











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The Kangaroo Mother Care (KMC) is an alternative to reduce stress for hospitalized babies and their mothers 1. However, several challenges can cause stress for mothers, such as fear of injuring their baby, difficulty maintaining the kangaroo position, fatigue, gender role concerns, limited opportunities for parents to practice the method 2, and lack of family support 3, negatively impacting maternal perceptions of their ability to care for their baby at home and affecting the quality of mother-child interaction.
Barnard's theory emphasizes that successful mother-child interaction relies on the ability of both to adapt to each other, with the quality of the socio-emotional environment in early childhood largely dependent on maternal competence in establishing an emotionally supportive and harmonious setting 4. The woman who can effectively meet her child's needs is considered a competent mother 5. However, preterm babies often provide limited responses to their mothers, and if the mother lacks sufficient understanding of her child's behavior, this dynamic can disrupt their interaction, leading her to perceive herself as incapable of alleviating her baby's discomfort 4.
The mother's ability to alleviate the baby's feelings of discomfort is one of the characteristics of mothers that Barnard argued for in her theory 4. Consequently, mothers who respond to and meet their children's needs gain confidence and competence, generating a positive interactive experience 4. However, when a premature baby does not send clear signals or is developmentally unresponsive 6, it can undermine the mother's ability to perform her parenting role safely and effectively, meaning the mother's confidence, competency, and satisfaction 7.
Low self-efficacy affects mothers' responses when they interact with their children 8, making it necessary to pay attention both to the mother's and the newborn's emotions 9. The perception of self-efficacy refers to an individual's judgment about their own abilities to perform tasks and handle situations with an expectation of success. It is not an inherent quality, but rather how one perceives their capacity to manage specific situations 10, understood as a dynamic and emergent attribute, subject to change depending on the demands of a particular task or situation. In this context, being a competent mother involves the ability to effectively respond to her children's needs. It requires a harmonious approach to foster an interaction that is productive and satisfying for both mother and child within a nurturing environment 5.
Therefore, if the environment for premature infants is made pleasant-resembling the safety and comfort of the womb-and mothers are actively involved in the development of care interventions, it can significantly improve the child's neurobehavioral outcomes in the long term. This serves as a motivating factor for mothers 11, especially when interventions are conducted in natural settings like the home. A scoping review concluded that infant massage administered by mothers to their hospitalized premature babies decreased their stress, improving maternal-infant interaction, satisfaction, and maternal competence in the short term 12.
Several interventions aim to foster early interactions between parents and premature infants, including auditory, tactile, vestibular, and visual (ATVV) massage therapy 13. While this technique has been evaluated with hospitalized infants, its application at home for babies in the kangaroo position has not been explored extensively, which means maintaining the kangaroo position during such interventions without disruption, and in the case of Bogota, with an average temperature of around 13-14°C. Furthermore, some mothers with premature babies at home are hesitant to perform massages due to a lack of knowledge and express a need for guidance from nurses on suitable techniques for the home environment 14.
Educating mothers about stimulation techniques is an essential step toward enhancing person- and family-centered care 15, considering that interventions targeting premature and low birth weight newborns can have profound future impacts on child health 16. Moreover, employing multimodal nursing intervention strategies, supported by valid and reliable scales like the perceived maternal parental self-efficacy questionnaire adapted to the Colombian context, significantly benefits both maternal and child health 17.
Nursing is vital for effective KMC management 18 and its professionals become key guides for its implementation 19. The practice itself helps overcome fear and reinforces positive experiences 20 while encouraging self-care for mothers and their families. Most massage techniques in premature newborns were performed in incubators and neonatal units, evidencing an absence of studies that apply a massage technique for premature babies in the kangaroo position at home, under the care of their mothers and families 15,21,22.
