











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Rhabdomyolysis is a clinical and paraclinical syndrome characterized by the presence of skeletal muscle necrosis that leads to the consequent release of intracellular muscle components (myoglobin, creatinine kinase (CK), aldolase, lactate dehydrogenase, and electrolytes) into the systemic circulation (1). Clinically, it has a variable presentation, ranging from the spectrum of asymptomatic elevation of creatinine kinase levels, myalgia, marked elevation of enzyme markers, myoglobinuria, macroscopic pigmenturia without hematuria, to severe complications that put life at risk such as acute kidney injury, electrolyte imbalance, arrhythmias, myocardial or liver dysfunction, disseminated intravascular coagulation (DIC) and even death (2-5). The main cause is a severe direct traumatic injury or crushes injuries; however, other conditions such as infections, intoxication, muscle ischemia, neuroleptic malignant syndrome, malignant hyperthermia, metabolic disorders, and genetic pathologies can also cause it, and particularly the extended rest or immobilization (1-3, 6) or strenuous exercise as one of the etiologies that can cause it (7-9). Rhabdomyolysis secondary to strenuous exercise is defined as the presence of some of the diagnostic criteria described, namely
1.An elevation of CK 12 to 36 hours after exercise, with a maximum at 3-4 days, followed by normalization within several weeks of rest
2.The increase in CK is preceded by exercise, generally beyond the limits of fatigue, also known as "unaccustomed physical exertion" or "involuntary exertion”
3.Symptomatic CK elevation with any of the following: myalgia (muscle pain or tenderness; rhabdomyolysis is generally very painful), swelling and/or weakness
4.The presence of myoglobinemia and/or myoglobinuria: either by inspection (pigmenturia) or by laboratory tests. Since the blood or urine myoglobin test is not widely available, many experts consider the combination of the first three diagnostic features to define exercise rhabdomyolysis (8-9). This condition may be the first manifestation of a genetic muscle disease that reduces the exercise threshold to develop muscle rupture and this possibility should be considered in the event of recurrent episodes (high creatine kinase (CK) levels (> 50 × upper limits of normal) or persistent hyperCKaemia; absence of unaccustomed exercise; absence of drugs (recreational or medical); or positive family history of rhabdomyolysis or other symptoms of exertion).9
Case report
In this case report, we present a patient with a picture of rhabdomyolysis with severe elevation of muscle enzymes and secondary acute kidney injury who was subsequently documented.
Our case is a 32-year-old man, with no relevant history, who consulted for symptoms of abdominal, lumbar, and thigh region pain, associated with changes in color in the urine of several hours of evolution. During the interrogation, as additional data, he reported that he had performed extreme physical activity (CrossFit) 2 days earlier with intense work on the lower limbs, which he was not familiar with, given that he had not performed a physical activity of this intensity for a long time.
He did not report the consumption of nutritional supplements. In the clinical evaluation at admission, he was hemodynamically stable, with mild pain on palpation of the abdominal flanks, without signs of acute abdomen, negative renal percussion, and pain in the thigh region. Blood and urine tests revealed: hemogram with normal cell count, hemoglobin 15.2 g/dL, hematocrit 42%, normal volumes, urinalysis: density: 1.005, pH: 5, proteins 150 mg/dL, blood 250 Ery/c, normal glucose, negative ketone bodies. Creatinine 1.56 mg/dL, urea nitrogen (BUN) 12.6 mg/dL, GRF 57.9 mL/min/1.73m2 (CKD-EPI). Rhabdomyolysis was suspected, thus, hydration with intravenous fluids was initiated and requested complementary tests showed: total CK 189,000 U/L, AST 3,185 U/L, ALT 589 U/L, PT 10.6 sec, INR 1.04, PTT 29 sec, potassium: 4.2 mmol/L, ionic calcium 1.18 mmol, total bilirubin 0.42 mg/dL, direct 0.26 mg/dL, abdominal ultrasonography and chest X-ray within normal limits.
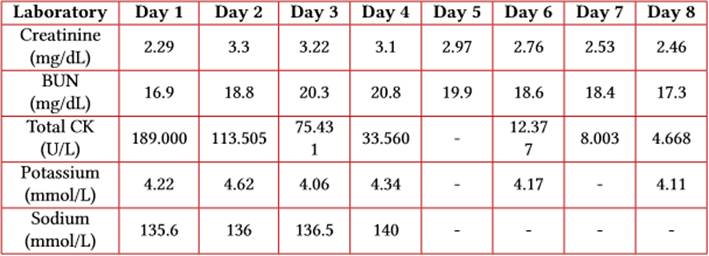
After the assessment by the internal medicine service with diagnoses of rhabdomyolysis, AKIN 2 acute kidney injury, and liver injury, a decision was made to transfer to the intensive care service (ICU). Management of intravenous water therapy was adjusted, bicarbonate was added, and control tests were requested (Table 1). The nephrology service identified acute kidney injury AKIN 3 and ordered an increase in venous fluids for a target diuresis between 200-300 mL/h. During his stay in the ICU, the patient had a favorable evolution, diuresis within the proposed limits, with no need to initiate renal support therapy, and a gradual decrease in creatinine and transaminase values. Hospital discharge was given with an outpatient follow-up order by the nephrology service.
