











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
It has been found that the estimated prevalence of diabetes mellitus (DM) in Mexico is 12.1% (Romero-Martínez et al., 2019) and only 53.6% of the people afflicted with the disease take preventive measures to avoid or delay complications (Hernández et al., 2016). HbA1c is the most important indicator for T2DM control (Pereira et al., 2015). It measures the average level of glucose or sugar in the blood during the last three months.
Several psychological interventions to control T2DM conducted in Mexico were analysed by González-Cantero and Oropeza-Tena (2016), who identified that these studies had not (or only partially) fulfilled Consolidated Standards of Reporting Trials (CONSORT), particularly those related to internal validity.
Cognitive behavioral therapy (CBT) has been efficacious in solving health problems (Hofmann et al., 2012). It particularly has been proven useful for people with diabetes mellitus (DM) to develop self-care, adherence to treatment, identification of barriers, and facing stressful situations, which are needed to achieve control of T2DM (Taylor, 2007). But, as it was mentioned, the effects are not lasting as measured in follow-up.
From the perspective of positive psychology (PP) it is necessary to focus on enhancing positive indicators (Seligman & Csikszentmihalyi, 2000) that could help maintain adherence to treatment and consequently achieve the results of interventions in the long-term. Interventions developed based on this perspective have broad evidence of its efficacy (Carr et al., 2023). Thus, for this study, psychological capital (PsyCap), a construct of the theoretical framework of positive psychology, was adopted. PsyCap is formed by four resources: self-efficacy, hope, resilience, and optimism. It was defined by Luthans et al. (2007, p. 3) as
The positive psychological state of development of an individual that is characterized by: 1) have confidence (self-efficacy) to take on and put the effort necessary to succeed in challenging tasks; 2) make a positive attribution (optimism) on succeed now and in the future; 3) persevere toward goals and when necessary, redirect the paths toward them (Hope) in order to achieve them; and 4) when beset by problems and adversity, maintained and retrieved and even beyond (resilience) to achieve the goal.
It is considered that the elements that make up the PsyCap could influence proactive and persistent behaviour of the person so that they can control their disease. For example, González-Cantero et al. (2017) conducted a study, in which the aim was to identify the relationship between the PsyCap and lifestyle of Mexican university students. There they found that the PsyCap explains 33.3% of the total variance of the lifestyle (R2 = .333). This result suggests that self-efficacy, hope, resilience, and optimism promote people to have a healthy diet, activity and/or exercise regularly, go to preventive medical check-ups, among other healthy behaviours that people with T2DM require. The purpose of this study was to develop and evaluate the feasibility of a positive and cognitive behavioral intervention to control HbA1c for people with T2DM in primary health care in Mexico.
Method
Design of the study
The current intervention is a case series design. There was a pre-test and a post-test with a three-month follow-up.
Description of the sample
Eleven (n = 11) patients with T2DM, (eight women and three men) from two primary health care institutions which approved the protocol for the study, participated in the study. They were recruited with an ad posted in sites of primary healthcare interest. Written informed consent was obtained prior to data collection; participants did not receive any compensation. Eligibility criteria included adults who: 1) had ≥ 1 year with the diagnosis of T2DM; 2) were of legal age (≥ 18 years); and 3) were literate. Adults with comorbidities, cancer or chronic renal disease, or major psychiatric illness were excluded. Participants who did not attend the 12 sessions, did not answer 100% of the questionnaire’s questions, or not to provide clinical study of HbA1c, were excluded from the study.
Thirteen participants met the inclusion criteria and were invited to participate, out of which two declined to participate because of lack of interest. Six were randomly assigned to the experimental group (EG) and five to the control group (CG) by flipping a coin (heads: control; tails: treatment). The CG was a wait list control group, which is a group of participants who do not receive the experimental treatment but are put on a waiting list to receive it.
The participants of the experimental group completed the 12 sessions, showing good adherence to treatment, since they carried out all the activities in each session.