Nevertheless, the KBM technique is an intervention that has been used by mothers since 1996, allowing them to care for their premature infants without the need for an incubator, both in neonatal units and home settings. A 2021 pre-experimental study involving 63 premature newborns from an outpatient kangaroo program in Bogota, Colombia, highlighted the safety of KBM on physiological parameters, demonstrating positive effects on heart rate, oxygen saturation, and temperature 23, although the study did not explore its impact on perceived maternal self-efficacy.
The objective of the present study was to investigate the effect of the KBM on a mother's ability to alleviate her child's discomfort, measured through perceived maternal self-efficacy, grounded in the hypothesis that KBM, when applied by mothers, would positively influence their perceived ability to effectively comfort and care for their infants, thereby enhancing maternal self-efficacy.
Methodology
This quantitative study employed a pragmatic randomized clinical trial design, evaluated using the PRECIS-2 tool. It was a parallel, double-blind trial involving two groups: An experimental group with mothers applying the KBM technique to their children, and a control group with mothers carrying their children in a kangaroo position without massage.
Mother-kangaroo baby pairs were randomly assigned to either group to prevent measurement bias. A biostatistician used computer-generated sequences through Stata to create a simple randomization scheme in blocks of size four. This resulted in 34 pairs in the KBM intervention group and 34 pairs in the kangaroo position control group without massage. To ensure blinding, sealed dark envelopes marked with codes from 1 to 68 were used, each corresponding to a consecutive assignment number. Inside each envelope was a slip indicating group assignment: A red slip for the KBM group or a blue slip for the control group. Additionally, the envelope contained information about the nurse responsible for conducting the tele-consultation. The opening of the envelopes was witnessed by the mother and an independent observer to maintain transparency.
Recruitment considered inclusion and exclusion criteria that allowed selection biases to be controlled. The inclusion criteria took into account that the baby was less than 37 weeks of gestational age or with low birth weight, cared for by its mother in the kangaroo position at home, with a gestational age greater than or equal to 30 weeks, age-corrected equal to or greater than 35 weeks at the time of recruitment, weight equal to or greater than 2100 g at the time of entry into the study, and controls in the Outpatient Kangaroo Mother Program of the Centro Policlinico del Olaya. Mothers with at least two days of training in said program, with social support, a family member's phone number, WhatsApp, and email.
Babies with a history of grade III or IV intraventricular hemorrhages, congenital malformations, or conditions requiring hospitalization during the study were excluded, as well as mothers who were hospitalized at the time of recruitment, re-hospitalized during the study, had cognitive problems or mental disorders, or had live twins.
The sample consisted of 34 mother-kangaroo baby pairs in each group, with a confidence level of 95 % and a significance level of 5 %. An estimated 10 % loss was accounted for. The independent variable was the KBM intervention, while the dependent variable was the total score of the perceived maternal self-efficacy questionnaire, which has robust psychometric properties for use with parents of neonatal populations. Initially validated with mothers of hospitalized premature newborns, the questionnaire has been proven to be a reliable, robust, and valid psychometric measure 25. It has also been utilized in other studies during the postnatal period and with first-time mothers 26,27.
Vargas et al. 26 were the first to translate this instrument into Spanish to use it in practice, research and, especially, easily measure maternal self-efficacy not only during the hospital stay but also at discharge and during postpartum follow-ups. The study found that the questionnaire had high face validity for women, with a comprehension rate of (99 %). For experts, it showed medium comprehension (84.1 %), medium clarity (83.9%), and medium precision (80 %). The content validity index was robust, with relevance scores of 0.93 and 0.96. The overall Cronbach's alpha value was 0.98 (95 % CI: 0.97-0.98). Therefore, the Spanish version of the questionnaire, with its robust properties, is suitable for identifying women with low self-efficacy and evaluating the effectiveness of nursing interventions.
