distributed in the world, observe rates of prevalence with much variations that may be associated to immunocompromised and immunocompetent patients able of increased prevalence´s rates.

In the Table 1, are shown some studies of prevalence of coccidian in the world, indicating prevalence percent, and population affected with diagnostic techniques frequently employed.
Table 1 Prevalence of Cryptosporidium spp., Cyclospora cayetanensis and Cystoisospora belli in communities from different countries.
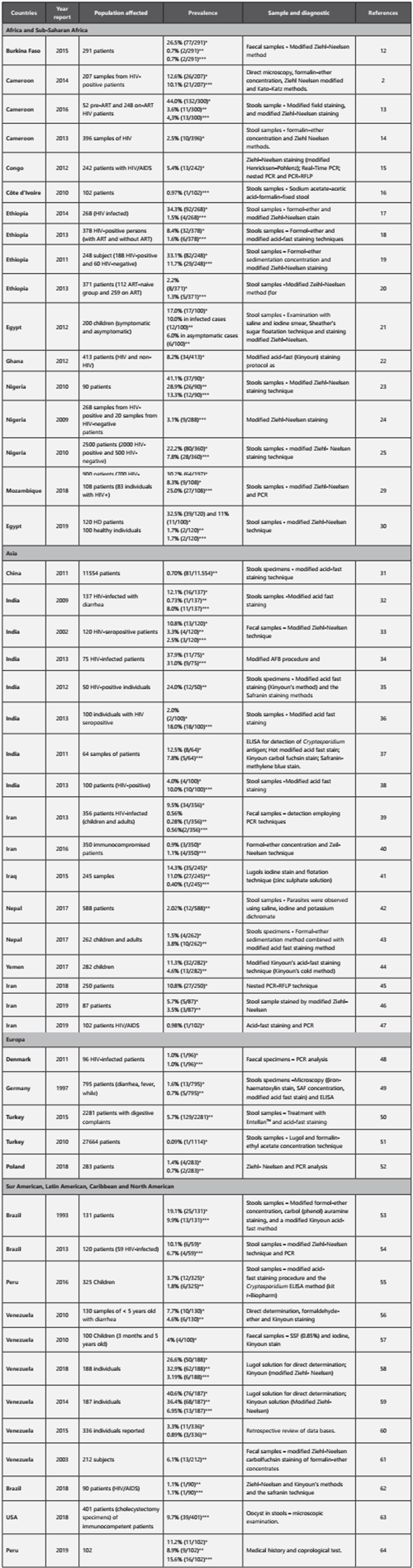
*Cryptosporidium spp. **Cyclospora cayetanensis. ***Cystoisospora belli. qPCR: Quantitative Polymerase Chain Reaction. ELISA: Enzyme-Linked ImmunoSorbent Assay. RFLP: Restriction Fragment Length Polymorphism.
In this review, are showed a variability in the reports of prevalence’s of Cryptosporidium infection that may be established in range between 0.09 - 44% associated with patients HIV/AIDS, coincident with registered in areas as Africa and sub-Saharan Africa (2.2 - 44%); Asia (1.5 - 37.9%); Europe (0.09 -5.7%) and in Latin America and the Caribbean with North America (3.3 - 40.6%). In the case of C. cayetanensis is observed a general prevalence between 0.7 - 36.9% with high relationship in patients with HIV/AIDS. Alike, in populations as Africa and sub-Saharan Africa is frequently found high prevalence´s (0.7 - 28.9%); Asia (0.7 - 24%); Europe (0.7 - 5.7%) and elevated prevalences data in Latin America and the Caribbean similar to evidence in Africa (1.8 - 36.9%). Also, C. belli shown values of prevalences into 0.4 - 31% observed at HIV-infected patients, which is evidenced similarly in communities of Africa and sub-Saharan Africa (0.7 - 13.3%); Asia (0.4 - 31.0%); Europe (1.0%) and in Latin America and the Caribbean with North America (3.2 - 9.9%).