Measurements
Questionnaire of Sociodemographic and Disease Variables. Designed specifically for this research, this questionnaire was used to obtain demographic data and register HbA1c percentage which was obtained through laboratory analysis.
Diabetes Treatment Self-Efficacy Instrument. This tool was designed and validated by Del Castillo (2010) in a sample of 240 persons with T2DM. It is composed of 14 items, each one with four response options ranging from “I feel very capable” to “I do not feel capable”. It assesses three dimensions: 1) self-efficacy in the follow-up of the food plan, 2) self-efficacy in the realization of physical activity, and 3) self-efficacy in the consumption of oral medication. Cronbach’s alpha for the overall scale is .83, .78 for the factor self-efficacy in the follow-up of the food plan, .80 for the factor self-efficacy in the realization of physical activity, and .63 for the factor self-efficacy in the consumption of oral medication.
Adult Hope Scale. Designed by Snyder (1995; 2002), it has 12 items and measures two factors (agency and pathways) using a Likert-type scale ranging from 1 “totally false” to 8 “totally true”. The agency factor consists of items 2, 9, 10, and 12 and pathways consist of items 1, 4, 6, and 8; the rest are distractor items. The total hope score is obtained from the sum of the items that make up the two factors mentioned above. The scores obtained can range from 8 to 64. Snyder (2002) pointed out Cronbach’s alpha ranging from .74-.88 for the overall scale, and .70-.84 for the agency factor and .63-.86 for the pathways factor.
Mexican Resilience Scale (RESI-M). This instrument was developed by Palomar and Gomez (2010). It consists of 43 items marked on a Likert-type scale ranging from 1 “totally disagree” to 4 “totally agree”. It has five factors: 1) Strength and Confidence in Himself, 2) Social Competence, 3) Family Support, 4) Social Support, and 5) Structure. Cronbach’s alpha for the overall scale is .93, .92 for Strength and Confidence in Himself, .87 for Social Competence, .87 for Family Support; .84 for Social Support and .79 for Structure.
Life Orientation Test (LOT). This instrument was created by Scheier et al. (2001) and validated in Mexico by Palomar et al. (2011). It contains 10 items (6 nouns and 4 fillers) marked on a 4-point Likert-type scale ranging from 1 (strongly agree) to 4 (strongly disagree). It assesses two factors: 1) optimistic attitude to life and 2) pessimism. In the validation study of Palomar et al. (2011) Cronbach’s alpha for optimistic attitude to life was .78 and for pessimism .45.
Procedures
Intervention proposal
The intervention was conducted from March 2016 to January 2017. It was applied by a health psychologist with master’s degree. A treatment manual was created for the intervention. In each session video and audio were recorded to evaluate adherence to treatment manual by two independent health psychologists with experience in treatment in chronic illness and its adherence.
Each session lasted for 90 minutes and had individual and weekly periodicity. Each one begun with a brief ‘check-in’ conversation period to allow for health psychologist-participant rapport-building. The session began with an introduction to the topic, the objectives, and materials, and a mood-state evaluation through a visual analogue scale. For treatment sessions, the review of the previous week’s home practice and self-records, including a discussion of successes or difficulties, was carried out. Thereafter, the health psychologist showed the technique(s) and gave examples of its application, followed by an interactive practice, and finally discussing home practice. In each session, the participants received the material.
The intervention consisted of 12 sessions. It had four phases: 1) Admission-evaluation contemplated in the first session where the outcome variables were evaluated. 2) Treatment contemplated from session 2 to 9; where the health psychologist intervened based on the treatment manual. 3) Post-treatment was carried out in session 10; where the outcome variables were re-evaluated. 4) Session 11 consisted of follow-up at one month, and session 12, at 2 months. The purpose of sessions 11 and 12 was to evaluate the maintenance of the benefits of the intervention and / or to solve problems. All the outcome variables were re-evaluated in session 12.