The questionnaire contains twenty items, each rated on a Likert scale from 1 to 4 (strongly disagree, disagree, agree, strongly agree), with a maximum total score of 80. In this study, mothers completed the questionnaire through self-report at three points in time: before starting the intervention, 7 days after implementation, and 14 days after implementation. Additionally, there was a daily report noting who assisted with the kangaroo care and the mother's perception of "I am good at kangarooing" until the baby no longer required the position. These data were recorded in a printed manual titled Diary of My Kangaroo Baby, which also contained the perceived maternal self-efficacy questionnaires for days 7 and 14. Mothers were instructed to fill out the questionnaires and send photographic records via WhatsApp to the respective nurse conducting the follow-up. This method helped control measurement and information biases.
The information was collected in three stages:
Training of research assistants: A professional nurse expert in the Kangaroo Mother Program was trained virtually, who would be in charge of the control group; a research assistant was also trained in the management and systematization of the data, and a third research assistant was also trained to verify the data in its entirety.
Recruitment of the mother-baby kangaroo pairs: It was done in person, after the outpatient kangaroo program control. Once the mother voluntarily agreed to participate in the study and signed the informed and substituted consent, the sheets on sociodemographic aspects and maternal and perinatal history were completed, and the perceived maternal self-efficacy questionnaire was applied. The mother was trained in taking temperature with the baby in the kangaroo position and all mothers were given a kangaroo kit (the Diary of My Kangaroo Baby and black ink pen, 500 ml liquid hand soap, cotton lycra kangaroo girdle, digital thermometer). Mothers assigned to the intervention group received the massage kit (a 100 ml bottle of sunflower oil and a soft styling brush).
Virtual Training and Home Implementation: The control group received training from a research assistant, who sent a connection link via WhatsApp. All mothers in this group were trained simultaneously at 8:00 p.m. through a nursing teleconsultation, which included a PDF presentation covering hand washing, correct use of face masks, kangaroo position, alarm signs, and management of the diary. Following the training, the mothers were instructed to take their baby's body temperature while in the kangaroo position, observe for ten minutes, take the temperature again, record it in the diary, and send a photo via WhatsApp. It is important to note that the control group did not receive any training related to massage and did not apply any type of massage. The nurse monitored the control group daily via WhatsApp until the baby no longer required the kangaroo position.
For the experimental group, the nurse sent mothers a connection link and an audiovisual guide titled "Kangaroo Baby Massage" via WhatsApp. Mothers were instructed to consult this guide and practice the KBM technique with a doll at home before the nursing teleconsultation. This audiovisual guide served as a step-by-step reference for mothers to apply the massage daily to their babies, available at https://youtu.be/NV6ZDjodkXw?si=bf2fByrX6q6iwADI 28.
The mother logged on at 8:00 p.m. from their home through their mobile phone or computer for the teleconsultation, a PDF presentation was used with the same topics as the control group; additionally, mothers in the intervention group received training on how to perform the KBM at home, they took the baby's temperature before and after giving the KBM, in a way that, while the researcher demonstrated through the screen the step by step of the application of the method on a simulator (doll), the mother was simultaneously performing it at home.
Mothers in both groups completed and reported the perceived maternal self-efficacy questionnaire at 7 and 14 days. The main researcher received the information after all the data were rigorously verified. Mother-child pairs were continuously followed and evaluated. The protocol included several safety measures, such as taking the temperature before and after the KBM intervention, and ensuring it was conducted in a secure room with closed windows and doors, without interrupting the kangaroo position. The mother always used the kangaroo girdle, with the baby remaining in position while the mother lay down with the head of the bed inclined at 30° to prevent the risk of falling. Additionally, all measures to minimize COVID-19 transmission were strictly followed, as synthesized in a literature review 29.
The study was classified as research with greater than minimal risk due to the therapeutic intervention; however, the KBM is a non-invasive technique. Permission to use the perceived maternal parenting self-efficacy questionnaire was obtained, along with ethics approval from the Universidad Nacional de Colombia and the Centro Policlinico del Olaya. The study was registered prior to the pilot test on the United States National Library of Medicine platform (clinicaltrials.gov) with the identifier NCT04908332 30.
