











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Acute pain in pediatric patients elicits a stress response that can have a deleterious effect on neurological, emotional, and behavioral development. Historically, opioids have been used to treat postsurgical pain; however, they can lead to a myriad of side effects, including apnea, sedation, hypotension, gastric motility dysfunction, tolerance, and withdrawal. Regional anesthesia techniques are gaining traction in a multimodal pain management approach to decrease opioid use and provide effective analgesia. Fascial plane blocks are replacing neuraxial methods (caudal) for postoperative analgesia due to ease of use with ultrasound guidance and increased duration of action.1 Emerging literature2 supports the feasibility, efficacy, and safety of pediatric regional anesthesia in the hands of experienced practitioners. The quadratus lumborum fascial plane block (QLB) is one of the more recently described truncal blocks that provides analgesia over a large truncal plane. The QLB provides effective truncal sensory blockade from dermatomal levels T6 to T12 for abdominal surgery. The QLB has been well described in the adult literature as well as the pediatric surgical literature. 3 To date, there is limited description of its use and efficacy for pediatric patients undergoing upper abdominal urologic surgery. 1,4 Herein we present a case series examining the use of the QLB for postoperative pain management in pediatric patients undergoing upper tract urological surgery via flank incision.
Methods
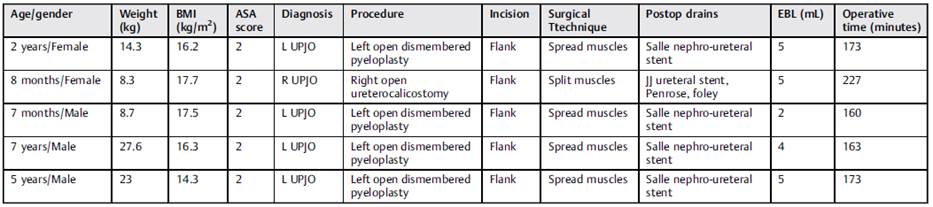
Following approval from the Institutional Review Board, the electronic medical record from our institution was queried from August 2019 to August 2020, to identify pediatric patients aged between 0 and 17 years who underwent open upper urinary tract surgery via a flank incision. Patients undergoing upper urinary tract surgery via a laparoscopic approach were excluded due to the different incisions used in laparoscopy. All patients undergoing open upper urinary tract surgery during the defined study period were offered and consented to undergo a QLB. Five patients were identified (Table 1).
Upon induction of general anesthesia, patients received fentanyl IV (1 mcg/kg) and acetaminophen IV (15mg/kg) during the operation. After induction, a posterior QLB was performed. Patients were placed in position for their pyeloplasty, as dictated by the surgeon, and the skin site was prepped. A high-frequency (4.2-13 MHz) linear ultrasound probe was placed transversely in the midaxillary line to visualize the muscular plane and moved posteriorly until the aponeurosis of the transversus abdominis became visible and the quadratus lumborum (QL) muscle was identified. Using an in-plane approach, a 22-gauge, 50-mm echogenic needle was inserted and advanced posteriorly to the interfacial plane between the QL muscle and the thoracolumbar fascia (Fig. 1). Hydrodissection was performed to confirm needle position and, after negative aspiration, a single injection of 0.5mL/kg of either 0.25% or 0.5% ropivacaine. (concentration chosen at practitioner's discretion) with 1mcg/kg of clonidine was administered (Fig. 1).
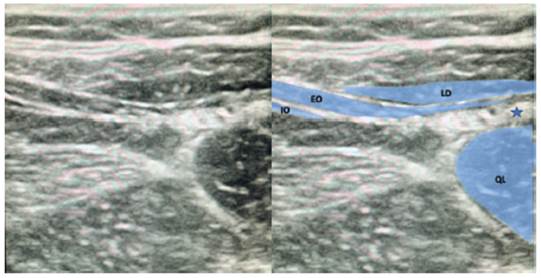
Figura 1 Ultrasound image of the anatomical structures and local anesthetic injection point for posterior QLB. Abbreviations: EO, external oblique muscle; IO, internal oblique muscle; LD, latissimus dorsi muscle; QL, quadratus lumborum muscle. Note: Injection point.
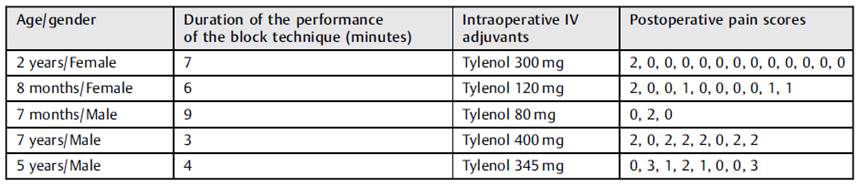
Per hospital protocol, postoperative pain scores were obtained every 20 minutes in the postanesthesia care unit (PACU) and every 4 hours on the inpatient floor according to age-appropriate 10-point scales (Children's Revised Impact of Event Scale [CRIES] for patients aged < 1 year; Face, Legs, Activity, Cry, Consolability [FLACC] for those aged between 1 and 5 years; and the Wong-Baker Faces Pain Rating Scale [FACES] for patients aged between 5 and 8 years) (Table 2). Postoperative pain was managed with oral acetaminophen and ibuprofen. Oral narcotics were available for break-through pain scores > 4.