Intervention content
A multi-skill approach was selected for this study, as its efficacy has been pointed out (Schueller, 2010): people respond to and adopt techniques that they are interested in, attracted to, and willing to spend time practicing. This is supported by the meta-analysis by Sin and Lyubomirsky (2009) that reported multiple component interventions to be more effective than those that focus on a single technique. Therefore, in the present study, techniques of CBT and PP, particularly to increase PsyCap, were combined to develop skills for control of HbA1c. It was realized as a clinical health psychology intervention (Marks, 2009), abiding by the recommendations of CONSORT and TREND statements (Marks, 2010), particularly those related to internal validity factors. The program, intervention, and technique levels are shown in Figure 1. The topics covered in the intervention were as follows: healthy eating, physical activity, assertive skills for rejecting unhealthy foods, self-efficacy, hope, optimism, and resilience.
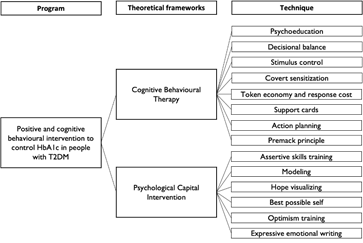
The following is a brief description of the techniques used.
Psychoeducation. This technique is used to provide information on how psychological aspects operate in relation to some topic (Suzuki & Tanoue, 2013).
Decisional balance. It is a technique by which people compare the benefits versus the costs of performing some behavior (Miller & Rose, 2013).
Stimulus control. This technique consists of eliminating or adding those stimuli that are provoking or preventing the participant from executing a specific behavior that needs to be eliminated or established to achieve something (Sidman, 2008).
Covert sensitization. It is a technique in which neither the undesirable stimulus nor the aversive stimulus is presented only in the imagination with the intention of creating an avoidance response to the undesirable stimulus (Cautela, 1967).
Token economy and response cost. This technique sought to encourage the participant to give himself reinforcers (rewards, rewards, gains) for what he did well and to administer punishments (response cost) when he did not fully achieve his eating objectives (Kazdin, 1977).
Support cards. It consists of the participant writing on a small piece of paper the benefits of performing an activity so that when he/she has trouble or apathy in performing the activity, he/she will remember that it is beneficial (Beck, 2009).
Action planning. Action planning is a process that occurs after a decision has been made to do something. It is directed towards a goal, specifies when, where, and helps to identify signals in the favorable direction of achieving the goal (Sniehotta et al., 2005).
Premack principle. The use of this principle implies that a less desired behavior may be reinforced by the opportunity to perform a more desired behavior (Premack, 1959).
Assertive skills training. According to Rich and Schroeder (1976, p. 1085) assertiveness training comprises “hierarchical presentation of stimulus situations, operant shaping, constructive criticism, role play, role reversal, response playback, response practice, homework, postural and vocal analysis training, exhortation and lecturing by the therapist, modeling, relaxation, fixed role therapy, exaggerated role taking, instructions, coaching, external reinforcement, and self-reinforcement”.
Modeling. Based on the principle of vicarious learning, the technique consists of the person observing a model or models performing the behavior to be acquired (Bandura, 2016).
Hope visualizing. The technique consists of the person establishing goals, identifying the ways to achieve them and the obstacles to be overcome so that he/she can then generate alternative solutions and proceed with the achievement of the objective (Snyder, 1994).
Best possible self. In this technique the participant is asked to imagine their best possible future over the next five years with respect to their life (in their family, work, school, etc.) and consider how to make that future a reality (King, 2001).
Optimism training. The participant is trained to analyze a situation based on the following questions: what is the worst and best that can happen; what the most realistic alternative is; what I should do to make the worst happen; and what should I do to make the best happen. The basis of this technique assumes an identification of the ABC (Adversity, Belief and Consequence) (Seligman, 2014).
Expressive emotional writing. This technique basically consists of writing about a traumatic event for 15 minutes on four occasions with indications so that the participant expresses the emotions caused by the traumatic event and analyzes the causes and emotions of the event so that instead of complaining, he/she can look for a possible direct solution to the problem (Pennebaker & Evans, 2014).