Results
The intervention was implemented and evaluated from August to December 2021 in the Outpatient Kangaroo Mother Program at the Centro Policlinico del Olaya in Bogota. At the time, the program was not conducted as a collective consultation due to the need to expand intensive care for COVID-19 patients and implement isolation measures. Consequently, the program operated in two offices where only the mother and her baby were allowed entry, adhering to protocols for mask use, hand washing, and social distancing. Meetings between mothers and group educational activities were strictly prohibited, minimizing the risk of sample contamination.
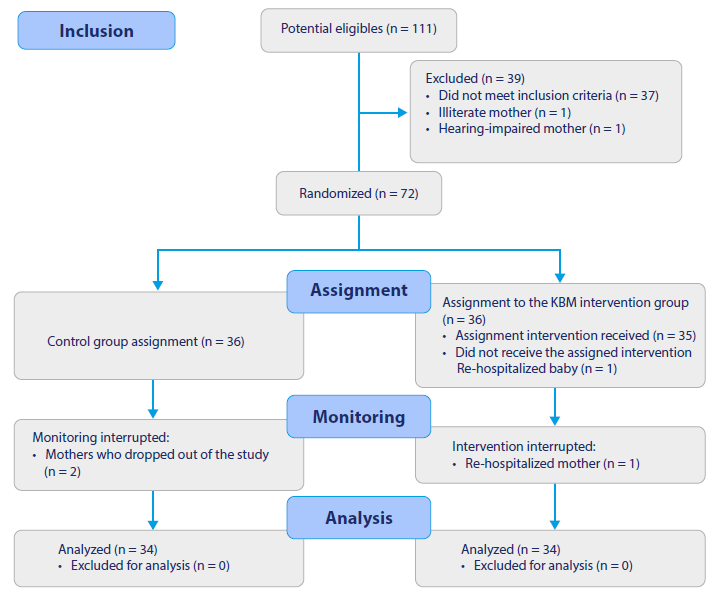
Figure 1 presents the flow chart according to the Consolidated Standards of Reporting Trials (CONSORT) 31, detailing the procedure for inclusion, assignment, monitoring, and analysis of the sample. The study was well-received and widely adhered to by participants.
The baseline data were homogeneous in the two groups (KBM vs. control), except for maternal age, finding that mothers in the KBM group were older (28 ± 6.4) than the mothers in the control group (24 .4 ± 5.1) (p=0.014). These data are presented in Tables 1, 2 and 3, corresponding to sociodemographic aspects, maternal history, and perinatal characteristics.
Table 1 Sociodemographic Aspects KBM vs. Control
Source: 32.
Table 2 Maternal History KBM vs. Control
Source: 32.
Table 4 presents the family support received by mothers in the KBM group, where a family member (typically the father or grandmother) took over kangarooing duties, allowing the mothers to rest. This support showed statistically significant differences over the days (p<0.05). In contrast, mothers in the control group generally performed kangaroo care alone. Table 5 shows that there were no statistically significant differences between the two groups (p>0.05) concerning the maternal perception expressed in the statement, "I am good at kangarooing my baby."
Table 3 Perinatal Characteristics KBM vs. Control
Note: F=Fisher; *Chi squared; U= Mann-Whitney: M (±SD) = Mean (± standard deviation); T= T student; NICU= Neonatal care unit.
Source: 32.