In general, epidemiologic studies have been registered prevalence’s of Cryptosporidium spp., Cyclospora cayetanensis and Cystoisospora belli in European countries as UK (15.2%), France (0.2-23.0%), Italy (0.6-33.3%), Poland (5.4%), Portugal (7.7%), Turkey (0,5-6%)65-68. In Africa have established countries such as Cameroon (2.1-44.0%), DR Congo (2.9-31.0%), Ethiopia (1.3-34.0%), Kenya (8.8-25.9%), Ghana (28.6%), Nigeria (1.0-79.0%), Senegal (13.9-16.0%), South Africa (7.7-75.6%), Uganda (0.1-74%), Zambia (2.2-7.7%) and Zimbabwe (0-10%)69. Equally, in Asiatic continent exist a high prevalence in countries as China (12.0%), India (1.1-31.3%), Iran (0.6-9.6%), Saudi Arabia (4.2-19.2%), Libya (0.9-13.0%), Malaysia (3.0-23.0%), Nepal (0.2%-11.2%), South Korea (7.5-10.4%), Thailand (1.1-25.3%)65,70,71. In Latin-American, have been founded prevalence´s with similar frequency, including Cuba (1.5-12%), Colombia (2.6-29%), Guatemala (0.9-13.7%), Honduras (2.0-6.8%), Mexico (9.8-28.4%), Argentina (1.3%), Peru (0.7-52%), USA (0.8-33%) and Venezuela (0.2-41.6%)72. (Figure 2).
In wide evidences have established the association and coexistence of opportunistic intestinal parasites and increase the worldwide prevalence in HIV individuals, being Cryptosporidium, C. cayetanensis and C. belli, the main intestinal organisms detected with high relevance in HIV-infected patients; have been considered prevalences usually high in areas as sub-Saharan Africa, Asia and Latin American and Caribbean which have observed the intensification of numerous clinical signs in patients with diarrhea as principal manifestation in this type of patients. Possibly, the behavior in immunocompromised and immunocompetent lead to a substantial development of coccidia and largeness clinical indications, given the ineffectiveness of the immune response and poor results with pharmacological treatments, alike, these comportments are favored by the existence of conditions environmental in these populations, poor access to sanitary care and educational factors, that directly influence the exacerbation of the clinical alterations presented. For other hand, in ours review the studies included were predominated in Africa and subSaharan African (n=18), Asia (n=14) and Latin American and the Caribbean (n=10) and with few studies development in Europe (n=4), emphasizing the need for more robust investigation of Cryptosporidium spp., C. cayetanensis and C. belli infection in HIV-infected individuals in these areas. Likewise, many studies were identified through literature search, but not all results were available, additionally, the major part of studies registered were based traditional microscopic techniques that present a minor detection response compared with PCR, ELISA and fluorescent techniques, inducing to minor quantitation of coccidian or no corrected estimation of prevalences.
Epidemiological reports of coccidia in Colombia
In Colombia, some epidemiological data have been shown regarding the identification of intestinal coccidia and associated with multiple clinical manifestations. Likewise, different routes of exposure related to the invasion in different hosts. Some of these routes have been described from the conditions of health, food, consumption of contaminated water, soil and air with spores or oocysts, seasonal distribution, agricultural and livestock practices. Thus, in the limited reports established for the diagnosis of these parasites, some genera of intestinal coccidia have been detected such as Cryptosporidium spp, Cyclosporas spp., Cystoisospora spp. and Microsporidium spp. The few studies reported with respect to presence of coccidian in Colombia are listed in the Table 2.
Table 2 Prevalence of Cryptosporidium spp., Cyclospora cayetanensis and Cystoisospora belli in communities from Colombia.