Discussion
One of the biggest challenges in diagnosing exertional rhabdomyolysis is the fact that serum CK levels will normally rise naturally after strenuous exercise, potentially up to 10 times the upper limit of normal (9). Increased CK levels also vary widely among patients (10), and exposure to high temperatures and humidity during exercise may also play a role in higher rates of rhabdomyolysis according to reports in the literature (11). A retrospective cohort study published in 2010 reported 22.2 cases of exertional rhabdomyolysis per 100,000 military personnel per year, with a low incidence and risk of exertional recurrence among young people (12).
The genetic disorders most frequently described in this clinical setting are disorders of glycolysis or glycogenolysis, including McArdle's disease, Tarui disease, LDH deficiency, and debranching enzyme, lipid metabolism disorders, including deficiency of CPT I and II, long-chain acyl-coenzyme A DH deficiency, medium-chain acyl-coenzyme A DH deficiency and thiolase deficiency, increased susceptibility to malignant hyperthermia, including familial malignant hyperthermia, Duchenne and Becker muscular dystrophies and myotonic dystrophy. Other genetic conditions include Krebs cycle disorders, mitochondrial respiratory chain disorders, G6PDH deficiency, and myoadenylate deaminase deficiency (1).
Clinically, it is manifested by a triad of symptoms: myalgia, weakness, and myoglobinuria. However, this rigid description of symptoms is only present in <10% of patients (13). The hallmark of rhabdomyolysis is the presence of elevated CK levels (these are usually at least five times the upper limit of normal, but range from approximately 1,500 to more than 100,000 international units/L). Levels begin to rise 2 to 12 hours after the onset of muscle injury and peak within 24 to 72 hours. Typically, a decrease is seen within three to five days after the muscle injury ceases. CK has a serum half-life of about 1.5 days and decreases at a relatively constant rate of about 40 to 50% of the previous day's value (3). Elevated CK levels are the most sensitive laboratory test to assess muscle injury (9, 13). In patients whose CK does not decrease as expected, there may be ongoing muscle injury or the development of compartment syndrome (1-3).
The other characteristic finding is the reddish-brown urine of myoglobinuria, but since this can be observed in only half of the cases, its absence does not exclude the diagnosis. 9,14 Myoglobin is rapidly excreted in the urine when the plasma concentration exceeds 1.5 mg/dL. Visible changes in urine only occur once urine levels exceed approximately 100 to 300 mg/dL, although they can be detected with the urine test strip (orthotolidine) at concentrations as low as 0.5 to 1 mg/dL (15). Myoglobin has a half-life of only two to three hours, much shorter than that of CK. Due to its rapid excretion and metabolism to bilirubin, serum levels can return to normal within six to eight hours. Therefore, it is not uncommon for CK levels to remain elevated in the absence of myoglobinuria (1, 2). In rhabdomyolysis, myoglobin appears in the plasma before the elevation of CK occurs and disappears while CK is still elevated or increasing (1). Routine urine tests for myoglobin by urine dipstick evaluation may be negative in up to half of the patients with rhabdomyolysis (1-3). It is estimated that 10%-40% of patients with rhabdomyolysis develop acute kidney injury (9, 13, 14, 16).
Routine laboratory tests, including complete blood count (CBC), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), kidney function and urinary sediment vary greatly depending on the underlying cause of rhabdomyolysis and its severity (1, 2, 9). Elevation of serum aminotransferases is common at the expense of aspartate aminotransferase (AST) in cases of rhabdomyolysis in which CK was greater than or equal to 1000 units/L (17). Electrolyte imbalance may be present, especially severe hyperkalemia that leads to the development of arrhythmias, putting the patient's life at risk (1-3). Hyperphosphatemia, hypocalcemia, high anion gap metabolic acidosis, and the development of severe hyperuricemia are other manifestations that can be found. Later complications include acute kidney injury, compartment syndrome (intracompartmental pressure is> 30 mmHg), and, rarely, disseminated intravascular coagulation (1-4, 18, 19).
Acute kidney injury is a common complication of rhabdomyolysis, it is the result of the accumulation of myoglobin, which is nephrotoxic in the kidney, and its presentation varies between 15% and 50% (4). The risk of AKI is greater when CK levels are in the greater range of 15 to 20,000 units/L, there is the presence of coke or dehydration, sepsis, and acidosis (3, 4). The management of rhabdomyolysis aims to avoid acute kidney injury, since this condition leads to an increase in adverse clinical outcomes (4), through early hydration with crystalloids at a rate of 1.5 L/h (20), to maintain urinary output of 200 ml/h, urinary pH> 6.5 and drink reaches a plasma pH <7.5 (1). Alkalinization of urine with sodium bicarbonate has no conclusive evidence (21). Early recognition of rhabdomyolysis is required, as well as an adequate differential diagnosis and timely treatment of the specific causes, including the intervention of complications to positively impact the results (1).
We present a case report of a patient with a rhabdomyolysis with a severe elevation of muscle enzymes and secondary acute kidney injury who was subsequently documented (initial Total CK 189,000 u/L) after extreme physical activity (CrossFit), who developed multiple complications and the need for support in the Intensive Care Unit (ICU) with satisfactory outcome.