Table 4 Family Support to Carry the Baby in the Kangaroo Position KBM vs. Control
| Day | n | Group | Dad and Grandmother | Only the Mother | Other People | p |
|---|---|---|---|---|---|---|
| 1 | 3. 4 | Control | 1 | 11 | 22 | 0* |
| 3. 4 | KBM | 20 | 1 | 13 | ||
| 2 | 33 | Control | 1 | 9 | 23 | 0* |
| 33 | KBM | 18 | 1 | 13 | ||
| 3 | 3. 4 | Control | 4 | 7 | 23 | 0.01* |
| 33 | KBM | 16 | 3 | 14 | ||
| 4 | 3. 4 | Control | 1 | 9 | 24 | 0.001* |
| 31 | KBM | 15 | 2 | 14 | ||
| 5 | 30 | Control | 0 | 7 | 23 | 0* |
| 30 | KBM | 15 | 4 | 11 | ||
| 6 | 31 | Control | 2 | 8 | 21 | 0.01F |
| 28 | KBM | 14 | 3 | 11 | ||
| 7 | 28 | Control | 2 | 7 | 19 | 0.001F |
| 24 | KBM | 14 | 3 | 7 | ||
| 8 | 26 | Control | 2 | 7 | 17 | 0.024F |
| 20 | KBM | 9 | 3 | 8 | ||
| 9 | 19 | Control | 1 | 6 | 12 | 0.002F |
| 18 | KBM | 11 | 2 | 5 | ||
| 10 | 16 | Control | 1 | 5 | 10 | 0.033F |
| 15 | KBM | 7 | 1 | 7 |
F = Fisher; * Chi squared; KBM= Kangaroo Baby Massage; Significance 0.05
Source: 32.
Table 5 Maternal Perception: "I am good at kangarooing." KBM vs. Control
| Day | n | Group | Disagree | Agree | Strongly Agree | p |
|---|---|---|---|---|---|---|
| 1 | 3. 4 | Control | 14 | 20 | 1* | |
| 3. 4 | KBM | 14 | 20 | |||
| 2 | 33 | Control | 17 | 16 | 0.215* | |
| 33 | KBM | 12 | 21 | |||
| 3 | 3. 4 | Control | 17 | 17 | 0.056* | |
| 33 | KBM | 9 | 24 | |||
| 4 | 3. 4 | Control | 15 | 19 | 0.206F | |
| 31 | KBM | 9 | 22 | |||
| 5 | 30 | Control | 11 | 19 | 0.584F | |
| 30 | KBM | 9 | 21 | |||
| 6 | 31 | Control | 13 | 18 | 0.283F | |
| 28 | KBM | 8 | 20 | |||
| 7 | 28 | Control | 12 | 16 | 0.115F | |
| 24 | KBM | 1 | 8 | 15 | ||
| 8 | 26 | Control | 8 | 18 | 0.187F | |
| twenty | KBM | 3 | 17 | |||
| 9 | 19 | Control | 7 | 12 | 0.162F | |
| 18 | KBM | 3 | 15 | |||
| 10 | 16 | Control | 5 | 11 | 0.256F | |
| fifteen | KBM | 1 | 2 | 12 |
Note: *Chi = square; F = Fisher; KBM= Kangaroo Baby Massage (intervention): Significance 0.05 Source: 32.
The mother's ability to alleviate the baby's discomfort was assessed using the total score from the perceived maternal self-efficacy questionnaire, which was administered to 68 mothers with kangaroo babies. These mothers were divided into the intervention (KBM) and control groups, and the questionnaire was applied at three different points in time (days 0, 7, and 14). Table 6 indicates that, although mothers in the KBM group started with a lower score-median (Q1; Q3) = 68.5 (56; 80)-compared to mothers in the control group [71.5 (48; 79)], by day 14, the score for the KBM group increased considerably to 77.5 (66; 80), compared to 75 (61; 80) for the control group. Consequently, the final measurement of the questionnaire revealed a significant difference between the groups, with higher scores for the mothers who applied the KBM technique at home.