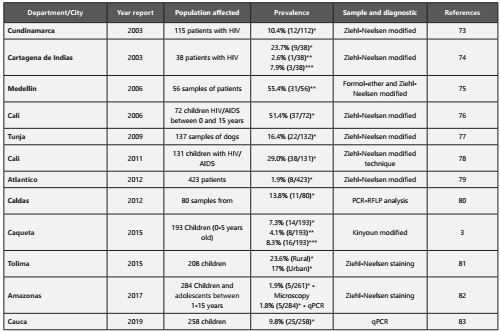
In the context Colombian, some the reports established by the Ministry of Health between the periods of 2012 to 2014, the diagnosis of the presence of intestinal coccidia in low proportion was demonstrated, values established on average between 0.5%, and individual records in some regions such as the Caribbean ocean territories in values close to 3.9%, and at the Pericaribeño, Norandina, Chocó-Magdalena and Amazonia Belt levels close to the value established at the national level; on the other hand, some historical studies of cryptosporidiosis in Colombia have shown prevalences between 2.5 and 4.0% in people with characteristic clinical manifestations such as diarrhea; However, this report can be higher in immunosuppressed individuals, among which 32 and 42% prevalence can be reached57. Likewise, other researchers establish the same scenario regarding the predominance of Cryptosporidium spp. with totally coincident values between 1 and 45.3% of case reports. Aspect that is not fully detailed for other types of coccidia such as Cyclosporas cayetanensis including C. belli which have shown some reports, but without a total distribution of prevalence84. Figure 3

However, the prevalence of the disease associated with Cryptosporidium from animal species is not fully clarified and the zoonotic association in Colombia is still lacking information. The few reports have shown the presence of Cryptosporidium around 16.4% of positive samples, where it was observed more frequently in children under one year of age, diarrea (OR = 2.99; p = 0.01) and the antecedent of a low vaccination effect. related to the probability of infection, which suggests that it can be an indicator or predictor of infection77. In this way, some similar reports have been established in the coffee region and specifically in the municipality of Caldas where fecal samples of cattle were analyzed by PCR-RFLP techniques, in which the confirmation of around 13.5% was demonstrated of presence of these parasites, being C. parvum the species completely identified in all the simples85. The authors have indicated that the presence of C. parvum in bovines represents a risk for individuals who perform tasks associated with these animals, possibly through direct routes such as contact with fecal matter in crop or grazing areas, or indirectly through the routes of contamination of drinking water by the presence of oocysts generated from the practices previously established80.
Likewise, in cross-sectional studies descriptive type, the department of Atlántico allowed the identification of the presence of oocysts of Cryptosporidium spp. by microscopic and macroscopic analysis in fecal samples. Evidence of similar prevalence values at the national level, these prevalence values of 1.9%, further demonstrated the association between the presence of the parasitic agent and symptoms such as fever, the presence of blood in the samples and the incidence of zoonotic elements (domestic animals). In order to provide detailed information regarding the clinical manifestations due to this type of coccidian79. Additionally, this similar behavior is evidenced in other increasingly rural populations such as Amazonas (Puerto Nariño, San Juan del Soco, Villa Andrea and Nuevo Paraíso), where the presence of intestinal coccidia such as Cryptosporidium sp. was established in these communities. Which were diagnosed in faecal samples in minors by using microscopy techniques, showed prevalences greater than 1.8%, managing to identify 3 species of Cryptosporidium including C. viatorum, C. hominis and C. parvum, establishing that these species are linked in the transmission in humans and keeping a close relationship with the living conditions of these populations82.