Statistical analyses
The IBM SPSS Statistics 26 software was used for statistical analysis. The analysis consisted of three stages: 1) analysis of homogeneity, 2) Wilcoxon test for related samples (from pre-to post-test, post-test to follow-up, and pre-test to follow-up) for the outcome variables and 3) Hedges' g to evaluate the effect size, related to clinically significant changes.
Ethical considerations
The present research was subject to the guidelines established in the Ley General de Salud (Título Quinto “Investigación para la Salud” Article 100). In addition, all the corresponding points of the Código Ético del Psicólogo issued by the Sociedad Mexicana de Psicología and the Consejo Nacional para la Enseñanza e Investigación en Psicología were considered. Then, was reviewed and approved by the Comité de Ética de la Facultad de Psicología of the Universidad Michoacana de San Nicolás de Hidalgo (Reference Number 005).
Results
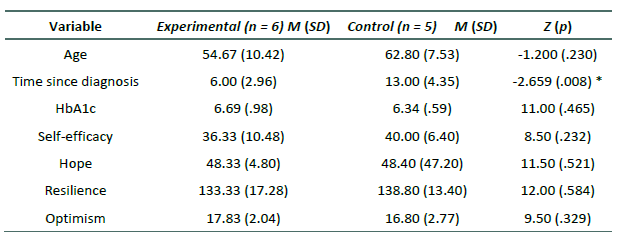
According to the analysis of homogeneity through χ2 and Fisher's exact, there were no statistically significant differences in the following variables: sex (p = 1.00); marital status (χ2 = 3.438, p = .179); T2DM complications (p = .061); and comorbidity (p = 1.00), that is, both groups were homogeneous. The only variable in which differences were identified, was in the time since diagnosis (Z = -2.659, p = .008) as shown in Table 1.
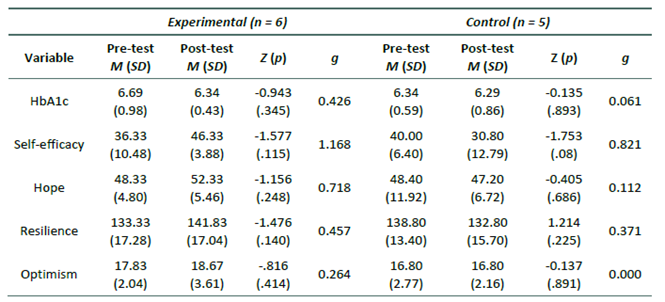
Despite not having statistically significant differences in HbA1c between pre-test and post-test, there was a favourable moderate improvement (g = 0.426) in EG (see Table 2). Self-efficacy in EG had a high favourable improvement (g = 1.168) from pre-test to post-test as shown in Table 2, but no statistically significant differences were identified. A high deterioration in self-efficacy was identified (g = 0.821) in the CG.
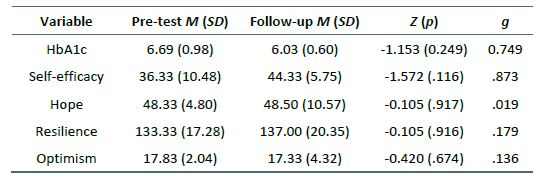
In the EG, there was a high and favourable improvement in HbA1c (g = 0.749) from pre-test to follow-up, as shown in Table 3. Regarding the EG, in the analysis from the pre-test to the follow-up, no statistically significant changes were found in psychological variables associated with control of T2DM. However, a high and favourable improvement remained on self-efficacy (g = 0.873).
Discussion and conclusion
The purpose of this study was to develop and evaluate a positive and cognitive behavioral intervention to control HbA1c for people with type 2 diabetes in primary health care in Mexico.
It was found that the intervention, as a pilot intervention, reflected a high clinically significant improvement in HbA1c and in self-efficacy, after the intervention and at follow-up, in the patients who were a part of the EG. The moderate and favourable improvements in HbA1c obtained in this study from the pre-test to the follow-up coincide with other studies conducted in Mexico (Hattori, 2014; Montes et al., 2013); the effects of cognitive behavioral interventions were clinically favourable, but not statistically significant most likely due to the size of the sample, 11 in this study, eight and 12 in the studies mentioned above, respectively. The high rate of improvement from pre-test to follow-up in HbA1c obtained in this study coincides with studies done by Safren et al. (2014) and Weinger et al. (2011) but contrasts with studies which report that the favourable effects of the interventions on the percentage of HbA1c decline in the immediate follow-up to the post-test (García & Sánchez, 2013; Quiroga, 2012).