Table 6 Total Perceived Maternal Self-Efficacy score KBM vs. Control
| Time | Group | n | Minimum | Maximum | Median | Q1 | Q3 | IQR | Half | D.S. |
|---|---|---|---|---|---|---|---|---|---|---|
| Day 0 | KBM | 3. 4 | 56 | 80 | 68.5 | 64.25 | 72.75 | 8.5 | 68.176 | 5.697 |
| Day 07 | KBM | 3. 4 | 60 | 80 | 72.5 | 70 | 77 | 7 | 72.382 | 5.919 |
| Day 14 | KBM | 3. 4 | 66 | 80 | 77.5 | 75.25 | 80 | 4.75 | 76.735 | 3,752 |
| Day 0 | Control | 3. 4 | 48 | 79 | 71.5 | 64.25 | 75 | 10.75 | 69.324 | 8.112 |
| Day 07 | Control | 3. 4 | 55 | 80 | 72.5 | 68.25 | 78 | 9.75 | 72.324 | 6.153 |
| Day 14 | Control | 3. 4 | 61 | 80 | 75 | 68.25 | 79 | 10.75 | 73.5 | 6,121 |
Source: 32.
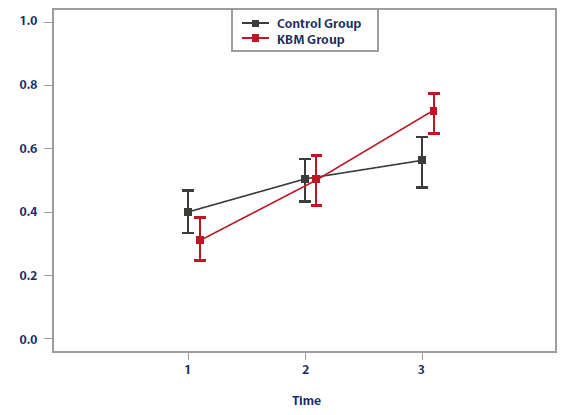
After running the F1LDF1 statistical model, Table 7 clearly shows that the relative treatment effects (RTE), with the respective 95 % confidence intervals, indicate a higher total score observed in the questionnaire. This change occurred significantly faster in the intervention group.
Table 7 RTE: Perceived Maternal Self-Efficacy in Time-Group Relationship KBM vs. Control)
| Group | Time | n | Mean of the ranges | RTE | Bias | Variance | Lower limit | Upper limit |
|---|---|---|---|---|---|---|---|---|
| KBM | 1(day 0) | 34 | 64.029 | 0.311 | -0.0005 | 0.083 | 0.250 | 0.386 |
| KBM | 2(day 07) | 34 | 103.177 | 0.503 | -0.0001 | 0.109 | 0.426 | 0.581 |
| KBM | 3(day 14) | 34 | 147.279 | 0.719 | 0.0007 | 0.071 | 0.650 | 0.776 |
| Control | 1 (day 0) | 34 | 82.118 | 0.400 | -0.0007 | 0.088 | 0.333 | 0.473 |
| Control | 2(day 07) | 34 | 102.941 | 0.502 | -0.0002 | 0.076 | 0.437 | 0.567 |
| Control | 3 (day 14) | 34 | 115.456 | 0.564 | 0.0009 | 0.114 | 0.482 | 0.640 |
Source: 32.
Figure 2 shows the significant difference between groups, displaying better results in the total score of the mothers who applied the KBM at time 3 (day 14).
In summary, the KBM technique applied by mothers had a favorable effect on the ability to alleviate the newborn's feeling of discomfort, expressed in perceived maternal parenting self-efficacy.
Discussion
This study's findings show sufficient statistical evidence of the positive effect of the KBM on perceived maternal self-efficacy in mothers who applied the method compared to the control group of mothers who only kangarooed, with differences also found over time. The results were given in RTE (lower limit; upper limit), in the three measurements (days 0, 7 and 14), both for the KBM group [day 0: 0.311 (0.250; 0.386), day 7: 0.503 (0.426; 0.581), day 14: 0.719 (0.650; 0.776)], as well as for the control group [day 0: 0.400 (0.333; 0.473), day 7: 0.502 (0.437; 0.567), day 14: 0.564 (0.482; 0.640)].