On the other hand, it is very common to find a high association and presence of this type of coccidias in immunocompetent and immunosuppressed individuals, as is the case of patients with HIV, in which they have been associated with Cryptosporidium and other coccidia as opportunistic parasites. In studies developed by Flórez et al, the prevalence of Microsporidium and other opportunistic intestinal parasites in HIV-infected patients with gastrointestinal symptoms was studied, for which 115 patients were studied during 2001, in different health institutions and in which the Sample of fecal matter of each individual. In this way, it was established that the prevalence of opportunists was 10.4% for Cryptosporidium spp. Regarding Microsporidium spp, a figure of around 29% was found through modified screening68,86. Likewise, Botero et al, determined the presence of intestinal parasites such as Cryptosporidium spp., Microsporidium spp, C. cayetanensis and C. belli, in which prevalences of 3.6% and 1.8% were indicated for Cryptosporidium spp., Microsporidium spp., respectively. For another hand, Siuffi et al. have identified the presence of coccidia in feces of infants with AIDS through colorimetric tests and detection of viral load accompanied by an increase in TCD4 lymphocyte values. The prevalence was close to 51.4%, with the population mostly affected between the ages of 5-10 years and related to the most advanced cases of AIDS 76. Similarly, some reports have established the prevalence in 29% of children in the department of Valle del Cauca, in addition to the detection of a high percentage of presence, some manifestations and aspects were related as abdominal pain, the presence of animals and a considerable viral load. Likewise, a behavior of higher incidence of infection by Cryptosporidium was observed in terms of its geographical distribution at the level of rural areas or with clinical recidivism68.
However, for Cyclospora cayetanensis and Cystoisospora belli no evidence of parasite oocysts was found87. However, have been evidenced minor reports of prevalence of Cyclospora cayetanensis as study development by Botero-Garcés et al., in number of cases of diarrhoea appeared in 2002, obtained of 56 samples of stool from patient found as etiological agent to Cyclospora cayetanensis with positive response. Which, 55.4% of the patients evaluated proved positive for C. cayetanensis75. Equally, in a study realized by Lucero-Garzón et al in Caquetá, Colombia, which fecal samples were collected from 193 children and coccidia were identified using the Kinyoun technique with modifications, demonstrating that the prevalence of coccidia was 19%; with prevalence’s individually for Cryptosporidium spp. (7%), Cystoisospora spp. (8%) and Cyclospora spp. (4%)3.
Discussion
During years the epidemiological studies of coccidia in the world increases progressively due to sanitary conditions and factors that encourage the transmission and propagation from one vector to another. The large cases reported worldwide, especially in countries in Africa, Asia and America, have been associated with a high alteration in health care conditions, inadequate implementation of public policies and cultural patterns, in which have been evidenced high rates prevalence and particularly in cases of immunosuppression related to patients with HIV/AIDS.
Likewise, the propagation of these agents in these regions has been schematized in different routes, but definitely maintain common patterns of infection independent of the region. Thus, in the transmission and invasion of the host, the oocysts of Cryptosporidium spp., C. belli and C. cayetanensis can remain in the stool and eventually be transmitted to humans1; multiple routes of infection can be established depending of geographic reference, including areas of medium to high prevalence, such as in rural zone associated with wide agricultural activities, with low sanitary access and inadequate life habits58,88, in which the passage of feces of infected animals through direct manipulation by the individuals of farm leads to an increase in the likelihood of invasion by the oocysts and finally could contaminate plants and fruits as possible route of contact with the organisms89,90, or indirectly by runoff waters or wastewater that may be serve as vehicles of parasitic forms, leading to contamination of plants91-93; likewise with contamination of water deposits that can be used as water sources of supply for human consumption or animal husbandry94-96. However, atypical infections of nonendemic individuals may be affected due to the consumption of contaminated food or water ingested by the mechanisms established above97. Figure 4.

Correspondingly, multiple methods of diagnosis of coccidia were established in the global and national prevalence reports, in which traditional and modern methods for the identification of these agents have been established. The use of each of these methods depends the objectives, sensitivity, precision and accuracy in the characterization of each species, as well as the dependence on the operational cost of equipment and materials to diagnosis. Likewise, in traditional microscopy methods for the correct detection of intestinal coccidia, it is advisable to process a coprological examination using a stool concentration technique and thus increase the chances of finding oocysts, it´s also required to apply the modified Ziehl Neelsen staining, for their visualization, taking into account that coccidia are acid resistant alcohol. At present, in less developed countries such as Colombia, these methodologies are still tools of wide application due to several advantages such as rapid screening, low cost, and to which research institutions and clinics have Access98,99. However, these techniques have some disadvantages in terms of handling, the development of poorly validated and non-reproducible techniques that lead to the inaccurate detection of some species of coccidia100.