Results
From August 2019 to August 2020, 2 pediatric urologists within a single quaternary care institution performed a total of 12 upper urinary tract surgeries for management of primary or secondary obstruction of the ureteropelvic junction. Of these cases, five patients submitted to open flank surgery who underwent a preoperative unilateral QLB were identified. No QLB had to be aborted or crossed over to an alternative block. The performance of the block technique took less than ten minutes for all patients. All patients had either an internalized JJ ureteral stent or Salle nephroureteral stent. One patient had a postoperative foley catheter and Penrose drain.
The average postoperative pain score during the admission was 1, with the lowest being 0 and highest, 3. All blocks were considered successful because no patient required narcotics in the postoperative period. The average length of stay was of 0 to 1 day. No complications (such as hypertension, infection, hematoma) or technical difficulties associated with the regional QLB were identified.
Discussion
The present series supports the notable trends demonstrated elsewhere toward the use of regional anesthesia. The transversus abdominus plane (TAP) block has been described for pediatric abdominal surgeries, but the comparison by Lorenzo et al. 5 of the TAP block to surgeon-administered infiltration in children undergoing pyeloplasty was equivocal. The QLB is a fascial plane block that provides sensory blockade from T6 to L1 with a single injection. The levels for a typical flank incision, as used in the present series, would be dermatomal levels T7 to T10. In comparison to the TAP block, Öksüz et al. 6 describe that the QLB provides longer and more effective postoperative analgesia compared with the TAP block for children undergoing lower abdominal surgery. The QLB has been found to be equivalent to the erector spinae plane block for pediatric abdominal surgery; however, the QLB was chosen due to the ease of performing it in the planned surgical position. 7 A transvertebral block was not considered by the surgical and anesthesia teams, as the duration of this block is shorter than that of the QLB, and, while low, potential risks associated with the technique are significant, such as pleural puncture and pneumothorax. 8 In the present series, we observed an average postoperative pain score of 1. The lack of response to the initial incision and the lack of need for narcotics following induction strongly suggest that dermatomes were not missed by the QLB, and that pain was adequately controlled.
Most regional anesthesia studies decrease the concentration of the ropivacaine used in fascial plane blocks to increase the volume that can be utilized, but this may sacrifice block density. The deposition of a high volume and high concentration of local anesthetic solution posterior to the QL muscle in the middle of the thoracolumbar fascia provides a dense truncal block, while the addition of clonidine prolongs the duration of the block. 9,10 In the present case series, the local anesthetic concentration injected for the procedure was increased, but within standard maximum dosing guidelines according to patient weight. Utilizing such dosing with the pediatric patient population enables the performance of an opioid-sparing technique, potentially leading to a denser blockade, and providing effective analgesia for 24 hours following surgery. The duration of the block could not be objectively measured in the present series, but it is described to have analgesic effects lasting up to 24 hours. Future studies will aim to assess the effect of varying local anesthetic concentration on pain control and durability after QLB, as well as whether the block may be optimized with the addition of alternative adjuncts such as dexmetomidine. 11
The limitations of the present case series include its small sample size and retrospective nature, which is inherent to this type of study. The small number of cases identified during this one-year period is likely directly related to the onset of the COVID-19 pandemic in March 2020, the midpoint of the period reviewed, which negatively impacted both patients interacting with health care and the availability of operating rooms to the surgeons involved in the present study. Additionally, there was varied dosing concentrations used for the blocks, as well as multiple practitioners performing the blocks in a non-standardized fashion, all of which may have introduced bias in the observed results.
Despite its limitations, the present series serves to demonstrate the feasibility of performing QLBs in this patient population. Future randomized, controlled studies are needed to establish the efficacy of pain control for QLB versus infield surgeon-administered infiltration, as well as the optimal local anesthetic concentration and volume, and potential added benefits from the use of local anesthetic adjuvants.
Conclusion
The present case series demonstrates the utility of the QLB in minimizing narcotic requirements for pediatric patients undergoing upper abdominal urological surgery, both intraoperatively and postoperatively. Randomized, controlled studies are necessary to compare the efficacy of the QLB versus surgeon-administered infiltration for upper abdominal surgery in pediatric patients, as well as to determine effective dosing and use of adjuvants.