Prematurity, compared to a full-term birth, generally had no effect on the perception of maternal self-efficacy 33. This finding supported the use of the self-efficacy questionnaire with mothers of premature newborns at home as well as allowing testing the positive effect of the KBM on maternal self-efficacy compared to the control group over time. The results of this study showed statistically significant differences between the two groups (KBM vs. control), with higher total scores at day 14 [mean (± SD): KBM = 76.7 (± 3.7) vs. control = 73.5 (± 6)], in alignment with the findings of Tristão 33, who reported no significant differences in mean total scores (± SD) between mothers of premature babies [65 (± 9)] and mothers of full-term babies [65.5 (± 8.2)]. Similarly, Vargas reported no significant differences in mean total scores (± SD) between first-time mothers of full-term babies receiving the multimodal intervention Maternal support in the process of becoming a first-time mother = 70.03 (± 7.08) and those receiving usual postnatal care = 69.73 (± 7.75); p=0.87. In a similar fashion, Taneja 34 found no significant effect on maternal competence scores at 6 weeks and 12 months after promoting skin-to-skin contact and breastfeeding through home visits (intervention group) compared to the control group. A recent study highlighted low perceived maternal self-efficacy in adolescent mothers due to the birth of a premature child, particularly when hospitalization was required 35.
This research is notable for being the first to evaluate mothers' perceptions of being "good at kangarooing," finding that the KBM intervention did not alter this perception at any point in time (Table 5). Perceived maternal self-efficacy and family support uniquely explained variations in parenting stress during the postpartum period, compounded by the challenges of the COVID-19 pandemic 36. The findings of this study, along with others 36,37, indicate that the severe restrictions of the pandemic, which forced families to stay at home, made cohabitation with a partner beneficial for alleviating parenting stress.
Empowerment is crucial for competence in caregiving and facilitates the transition to home life, allowing parents to recognize their abilities and believe in themselves 38. Consequently, mothers who applied KBM felt more competent and perceived themselves as more empowered in caring for their children.
The study by Torres et al. found that 57.6 % of mothers with partner support reported high self-efficacy in breastfeeding 39. Similarly, in our study, mothers who applied the KBM technique received more help from their partners, who also undertook nursing duties, allowing the mothers to rest. As recommended by Rebolledo 8, it is crucial to address maternal tiredness or fatigue and implement interventions like KBM to enhance maternal well-being and mental health.
Additionally, in line with Kourouma et al. 3, who suggested designing strategies and interventions to improve the acceptance of KMC, our findings with the application of the KBM technique of fer an alternative solution to minimize barriers related to gender-related fatigue 40, lack of family support 41, resistance from grandmothers, and cultural aspects that hinder the adoption of KMC 42,43.
Conclusions
The KBM technique significantly enhanced mothers' responsiveness to their infants' discomfort, thereby improving perceived self-efficacy compared to control mothers. The study revealed statistically significant differences between the groups over time [RTE (lower limit; upper limit) - Day 7: Control = 0.502 (0.437; 0.567) vs. KBM = 0.503 (0.426; 0.581); Day 14: Control = 0.564 (0.482; 0.640) vs. KBM = 0.719 (0.650; 0.776)]. Mothers in the KBM group reported higher scores on the perceived maternal-parental self-efficacy questionnaire at 14 days compared to those in the control group. Additionally, KBM strengthened family support (p < 0.05) without affecting perceptions of "being good at kangarooing." Thus, KBM serves as a nursing intervention that, when applied by mothers to their infants, effectively alleviates infant discomfort and enhances perceived maternal parental self-efficacy.
Mothers and families with preterm infants often experience fatigue and stress at home, and KBM emerges as an effective intervention to bolster maternal self-efficacy, thereby reducing barriers to adopting KMC. This study underscores the positive impact of the KBM technique, grounded in Barnard's theory, and underscores the importance of ongoing research to further enrich nursing practices.