Also, other methods applicable in the identification of intestinal coccidia, specified the ability of self-fluorescence that has the genus Cyclospora, fluorescence microscopy is a very sensitive and specific method of support for its diagnosis within which the auramine O101, and other diagnostic methodologies such as Enzyme immune-assays (EIAs) or immunochromatographic lateral flow (ICLF) and automated capillary electrophoresis (CE)-based DNA fragment analysis tool102-104. Additionally, the use of DNA extracted from coccidia oocysts for PCR amplification is very useful for an accurate diagnosis. At present, PCR techniques can represent advantages around the time of analysis, improvement of sensitivity and reduction of cross contamination, resulting in a greater response capacity and accuracy105. However, some methodological limitations appear to be related to the stool samples of the organisms analyzed, in which agents capable of inhibiting polymerase activity, necessary for the DNA amplification process of these agents may be present106,107. On the other hand, in Colombia due to the barely growing research development, and taking into account the high economic costs for the implementation of these techniques, few institutions have carried out this type of strategies in order to establish an accurate opinion and complete validation of the complete epidemiological panorama of the country.
On the other hand, the relationship of the presence of diseases with a growing background such as HIV/AIDS, which affects disadvantaged populations and even countries with high economic incomes, has been established. The global reports established by the WHO register that more than 30 million individuals are related to HIV/AIDS108, supporting a death rate of more than 900,000 people109. Also, in consideration of the increases in the prevalence, the parasitic agents such as coccidia show a sustained increase at the level of the whole world, in which show a substantial relationship in immunocompetent and immunocompromised individuals110. According to the epidemiological reports it has been estimated that individuals with HIV/AIDS tend to increase the prevalence levels of coccidia. In this way, populations that reach reports of infection between 3.1 - 44% in the African continent have been characterized14,111; likewise, in Asia with values between 0.98 - 37.9%112,113 and similar estimates are established in the American continent, with records between 1.1 - 40%68. In addition, in Colombia the presence of coccidia has a behavior similar to that established by the world reports, despite establishing the registry of few studies at the national level. These general data indicate a behavior trend that can affect approximately half of the individuals detected with HIV/AIDS, due to the opportunism of these microorganisms, which spread rapidly and lodge at the intestinal level, during the infection by coccidias multiples mechanism are active inducing internalization into enterocyte, modifying cellular structure by exportation and activation of cytokines pro-inflammatory that increase phagocytic capacity114. Therefore, these activated cells release mediators such as prostaglandins, neurotransmitters, leukotriene’s that influence the secretion of chloride and water ions, as well as the negative regulation of intestinal absorption103, and finally have a direct impact on the deterioration of the cell epithelium, established by an apoptotic effect induced by the parasite due to its growth and generation of new infectious agents, as well as damage of microvilli and cryptic hyperplasia115. Alike, in the patients a series of clinical complications occur, where about 90% of the patients diagnosed manifest each of these physiological alterations116. Moreover, the clinical symptomatology related between HIV/AIDS and the presence of coccidia in patients is denoted by the development of diarrheal stools as an indicator of increased complications of the alteration in patients39,108, with repercussions on their nutritional status and body homeostasis. Similarly, scientific literature has associated the development of acute or chronic diarrheal syndromes that reflect a marked loss of body mass, electrolyte imbalance, abdominal pain and alterations in the absorption of nutrients117,118 often established in immunocompromised patients. On the other hand, chronic diarrhea can lead to increased morbidity and mortality in these patients. In this way, the presence of these enteroparasitosis increases the mortality probabilities of immunocompromised patients or could cause refractory infections118.