In this study, all PsyCap variables in the EG increased in the post-test compared to the CG, in which only self-efficacy increased but to a lower level than that of the EG.
Studies have found that personal control is associated with better glycemic control (Martinez et al., 2017); therefore, in this study it was observed that the intervention had a favourable improvement in HbA1c and self-efficacy. Furthermore, this was like the results of other studies (Del Castillo, 2010; García & Sánchez, 2013) in which self-efficacy increased in post-test, but then decreased in follow-up, even though the decline was less.
The above could be explained by the fact that self-efficacy improves self-care practices, consequently improving the control on diabetes (Ali, 2017; Johnson et al., 2013). Thus, one of the strengths of this study is that it increased and maintained self-efficacy of the participants through intervention strategies. One strategy that was particularly effective was self-efficacy social comparison, which if supported can strengthen self-efficacy in individuals with T2DM (Arigo et al., 2018).
Regarding hope, there are not many studies with an experimental approach involving people with T2DM that focus on the impact on HbA1c. Nevertheless, there is evidence that hope can be increased in people with DM (Ghazavi et al., 2015) and be useful for mood status (Khaledi-Sardashti et al., 2018).
It has been found that resilience is associated with self-management of T2DM (Wilson et al., 2017). In this study, resilience increased moderately in the EG with only one session, which is consistent with the study by Bradshaw et al. (2007) whose purpose was to train people with DM on resilience. They found that those who received this treatment increased their physical activities and had a better control over their HbA1c compared to those who only received education about the disease. Additionally, as Ryan et al. (2019) pointed out, resilience training is a promising means to strengthen resilience and related protective factors and improve mental health in people with DM.
Regarding optimism, a study by De Ridder et al. (2004) indicated that optimism contributes to the maintenance of self-care behaviours in patients with T1DM up to 6 months; however, they suggest studying the effects of the optimism variable considering the strategy used, since there are different techniques, some of which may not achieve the same effects, thus learning how optimistic beliefs of self-care can help control the disease. This could explain why optimism in this intervention did not increase despite using the best possible exercise. Thus, it is necessary to try other strategies to increase optimism or similar variables that allow people to develop a positive perspective so that they feel motivated to achieve their goals. An alternative may be mental contrasting, which was shown in a study by Adriaanse et al. (2013), using which participants with T2DM had improved their diabetes self-management to a larger extent than participants who merely imagined a positive future how it is done in the best possible exercise.
(PP) interventions complement the clinical work of health psychologists (Rashid, 2009). Thus, this study is one of the first in Mexico where a combination of CBT with elements of PP at the intervention level was addressed. Furthermore, this research was carried out based on various criteria of methodological control that impacted other interventions, for instance, random assignment of participants to the experimental or control groups, video recording to assess adherence to the delivery of interventions by the psychotherapist. This represents a contribution for the health professional who works with people with T2DM.
This research achieved results like interventions with a greater number of sessions (Pantoja-Magallón et al., 2011; Riveros et al., 2005; Rodríguez et al., 2013; Ybarra et al., 2012). This can be attributed, as Riveros et al. (2005) point out, to the individual nature of the intervention.
In this study, participants performed specific techniques and strategies to develop behaviour-specific self-efficacy for diet, physical activity, and self-care, which has been suggested to be beneficial (Steed et al., 2014; Mohebi et al., 2013). Moreover, the results of this study suggest the importance of replicating the present intervention, with a larger number of patients, to analyse the results in HbA1c.
One of the limitations of the present study is that the evaluation of the three-month follow-up could not be performed in the CG. As this was a pilot study, future research needs to develop controlled studies with larger sample sizes and long-term follow-up (Kanapathy & Bogle, 2017).