Conversely, intestinal coccidia are infectious agents of great importance in public health, due to the impact generated and the increasing detection cases in the world population and national level. The presence of coccidia induces direct effects in the countries of low and medium development, with consequences especially in the health and well-being, due to the lack or ineffectiveness of the health systems, low development of the sanitary conditions and a notable decrease to the access to education119. Additionally, based at the aspects of public health, few studies as the Parasitism Survey 2012-2014 has been notified, considered as a repository that collects the behavior of different parasitic agents including coccidia, which have established conceptual aspects regarding it´s characteristics, a globalized distribution and prevalence at national level, in which 0.5% of Cryptosporidium sp. Were detected throughout the national territory, and almost distributed to other agents120. However, can be variable due to the health conditions of the patients, in which it has been observed in immunosuppressed individuals, who manage a tendency to increase these prevalence rates5. Considerations that have been reflected in the cases studies about of the presence of coccidia at the national level, which demonstrates a high rate of affection and a notable intensification of clinical manifestations (Table 2).
Thus, in order to maintain a basis of balance, prevention of cases and optimal living conditions, the implementation of public policies has been generated as considerable tool for the reduction of the effect generated. In the national territory there are limited declarations of public policies associated with the control of these agents. However, according to the guidelines established by the WHO, PAHO, the Ministry of Health and Social Protection of Colombia have been contemplated in the Health Plan 2012-2021, the interventions for the search for the reduction of inequity in health, establishes policies and programs based on 8 dimensions, as indicated in the dimension of healthy living and communicable diseases, which incorporate a set of regulations and actions that allow the right to live free of communicable diseases to be realized through strategies, where the emergent, reemerging and neglected diseases121, which is related to infectious processes caused by intestinal coccidia.
Similarly, in public health the environmental factor plays an important role for the maintenance of the well-being of the population and its environment, So, some comprehensive regulations have been included in the regulation of microbiological quality and, including the detection of these agents in consumer elements such as the one developed in the Conpes 113 of 2008 regulation122, which have been related to the presence of coccidia such as Cryptosporidium spp., which have a negative impact due to their ability to contaminate water sources and as a consequence generate intestinal diseases95,96. Likewise, the Ministry of Social Protection through Decree 1575 of 2007, establishes the implementation of prevention and control measures for drinking water sources for the purpose of monitoring microbiological risks123, due to the impact of intestinal coccidia in the generation of diseases transported by these routes, and in addition to this, the development of operational strategies through the use of information systems that allow estimates and monitoring of affected populations. In addition, other regulations, such as resolution 2115 of 2007, have established the identification of invasive forms as Cryptosporidium oocysts, aspects that have been validated by the National Health Institute with the aim of implementing analysis methodologies124.
Finally, these regulations should be implemented with greater operational direction in the prevention and promotion of the health conditions of the populations, and inclusive from the perspective of study of all the coccidia triggering intestinal parasitosis. This behavior will allow for greater consolidation of public health programs, the development of updated databases and the dynamism in the execution of action plans to reduce epidemiological indices.
Future perspectives and upcoming directions
This paper reviews show the evidences of generalities and the importance of a knowledge of the epidemiology of human of pathologies associated to coccidian, focusing in developing multiples populations and specially in Colombia. In this way, not exist complete studies in relation to the reports of the presence of intestinal pathogenic coccidia in each of the regions of the country, and knowing the succession of associated factors such as sanitation, adequate knowledge of crops and methods optimized breeding of livestock, sustainable social development and education, it seems to indicate that currently it is necessary to perform a new knowledge and verification of records due to the continuous increase in clinical cases that could be associated with this problem. Thus, is necessary the compression of punctual dates that are essential understanding the surveillance and risk factors for the infection, in order to supports risk management, control and prevention of cases and evasion of elements of transmission.

